
Abstract
Aim
The well-documented association of reductions in physical activity with age is based largely on cross-sectional studies that do not distinguish between prevalence of physical activity and initiation/discontinuation patterns. These studies also fail to consider the changes in physical activity as a function of life stage. We investigated how physical activity evolves over a lifetime. We distinguished between prevalence and initiation/discontinuation patterns and also considered multidirectional age effects.
Subject and methods
The analyses are based on the annual German Socio-Economic Panel survey, which originally involved 6,000 households (>12,000 individuals) from age 16. Our study included 3,487 subjects (West Germany), i.e., 33% of the individuals first interviewed in 1984. A survival analysis model was constructed to assess the simultaneous effect of age and generation, while adjusting for potential confounders.
Results
The results show that the ubiquitous differences in physical activity between age groups are mainly attributable to cohort differences, not age effects. The likelihood of initiating at least weekly physical activity declines with age, as does the likelihood of discontinuing an established exercise habit. Both trends are more readily explained by changes in occupational and family biography than by health and fitness.
Conclusion
The ubiquitous differences in physical activity between age groups are largely due to intergenerational differences.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Physical activity is a key factor in preventing cardiovascular disease, osteoporosis, diabetes, chronic disease, some types of cancer, and other diseases of the elderly. Physical activity also retards the aging process (World Health Organization 2003). The role of physical activity differs with age. Most fitness trends primarily pertain to the younger half of the population. Physical activity is much less prevalent among the elderly, i.e., those who would stand to achieve the greatest benefits from physical activity from a health point of view (Bijnen et al. 1998; Brach et al. 2004; Patel et al. 2006; Hollmann and Hettinger 2000). Age-related and biography-related differences in leisure-time physical activity participation are documented in numerous studies (Boutelle et al. 2000; Brändle et al. 1999; Dai et al. 1990; Lim and Taylor 2005; Sallis et al. 1989; Ruchlin and Lachs 1999; Schneider and Becker 2005; Shaw et al. 2010; Sternfeld et al. 1999) and it seems obvious at first glance that both physical performance and the extent of physical activity decline in the life course.
Studies available to date on the effect of aging on physical activity fail to address key questions, however. For instance, the apparent fact of an age-related reduction in physical activity is based almost entirely on cross-sectional studies comparing physical activity of different age groups at a specific point in (calendar) time, i.e., in cross section. However, different age groups also belong to different birth cohorts, and little research has been done to investigate the extent to which differences in physical activity are actually due to age difference (e.g., differing levels of fitness) or can in fact be attributed to differences in birth cohort or generation (e.g., different socialization into sports). Physical activity is also affected by fashion and contemporary opinion—period effects—which are separate from age and cohort affiliation. Only recently have scientists come to realize that generation and period effects are factors co-determining the extent to which individuals are physically active (cf. Breuer 2005 and others). Yet it is still unclear how intergenerational differences in physical activity arise.
Declining prevalence of physical activity with increasing age cannot be interpreted unquestioningly as indicating that the number of people who discontinue physical activity simply increases with advancing age. Instead, declining prevalence may be the result of declining initiation below a level that counterbalances discontinuation.
This paper investigates life course changes in leisure-time physical activity among different birth cohorts and hence expresses inter-cohort differences. It differentiates in this process between prevalence and initiation/discontinuation behavior. The analyses also take a non-uniform age effect into account.
Explanatory mechanisms and empirical results generated to date
Declining physical performance
Physical activity is closely linked in people’s minds with health and physical performance, both of which decline with age.
However, the connections between physical activity and health are by no means trivial; their interaction is complex. It is true that leisure-time physical activity requires a certain level of physical performance, which is why healthy individuals are more likely to engage in physical activity. On the other hand, physical activity has a beneficial effect on health, with the result that people who exercise further improve and/or maintain their health more effectively (Byberg et al. 2001; Pfaffenbarger et al. 1993; Thune et al. 1998; Wannamethee et al. 1998; Wannamethee and Shaper 2001; Yang et al. 2008). The converse applies to non-exercisers, whose physical performance deteriorates more rapidly than that of their more physically active peers. This feedback mechanism helps consolidate a physically active—and, even more so—a non-physically active lifestyle. A logical consequence would be the polarization of lifetime physical activity. One implication of the polarization theory is a reduction in initiation of exercise among non-exercisers because the health barriers grow with time.
In this connection, a recent study by Shaw et al. (2010) shows that the transition to a continual decline in exercise in the life course precedes the decline in health/onset of health problems and functional deterioration. A steady decline in leisure-time physical activity begins as early as approximately 33 years of age. This early decline in leisure-time physical activity in the course of a lifetime is more likely attributable to diminishing free time as a result of professional and family commitments than due to health limitations (Shaw et al. 2010).
The interrelationship (between health and physical activity) is compounded however by the fact that the beneficial effects on health motivate people diagnosed with an illness to start exercising. For instance, exercise can reduce the risk of developing chronic illness in general (Pfaffenbarger et al. 1993; Byberg et al. 2009). A cardioprotective effect is attributed in this context to moderate endurance sports in particular (Sallis et al. 1989; Wannamethee and Shaper 2001; Katzmarzyk et al. 2003). Intervention studies demonstrate that physical endurance activities have an especially positive impact on individual cardiovascular risk factors such as hypertension and high blood lipids (Boardley et al. 2007; Kokkinos et al. 2001; Panagiotakos et al. 2003; Pescatello et al. 2004). Various health care players are increasingly encouraging elderly people to become more active, in many cases in response to medical advice (Blech 2006; Hubert et al. 2002; World Health Organization 2002). This effect counteracts a decline in initiation rate and slows down—maybe even (over)compensates for—any decline in physical activity with age.
