
Abstract
The question as to whether fitness should be assessed in a European health monitoring system, perhaps from the early stages of life onwards, remains to be answered. We aimed to examine the associations between cardiorespiratory fitness and metabolic risk factors in children. A total of 873 healthy children from Sweden and Estonia aged 9–10 years (444 girls and 429 boys) were randomly selected. A maximal ergometer bike test was used to estimate cardiorespiratory fitness. Additional cardiovascular risk factors were assessed. Significant differences among cardiorespiratory fitness quartiles for the sum of five skinfolds, insulin resistance, triglycerides, and total cholesterol (TC) and high-density lipoprotein cholesterol (HDLc) ratio were shown in girls whereas in boys, the sum of five skinfolds and insulin resistance were significantly different. The lowest sum of five skinfolds and insulin resistance was shown in the highest cardiorespiratory fitness quartile in girls and boys, and the lowest values of triglyceride and TC/HDLc values in the highest cardiorespiratory fitness quartile was observed only in girls. Cardiorespiratory fitness was negatively associated with a clustering of metabolic risk factors in girls and boys. The results add supportive evidence to the body of knowledge suggesting that cardiorespiratory fitness in children is an important health marker and thus should be considered to be included in a pan-European health monitoring system.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low cardiorespiratory fitness seems to be an important health problem (Lee et al. 1999; Carnethon et al. 2003; Mora et al. 2003; Myers et al. 2002). It has been recently shown that low cardiorespiratory fitness is a strong and independent predictor of incident metabolic syndrome (i.e. hypertension, dyslipidemia, impaired glycemic control and obesity) in men and women (LaMonte et al. 2005), which could be one of the mechanism of overall cardiovascular disease. Moreover, cardiorespiratory fitness seems to prevent premature mortality regardless of body-weight status or the presence of metabolic syndrome in adult men (Katzmarzyk et al. 2004, 2005).
High cardiorespiratory fitness during childhood and adolescence has been associated not only with healthier cardiovascular profile during these years but also later in life (Twisk et al. 2002). However, the association between cardiorespiratory fitness and cardiovascular risk factors in children is uncertain, probably because of low research priority. Furthermore, most children are asymptomatic for cardiovascular disease. Cardiorespiratory fitness has been suggested to be included in the European Health Monitoring System for the adult population (Sjöström et al. 2005), but the question as to whether fitness should be assessed in European health monitoring systems from the early stages of life remains to be answered. Understanding the association between a low cardiorespiratory fitness and cardiovascular-disease-related outcomes in children would support the question as to whether cardiorespiratory fitness might or might not be proposed as a health marker at these ages. Therefore, the aim of the present report was to examine the associations of cardiorespiratory fitness to health-related variables in a wide cohort of children aged 9–10 years and to relate the findings with corresponding results from recent cross-sectional and prospective cohort studies.
Research design and methods
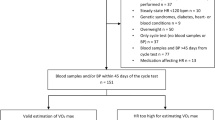
The present cross-sectional study involved 873 children aged 9–10 years (444 girls, 429 boys). The subjects comprised Estonian and Swedish children who were part of the European Youth Heart Study (EYHS) (Poortvliet et al. 2003). The pooling of data was assumed to be possible because of the use of common protocols in both countries (Poortvliet et al. 2003; Wennlof et al. 2003). Study design, selection criteria and sample calculations have been reported elsewhere (Riddoch et al. 2005).
In Estonia, the city of Tartu and its surrounding rural area was the geographical sampling area. In Sweden, seven municipalities in the Stockholm area and one in Örebro were chosen for data collection. The local ethical committees approved the study (University of Tartu no. 49/30-1997, University Hospital no. 474/98 Huddinge, and Örebro City Council no. 690/98). The study procedures were explained verbally and in written text to all parents and children. One parent or legal guardian provided written informed consent, and all children gave verbal consent.
Data collection
Physical examination
Height and weight were measured by standardized procedures. Body mass index was calculated as weight/height squared (kg/m2). Skinfold thicknesses were measured with a Harpenden caliper at the biceps, triceps, subscapular, suprailiac and triceps surae areas on the left side of the body. These measures have been shown to highly correlate with dual-energy X-ray absorptiometry-measured body fat percentage in children of similar ages (Gutin et al. 1996). All measurements were taken twice and in rotation, and the mean was calculated. If the difference between the two measurements differed by >2 mm, a third measurement was taken, and the two closest measurements were averaged. The sum of five skinfold thicknesses was used as an indicator of body fat.
Blood pressure
The systolic and diastolic blood pressures were measured with an automatic oscillometric method (Dinamap model XL Critikron, Inc., Tampa, Florida.). The equipment has been validated in children (Park and Menard 1987). An appropriate cuff size was chosen according to the manufacturer’s recommendation after checking the arm circumference. The subject was in a sitting, relaxed position, and recordings were made every second minute for 10 min with the aim of obtaining a set of systolic recordings not varying by more than 5 mmHg. The mean value of the last three recordings was used as the resting systolic and diastolic blood pressure in millimeters of mercury (mmHg).
Blood samples
With the subject in the supine position, blood samples were taken by venipuncture after an overnight fast, using vacuum tubes (Vacuette, Greiner Lab Technologies Inc). The fasting state was verbally confirmed by the subject before blood sampling. Blood was centrifuged for 10 min at 2,000 g, serum was separated within 30–60 min, and the samples were stored at −80°C. Serum concentrations of triglycerides, total cholesterol (TC), high-density lipoprotein cholesterol (HDLc), and glucose were measured on an Olympus AU600 autoanalyser (Olympus Diagnostica GmbH, Hamburg, Germany). The insulin for the Estonian subjects was analyzed with an enzyme immunoassay (DAKO Diagnostics Ltd., Ely, England). All analyses were performed at Bristol Royal Infirmary, UK, with the exception of insulin for the Swedish subjects, which was performed at Huddinge University Hospital, Sweden (Elecsys, Roche Diagnostics GmbH, Mannheim, Germany). A more detailed description of the blood analysis has been reported elsewhere (Wennlof et al. 2005). Insulin resistance was estimated from fasting glucose and insulin according to the homeostasis model assessment (HOMA) (Matthews et al. 1985), and the ratio TC/HDLc was also calculated.
Cardiorespiratory fitness test
Cardiorespiratory fitness was determined by a maximum cycle-ergometer test, as described elsewhere (Hansen et al. 1989). Briefly, the workload was preprogrammed on a computerized cycle ergometer (Monark 829E Ergomedic, Vansbro, Sweden) to increase every third minute until exhaustion