This line of argument can be summarized by saying that changes in lifetime physical activity are due to deterioration in physical performance, which in turn suggests that the age effect must be much less apparent for people who maintain their health at a constant level, although a positive correlation between physical activity and health is amply documented (Erlinghagen 2003; Ruchlin and Lachs 1999; Sternfeld et al. 1999; Gregg 1996; Hirvensalo et al. 1998; Roberts et al. 2003; Meyer et al. 2004; Whaley and Ebbeck 1997).
Occupational and family demands
Leisure-time physical activity is also subject to opportunities and restrictions which change in the course of a lifetime. A number of influencing mechanisms are at work:
(1) Life circumstances determine the time budget available for leisure-time physical activity. The time potentially available for leisure-time physical activity depends on the amount of time required for paid employment, on partnership/family life situation, living situation, and daily mobility requirements. The time budget tends to be at its most limited for middle-aged adults with a job and family. (2) Furthermore, the physical demands of work inside and outside the home affect a person’s desire to engage in leisure-time physical activity. (3) The place of physical activity in a person’s life may also depend on the attitude toward physical activity of the person’s partner and significant others. (4) Finally, life circumstances co-determine which types of physical activity are accessible to a person. Crucial factors here include workforce membership, income, and—not least—size of place of residence; the latter concerns types of physical activity that depend on infrastructure (e.g., swimming pool, tennis courts, gym).
There is a paucity of empirical data on life stage dependency of leisure-time physical activity. The available data from empirical studies investigating the impact of life circumstances on leisure-time physical activity are contradictory in part. Some studies see a positive correlation between workforce membership and leisure-time physical activity (Sternfeld et al. 1999; Crespo et al. 1999) or no connection at all (Droomers et al. 1998); a negative impact is documented for women only (Mensink et al. 1997). With respect to job-related physical exertion, a difference between blue-collar and white-collar workers is well established (e.g., Lindström et al. 2001), and there is evidence of a direct negative correlation between manual exertion at work and leisure-time physical activity (Becker and Schneider 2005). As far as marital status is concerned, most studies indicate that marrieds take less exercise than unmarrieds, but the results are inconsistent overall (Boutelle et al. 2000; Sternfeld et al. 1999; Mensink et al. 1997; Ransdell and Wells 1998). Inconsistency also applies with respect to the existence of minor children in the household (Sternfeld et al. 1999; Bässler 1990). On the other hand, there are in fact several (albeit few) empirical studies indicating a more nuanced lifetime physical activity profile—specifically with respect to an increase in physical activity in the second half of life (Lindström et al. 2001)—which support the life stage dependency theory.
However, it is also reasonable to assume that, owing to differences in level of involvement, these occupational and family demands will vary in their impact on women and men in the relevant contexts.
Generational differences
Given that a lot of studies are based on cross-sectional data, most of the theories attempting to explain age differences in physical activity (declining performance, changing life circumstances) apply only if the observed differences between age groups are not in fact due to cohort differences. The case for cohort differences can be argued in several ways:
(1) Cohort differences might also be due to differences in physical performance between cohorts. Intergenerational variance in physical performance is implausible only at first glance. For instance, there is a growing acceptance that events and life circumstances in early childhood affect mortality (and, prior to that, state of health) in later adulthood (Barker 1998; Bengtsson and Lindstrom 2000; Costa 2000; Gavrilova et al. 2003). Against this background, it seems conceivable that early childhood deprivation is associated with lifelong impairment of physical performance, while the growing improvement in material life conditions for broad sections of the population in the post-World War II era is likely to be associated with continuous improvement of health in subsequent generations. This trend is congruent with the observation that the health of the elderly is improving in Germany and that active life expectancy has increased significantly (Dinkel 1999; Klein et al. 2002).
(2) Cohort differences in leisure-time physical activity might also be due to declining physical exertion in manual occupations as a result of technological progress, rationalization, and automation of production.
(3) Finally, differences in socialization may be another cause of cohort differences in leisure-time physical activity. According to this line of argument, older people would have engaged in less physical activity throughout their lives because of a lesser emphasis on leisure and leisure-time activities during their youth; it is only in more recent generations that a postmaterialist value shift has taken place with a greater emphasis on leisure time and personal well-being, with a concomitant rising prevalence of leisure-time physical activity (Lamprecht 1991). In addition, the generations are marked by differences in how they perceive the meanings and contexts of leisure-time physical activity. Alongside the traditional importance of physical activity as a competitive pursuit, physical activity today is increasingly motivated by the enjoyment derived from an active lifestyle, by the attraction of the type of physical activity involved, and by the associated effects on health, appearance, and other individual motivating factors (Salmon et al. 2003; Leslie et al. 1999; Sallis and Owen 1999).
Health is an increasingly important motivator, in particular with regard to preventing disease. Prevention has advanced in recent years to the status of a moral obligation of the individual (Bröckling 2008). Elderly people in particular tend to start exercising for health reasons (Oldridge 1982; Kolt et al. 2004). In a qualitative study by Conrad (1994), some respondents said that they did not like exercising as such but were motivated by the positive body sense they experienced after exercising.
There has been little empirical investigation to date into cohort differences in physical activity. The first indications of cohort differences are given in a recent study by Breuer (2005), but the study does not indicate which factors are responsible or how initiation and dropout rates are affected.
Methods and statistical analysis
The results presented in the following are based on the German Socio-Economic Panel (GSOEP), a survey repeated annually since 1984 among an original approximately 6,000 representative households involving more than 12,000 people from the age of 16 (Haisken-DeNew and Frick 2000). An East German sample was added to the 1984 sample in 1990, followed by a migrant sample and various additional samples. Since the question regarding lifetime changes in physical activity requires a long period of analysis, the present analysis of the GSOEP is limited to West Germany.
Since event analysis models are eminently appropriate and productive with regard to the issues involved in life stage research, and enable differentiation between age, period, and cohort effects, event analysis is the method chosen for the analyses presented here. To investigate the effect of age and other factors on rates of initiation of weekly leisure-time physical activity (or discontinuation of weekly leisure-time physical activity), subsequent analysis is based on a Gompertz modelFootnote 1 formulated as follows:
where q x is the initiation/discontinuation rate at age x. Further independent variables are given by X (cf. Beck 2009; Blossfeld and Rowher 1995; Diekmann and Mitter 1984). These include time-independent variables—specifically, gender and cohort affiliation—and time-dependent variables that change in the life course—such as health satisfaction, employment status, existence of children under 6 in the household, and life stages delimited only by age. The inclusion of specific age ranges as dummy variables also allows non-monotonic age effects to be expressed. The confounders included in the analyses are selected on the basis of theoretical considerations and past studies.
Subjects who engaged in leisure-time physical activity less than once a week in the previous wave and raised their activity to at least once per week in the following wave are termed exercise initiators. Conversely, subjects who reduce their at least once weekly exercise to less than once per week are defined as exercise discontinuers.
All analyses were performed using SAS for Windows Software Version 9.2.
Results and discussion
Physical activity in GSOEP
The GSOEP is currently the only national representative database on lifetime changes in physical activity. Nevertheless, major limitations attach to the GSOEP data in some respects. Physical activity is documented on the basis of a single question regarding frequency. The GSOEP does not investigate the duration or intensity of the respective physical activity. In addition, the frequency of physical activity is queried at irregular intervals, namely, 1986, 1988, 1990, 1992, 1994, 1995, 1996, 1997, 1998, 1999, 2001, 2003, and 2005. The limitations are compounded by another difficulty associated with the fact that the relevant question was based on different classifications. Four categories were used in most cases (every week, every month, more rarely, and never), but a fifth category (daily) was used in some years (1990, 1995, 1998, and 2003). The five-item scale unfortunately does not allow a reduction to four categories, since the classification has a huge impact on response behavior (Breuer 2005).
This can also be seen from Fig. 1. In the years where physical activity was assessed in five categories, “at least weekly” activity (i.e., the above two categories taken together) is cited much more frequently, and “never“ is cited much less frequently. A response spectrum amended upward seems to “raise” the frequency of physical activity. Hence, the question provides only a limited insight into the precise frequency of physical activity and is difficult to compare with the results of other studies—such as, for example, the German National Health Survey which uses yet another method of documenting physical activity (Mensink 1999). Interpreting with caution, it can nevertheless be assumed on the basis of Fig. 1 that—leaving aside duration and intensity—about one quarter of the above-16 population engages in physical activity every week, and about half the population never engages in physical activity. Figure 1 also shows that only a relatively small proportion of the population belongs to the fairly large category between once a month and less than once a week. This is indicative of polarization of the general population into exercisers who engage in physical activity at least once a week and non-exercisers who engage in physical activity never or almost never.

Frequency of physical activity from 1986 to 2005 (GSOEP 1986, 1988, 1990, 1992, 1994, 1995, 1996, 1997, 1998, 1999, 2001, 2003, 2005)
Although the specified answering scheme has the heaviest impact on the frequency of affirmation for both extremes, the response behavior is nevertheless at its most stable for these two frequency categories. This is shown in Table 1 which describes the incidence of no change/change to another category between two surveys. Whereas almost 70% of weekly exercisers and more than 80% of “never” exercisers are in the same category at the subsequent survey, change is much more common in the intermediate categories (see top of Table 1; a similar trend is obvious with respect to the five-step scale at the bottom). Therefore, multiple change between two surveys is least likely with respect to the extreme categories.
Because of the poor comparability of the four-point and five-point scales, the present analysis is based solely on the—more frequent—investigation of physical activity on the basis of four categories. Accordingly, the period is limited to 1986–2005. In addition, the analysis is based only on longitudinal subjects, i.e., those who consistently answered the physical activity question according to the four-point classification scheme: 3,487 subjects (West Germany), or 33%Footnote 2 of the individuals first interviewed in 1984.
Age and generational dependency of physical activity
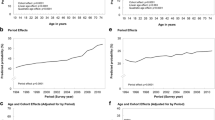
Figure 2 indicates how physical activity depends on age but also on generation and gives the proportion of weekly exercisers (i.e., individuals who engage in physical activity “every week”), differentiated by age and birth cohort. The cross-sectional curve for 2005 confirms the ubiquitous observation that exercisers engage in physical activity more rarely the older they are. The older the birth cohorts, the less exercise is taken, i.e., even when they were younger, members of older cohorts took less exercise than members of more recent cohorts. The most apparent cohort effect is between subjects socialized in wartime (> 1925, 1926–1935)Footnote 3 and afterward (1936–1945, 1946–1955, 1956–1970).Footnote 4 In contrast, period effects seem to have no major effect on the development of inactivity in the course of a lifetime.

Proportion of physically active (defined as physical exerciser at least once a week) adults by age and year of birth (GSOEP 1986, 1988, 1992, 1994, 1996, 1997, 1999, 2001, 2005)
The presented prevalence of physical activity is the result of initiation and discontinuation patterns. The following analyses investigate how age and cohort affect initiation and discontinuation rates, and which factors may be responsible for age and cohort effects. Table 2 primarily contains an analysis of age and cohort influences on initiation rates of physical activity every week, and the respective discontinuation rate. For example, the value of 0.986 (top of Table 2, column 3) indicates that the inclination to stop weekly physical activity declines 0.986-fold or by (1–0.986 =) 1.4% for every additional year of life. The initiation rate (column 1) declines at the same time but the effect is not significant. Hence, a reduction in discontinuation rate seems more likely than a reduction in the initiation rate in a lifetime.
Table 2 also considers the various assumptions with respect to non-continuous changes in physical activity. As can be seen from Table 2 (column 3), the discontinuation rate in early adulthood from age 20 to 30 is, in fact, almost 27.5% higher, while the initiation rate in this age range is not significantly lower. This observation agrees with the observation that the time budget tends to be under greater pressure in early adulthood as a result of job and family demands.
A discontinuity in age dependency is also seen for the higher age group of 60- to 66-year-olds. This only applies to discontinuation but not to initiation. In other words, there is no resumption of physical activity toward the end of working life and during the transition to retirement, i.e., when more leisure time becomes available again. One factor might be that the “fitness barrier” has grown excessively high after years and decades of inactivity. Transition to retirement only affects discontinuation behavior, in that anyone who has engaged in regular physical activity beforehand is even less likely to discontinue after reaching this age group.
Thus, it can be seen that a certain life stage dependency affects discontinuation but not initiation patterns. Nevertheless, a clustering of discontinuations in early adulthood and reduced discontinuations toward the end of workforce employment and during transition to retirement are strong arguments for the influence of lifetime stage on physical activity.
Finally, columns 1 and 3 of Table 2 give an account of cohort effects. Each subsequent year of birth cohort has an almost 2% lower discontinuation rate than the preceding birth year, while the discontinuation rate is 1.8% higher. Hence, the increased “athleticism” of subsequent generations is attributable both to an increase in initiation rates and to a decrease in discontinuation.
Effect of health and fitness
To what extent do health and fitness determine age and generational influences? Initiation and discontinuation of physical activity can be explained by health but can also be explained by—for instance—changing life circumstances. To obtain more precise information, various influencing factors are controlled for statistically in the following analysis. This means that age and cohort effects are analyzed under the (fictive) assumption that the factors in question do not differ between age groups or between generations. The extent to which the age effect disappears or is reduced can be explained by the factors in question (such as health and life circumstances).
The second and fourth columns of Table 2 also include the influence of health in the analysis for that reason. Health satisfaction in the period close to the relevant initiation or discontinuation event is taken into consideration, as is the current change in health satisfaction. For every step on the 11-point health satisfaction scale, the rate of initiation of physical activity at least once a week is 5.5% higher for non-exercisers and the discontinuation rate for exercisers is (1–0.96=) 4.0% lower (Table 2). There is also a 6.8% increase in initiation rate and a 5.5% reduction in discontinuation rate associated with a current increase in health satisfaction by one point (Table 2).
Despite the relevance of health satisfaction for the initiation and discontinuation of exercise, the effect of age on the discontinuation rate remains almost unchanged (see columns 1 and 2, and columns 3 and 4, of Table 2). Changes in cohort effects are similarly minor. Neither age nor cohort differences in physical activity can therefore be explained simply by health and fitness.
Age and generational differences in physical activity display a remarkably low correlation with health and fitness, however. Nevertheless, it would be premature to discount fitness and health as explanations for physical activity. For one, this paper confirms other studies indicating that good health promotes the initiation of a physically active lifestyle. The age dependency of initiation and discontinuation behavior in terms of starting/ending regular physical activity was not—or only marginally—attributable to the health factor. For another, the deficient power of the health factor to explain the age effect may be subject to data-related reservations and necessitates a nuanced approach.
For instance, due to a lack of precise data, the present analysis is based not on medical diagnoses of health but subjective assessment of health and satisfaction with health. Admittedly, numerous studies (Sieverding 1998) show a high correlation between objective and subjective health measurements. However, it is also well known that subjective assessment is affected by adaptation to age-matched peers. As a result, any deterioration in health accompanying advancing age is not adequately reflected in subjective evaluations of health.
Effect of life circumstances and socialization
With respect to life circumstances, the main influencing factors are time limitations and physical strain arising from work and household demands. Since job and family have different impacts on time budget and physical reserves for men and women, the following analyses look at the genders separately. Gender-specific calculations are limited, however, to analyses of discontinuation, as the previously established effects of age and lifetime stages primarily concern discontinuation.
As is obvious from Table 3, the biographical decline in discontinuation rate for women is much more marked than for men (for men, the age effect on discontinuation is below the level of statistical significance). At age 20–30, both genders experience an increase in discontinuation, which tends, in fact, to be even greater for men than for women.
In the remaining columns, workforce employment, existence of children under the age of 6, and educational attainment are controlled for in the models. Workforce employment and family are the primary determinants of time budget constraints and the extent of other physical exertion, whereas educational attainment is additionally of significance for socialization.
With respect to the restriction of time through workforce employment, Table 3 (columns 2 and 4) distinguishes between part-time and full-time employment versus non-employment. As can be seen from Table 3, neither part-time nor full-time employment or occupational status is associated with a statistically significant increase in discontinuation rate.
In terms of partnership and family situation, restrictions on time and physical strain primarily depend on whether individuals are responsible for the care of young children. The existence of children under the age of 6 indeed increases the discontinuation rate both for women and for men, but the effect is greater for women.
Taking workforce employment, job status, existence of children in the household, and educational attainment into account, the continuous age effect of reducing the discontinuation rate in successive years of life remains almost unchanged (compare columns 1 and 2 and columns 3 and 4, respectively). However, the increased discontinuation of women between ages 20 and 30 is reduced considerably, i.e., the parameters given before account for this increase primarily through the absorption of time and physical exertion by young children.
Correspondingly, the cohort effect is slightly reduced for men and for women, which can be taken as indicative of lifetime differences between the cohorts, partly due to a change in job structure (with increasingly less room for unskilled workers), to a declining birth rate, and, not least, to the expansion of education.
Surprisingly, job-related time pressures and physical exertion have less of an effect than generally supposed. These two factors can explain only a small part of the increased rate of discontinuation of physical activity among 20- to 30-year-olds, and apply to men rather than women. Among women, the existence of children contributes greatly to explaining the increased discontinuation rate between ages 20 and 30. The explanatory power of job and family might be revealed to be greater if the conclusions were not limited to once-weekly physical activity and if better data on duration and intensity of physical activity were available.
To compound matters, the database provides little information about the details of physical activity. Nothing is known, for instance, about the duration and intensity of physical activity or the type of physical activity and its requirements in terms of strength, endurance, and physical control. It needs to be taken into account that the category “every week” allows vast latitude in terms of frequency and duration of the respective physical activity, and also in terms of its intensity. Health restrictions would have to be very severe indeed to prohibit a person from engaging in physical activity of any duration or intensity at least once a week. It is therefore possible that the relevant connections exist within this wide sporting category, and that the possible explanatory power of the health factor for the age effect remains invisible only on that account.
Strengths and weakness of the study
The main strength of our study is the population-based design and the long follow-up time and the statistical methods involving time-updated variables. Little data are available that would enable analysis over such a long period. The main limitation of these data is that physical activity is documented on the basis of a single question regarding frequency. The duration or intensity of the retrospective physical activity is not investigated. Another limitation is that only 33% of the GSOEP interviews were able to be included in the analysis. This is attributable to a panel mortality issue. During panel studies, participants frequently drop out of the study population for reasons such as illness, unsustained motivation, or relocation. This can be a problem as it may lead to systematic bias if, as may be the case, the dropouts differ in various characteristics from individuals remaining in the panel. Despite these drawbacks, the advantages of panel data prevail. That is because retrospectively generated data may demonstrate significant recall bias and be less informative than panel data. One main advantage over other studies is hence the longitudinal design and the inclusion of time-dependent variables. Much of the evidence concerning exercise and age is from cross-sectional data (e.g., Boutelle et al. 2000; Lim and Taylor 2005). In many cases, previous studies have merely compared various age groups at one point in time (in a cross section). Many longitudinal studies tend to neglect cohort differences (e.g., Shaw et al. 2010). Various studies based on longitudinal data demonstrate, in contrast to our study, that the age-dependent decline in physical activity is not attributable to cohort effects (Bijnen et al. 1998; Shaw and Spokane 2008; Verbrugge et al. 1996 ). However, many of these studies include work-related physical activity (e.g., Shaw and Spokane 2008). Another advantage of our study is that it investigates actual changes (exercise initiation and discontinuation) rather than merely reporting prevalences.
Conclusions
Looking at all the results together, it is possible to conclude—at least for the over-30 age group—that the ubiquitous differences in leisure-time physical activity between age groups are almost exclusively due to cohort differences. Thus, the lower participation of older people in leisure-time physical activity has less to do with their age than the generation to which they belong. Seemingly, age differences tend to be confused with intergenerational differences.
Nonetheless, the inclination to initiate at least weekly exercise declines with increasing age. At the same time, however, exercisers are less likely to discontinue, which offsets the declining initiation rate and, on balance, results in a largely constant distribution of leisure-time physical activity in the course of a lifetime.
Rather than health and fitness, social factors are revealed to be of importance. These also result in discontinuities in terms of the relationship between age and physical activity and, in particular, are responsible for the fact that the discontinuation rate is markedly increased in young adulthood (age 20–30).
Apart from the issue analyzed here, this paper also shows that the seemingly proven elementary knowledge of the importance of fitness and health as an explanation for leisure-time physical activity may need extensive expansion in order to embrace social factors. However, national representative data in this area are seriously lacking.
The significantly lower participation of the elderly in leisure-time physical activity further indicates that leisure-time physical activity is mainly pursued by sectors of society with an already lower morbidity or lower risk of falling ill. These are the very people who are more likely to avail themselves of preventive health offerings. This phenomenon is well known from studies investigating target group uptake of health promotion measures (such as vaccination programs, nutrition counseling, back health, and weight reduction courses), where it is termed “preaching to the converted” (Oddy et al. 1995; Rost et al. 1990).
To make the health benefits of exercise accessible to all sectors of the population in spite of the above, it is crucial to avoid the systematic exclusion of specific sectors of the population from leisure-time physical activity.
More target group-specific physical activity offerings should therefore be made available to elderly people in the form of low-threshold but fitness-enhancing physical activities in low-cost, easily learned, flexible sports (Nordic walking, swimming, hill walking, cycling). According to Abele and Brehm (1990), fitness courses are the ideal initiation opportunity for people who have not engaged in sports since their school days. Doctors can also play a decisive role in encouraging older people to exercise. An explicit recommendation from the primary care physician is one of the most influential and effective factors in promoting leisure-time physical activity (e.g., Schneider and Becker 2005).
Notes
The Gompertz model’s usefulness has been established in the analysis of monotonic biomedical aging processes. The model is widely used in the analysis of increasing lifetime mortality and morbidity (Heigl 2004; Klein and Unger 2002; Richards 2008). Gompertz himself explored age-related mortality. His view was that the increase in mortality with age was a consequence of exponentially diminishing functional performance (Lampert and Kroll 2005).
Panel mortality is a well-known methodological problem in panel data analysis. Panel mortality refers to loss of participants in the course of panel studies for reasons such as illness, death, relocation, or loss of motivation. As a result, subjects who took part in all the relevant waves are not a random selection. Elderly people tend to be underrepresented in the study population because of illness or death, along with individuals living a fairly discontinuous lifestyle (e.g., long periods spent abroad). However, rigorous panel management (e.g., subjects are followed up even after moving out of the original household) is done to minimize panel mortality (Haisken-DeNew and Frick 2005).
Although individuals in these groups were born before World War II, critical socialization took place during the wartime years.
Although most people in the 1936–1945 birth cohort were born during World War II, the critical socialization period was after the war.
References
Abele A, Brehm W (1990) Wer ist der „typische“ Fitneß-Sportler? Sportwissenschaft 2:4–32
Barker DJP (1998) Mothers, babies and health in later life. Churchill Livingstone, Edinburgh
Bässler R (1990) Sportaktivität und Sportabstinenz. Spectrum Sportwiss 2:78–103
Beck N (2009) Ereignisanalyse. In: Kühl S, Strodtholz P, Taffertshofer A (eds) Handbuch Methoden der Sozialforschung. Quantitative und Qualitative Methoden. VS Verlag, Wiesbaden, pp 714–741
Becker S, Schneider S (2005) Analysen zur Sportbeteiligung auf der Basis des repräsentativen Bundes-Gesundheitssurveys 1998. Sport Ges 2:173–204
Bengtsson T, Lindstrom M (2000) Childhood misery and disease in later life: the effects on mortality in old age of hazards experienced in early life, southern Sweden, 1760–1894. Popul Stud (Camb) 54:263–277
Bijnen FC, Feskens EJF, Caspersen CJ, Mosterd WL et al (1998) Age, period, and cohort effects on physical activity among elderly men during 10 years of follow-up: the Zutphen Elderly Study. J Gerontol A Biol Sci Med Sci 53:M235–M241
Boardley D, Fahlman M, Topp R, Morgan AL et al (2007) The impact of exercise training on blood lipids in older adults. Am J Geriatr Cardiol 16:30–35
Blech J (2006) Fit wie in der Steinzeit. Der Spiegel 5/2006:134–145
Blossfeld HP, Rowher G (1995). Techniques of event history modeling. New approaches to causal analysis. Lawrence Erlbaum Associates, Mahwah
Boutelle KN, Murray DM, Jefferey RW, Hennrikus DJ, Lando HA (2000) Associations between exercise and health behaviors in a community sample of working adults. Prev Med 30:217–224
Brach JS, Simonsick EM, Kritchevsky S, Yaffe K et al (2004) The association between physical function and lifestyle activity and exercise in the health, aging and body composition study. J Am Geriatr Soc 52:502–509
Brändle M, Amann FW, Salomon F (1999) Diabetes mellitus Typ 2 und koronare Herzkrankheit. Schweiz Med Wochenschr 129:700–706
Breuer C (2005) Cohort effects in physical inactivity. A neglected category and its health economical implications. J Public Health 13:189–195
Bröckling U (2008) Vorbeugen ist besser? Zur Soziologie der Prävention. Behemoth. A Journal on Civilisation 1:38–48
Byberg L, Zethelius B, McKeigue PM, Lithell HO (2001) Changes in physical activity are associated with changes in metabolic cardiovascular risk factors. Diabetologia 44:2134–2139
Byberg L, Melhus H, Gedeborg R, Sundström J, Ahllbom A, Zethelius B, Berglund LG, Wolk A, Michaëlsson K (2009) Total mortality after changes in leisure time physical activity in 50 year old men: 35 year follow-up of population based cohort. Br J Sports Med 43:482–490
Conrad P (1994) Wellness as virtue: mortality and the pursuit of health. Cult Med Psychiatry 18:385–401
Costa DL (2000) Understanding the twentieth-century decline in chronic conditions among older men. Demography 37:53–72
Crespo CJ, Ainsworth BE, Keteyian SJ, Heath GW, Smit E (1999) Prevalence of physical inactivity and its relation to social class in U.S. adults: results from the Third National Health and Nutrition Examination Survey, 1988–1994. Med Sci Sports Exerc 31:1821–1827
Dai S, Marti B, Rickenbach M, Gutzwiller F (1990) Sport korreliert mit günstigen Lebensgewohnheiten - Ergebnisse der Bevölkerungsstudie des Schweizer MONICA-Projekts. Schweiz Z Sportmed 38:71–77
Diekmann A, Mitter P (1984) Methoden zur Analyse von Zeitverläufen. Anwendung stochastischer Prozesse bei der Analyse von Ereignisdaten. Teubner, Stuttgart
Dinkel RH (1999) Demographische Entwicklung und Gesundheitszustand. Eine empirische Kalkulation der Healthy Life Expectancy für die Bundesrepublik auf der Basis von Kohortensterbetafeln. In: Häfner H (ed) Gesundheit - unser höchstes Gut? Springer, Berlin, pp 61–84
Droomers M, Schrijvers CTM, Van De Mheen H, Mackenbach JP (1998) Educational differences in leisure-time Pphysical inactivity: a descriptive and explanatory study. Soc Sci Med 47:1665–1676
Erlinghagen M (2003) Wer treibt Sport im geteilten und vereinten Deutschland? Eine quantitative Analyse sozio-ökonomischer Determinanten des Breitensports. Graue Reihe des Instituts Arbeit und Technik. IAT, Gelsenkirchen
Gavrilova NS, Gavrilov LA, Evdokushkina GN, Semyonova VG (2003) Early-life predictors of human longevity: Aanalysis of the XIXth century birth cohorts. Ann Demogr Hist 106:177–198
Gregg EW (1996) Self-rated health and the spectrum of physical activity and physical function in older women. J Aging Phys Act 4:349–361
Haisken-DeNew JP, Frick JR (eds) (2000) DTC. Desktop Companion to the German Socio-Economic Panel Study (GSOEP), vol 3. Deutsches Institut für Wirtschaftsforschung, Berlin
Haisken-DeNew JP, Frick JR (eds) (2005) DTC. Desktop Companion to the German Socio-Economic Panel Study (GSOEP), vol 3. Deutsches Institut für Wirtschaftsforschung, Berlin
Heigl A (2004) Älter gleich kränker? BIB 111:41–49
Hirvensalo M, Lampinen P, Rantanen T (1998) Physical exercise in old age: an eight-year follow-up study on involvement, motives, and obstacles among persons age 65–84. J Aging Phys Act 6:168
Hollmann W, Hettinger T (2000) Sportmedizin: Grundlagen für Arbeit, Training und Präventivmedizin. Schattauer, Stuttgart
Hubert H, Bloch D, Oehlert J, Fries J (2002) Lifestyle habits and compression of morbidity. J Gerontol A Biol Sci Med Sci 57:M347–M351
Roberts RE, Deleger S, Strawbridge WJ, Kaplan GA (2003) Prospective association between obesity and depression: evidence from the Alameda County Study. Int J Obes Relat Metab Disord 27:514–521
Katzmarzyk PT, Janssen I, Ardern CI (2003) Physical inactivity, excess adiposity and premature mortality. Obes Rev 4:257–290
Klein T, Löwel H, Schneider S, Zimmermann M (2002) Soziale Beziehungen, Stress und Mortalität. Z Gerontol Geriatr 35(5):441–449
Klein T, Unger R (2002) Aktive Lebenserwartung in Deutschland und in den USA. Kohortenbezogene Analysen auf Basis des Sozio-ökonomischen Panel und der Panel Study of Income Dynamics. Z Gerontol Geriatr 35:528–539
Kokkinos PF, Narayan P, Papademetriou V (2001) Exercise as hypertension therapy. Cardiol Clin 19(3):507–516
Kolt GS, Driver RP, Giles LC (2004) Why older Australians participate in exercise and sport. J Aging Phys Act 12:185–198
Lampert T, Kroll LE (2005) Einfluss der Einkommensposition auf die Gesundheit und Lebenserwartung. DIW, Berlin
Lamprecht M (1991) Sport und Lebensalter. ESSM, Magglingen
Leslie E, Owen N, Salmon J, Bauman A, Sallis JF, Lo SK (1999) Insufficiently active Australian college students: perceived personal, social, and environmental influences. Prev Med 28:20–27
Lim K, Taylor L (2005) Factors associated with physical activity among older people—a population-based study. Prev Med 40:33–40
Lindström M, Hanson B, Östergren P-O (2001) Socioeconomic differences in leisure-time physical activity: the role of social participation and social capital in shaping health related behaviour. Soc Sci Med 52:441–451
Mensink GBM (1999) Körperliche Aktivität. Gesundheitswesen 61:126–131
Mensink GBM, Loose N, Oomen CM (1997) Physical activity and its association with other lifestyle factors. Eur J Epidemiol 13:771–778
Meyer K, Niemann S, Abel T (2004) Gender differences in physical activity and fitness—association with self-reported health and health-relevant attitudes in a middle-aged Swiss urban population. J Public Health 12:283–290
Oddy WH, Holman CD, Corti B, Donovan RJ (1995) Epidemiological measures of participation in community health promotion projects. Int J Epidemiol 24:1013–1021
Oldridge NB (1982) Compliance and exercise in primary and secondary prevention of coronary heart disease: a review. Prev Med 11:56–70
Panagiotakos DE, Pitsavos C, Chrysohoo C, Skoumas J et al (2003) Effect of leisure time physical activity on blood lipid levels: the ATTICA study. Coron Artery Dis 14:533–539
Patel KV, Coppin AK, Manini TM, Lauretani F et al (2006) Midlife physical activity and mobility in older age: The InCHIANTI study. Am J Prev Med 31:217–224
Pescatello DE, Franklin BA, Fagard R, Farquhar R, Farquhar WB et al (2004) American College of Sports Medicine position stand. Exercise and hypertension. Med Sci Sports Exerc 36:533–553
Pfaffenbarger RS, Hyde RT, Wing AL, Lee IM et al (1993) The associations of change in physical-activity level and other livestyle characteristics with mortality among men. N Engl J Med 328:538–545
Ransdell LB, Wells CL (1998) Physical activity in urban white, African-American, and Mexican-American women. Med Sci Sports Exerc 30:1608–1615
Richards SJ (2008) Applying survival models to pensioner mortality data. Br Actuarial J 14:257–303
Rost K, Connell C, Schlechtman K, Barzilai B et al (1990) Predictors of employee involvement in a worksite health promotion program. Health Educ Q 17:395–407
Ruchlin HS, Lachs MS (1999) Prevalence and correlates of exercise among older adults. J Appl Gerontol 18:341–357
Sallis JF, Hovell MF, Hofstetter RC, Faucher P et al (1989) A multivariate study of determinants of vigorous exercise in a community sample. Prev Med 18:20–34
Sallis JF, Owen N (1999) Physical activity & behavioral medicine. Sage, Thousand Oaks
Salmon J, Owen N, Crawford D, Bauman A, Sallis JF (2003) Physical activity and sedentary behavior: a population-based study of barriers, enjoyment, and preference. Health Psychol 22:178–188
Schneider S, Becker S (2005) Prevalence of physical activity among the working population and correlation with work-related factors: results from the first German National Health Survey. J Occup Health 47:414–423
Shaw BA, Spokane LS (2008) Examining the association between education level and physical activity changes during early old age. J Aging Health 20:767–787
Shaw BA, Liang J, Krause N, Gallant M, McGeever K (2010) Age differences and social stratification in the long-term trajectories of leisure-time physical activity. J Gerontol B Psychol Sci Soc Sci 65:756–766
Sieverding M (1998) Sind Frauen weniger gesund als Männer? Überprüfung einer verbreiteten Annahme anhand neuerer Befunde. Köln Z Soziol Sozialpsychol 50:471–489
Sternfeld B, Ainsworth BE, Quesenberry CP (1999) Physical activity patterns in a diverse population of women. Prev Med 28:313–323
Thune I, Njølstad I, Løchen M, Førde OH (1998) Physical activity improves the metabolic risk profiles in men and women. Arch Intern Med 158:1633–1640
Verbrugge LM, Gruber-Baldini AL, Fozard JL (1996) Age differences and age changes in activities: Baltimore Longitudinal Study of Aging. J Gerontol B Psychol Sci Soc Sci 51:S30–S41
Wannamethee SG, Shaper AG, Walker M (1998) Changes in physical activity, mortality, and incidence of coronary heart diseases in older men. Lancet 351(9116):1603–1608
Wannamethee SG, Shaper AG (2001) Physical activity in the prevention of cardiovascular disease: an epidemiological perspective. Sports Med 31:101–114
Whaley DE, Ebbeck V (1997) Older adults’ constraints to participation in structured exercise classes. J Aging Phys Act 5:190–212
World Health Organization (2002) Active ageing. A policy framework. World Health Organization, Geneva
World Health Organization (2003) Health and development through physical activity and sport. World Health Organization, Geneva
Yang X, Telama R, Hirvensalo M, Mattsson N, Viikari JSA, Raitakari O (2008) The longitudinal effects of physical activity history on metabolic syndrome. Med Sci Sports Exerc 40(8):1424–1431
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Klein, T., Becker, S. Age and exercise: a theoretical and empirical analysis of the effect of age and generation on physical activity. J Public Health 20, 11–21 (2012). https://doi.org/10.1007/s10389-011-0428-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-011-0428-0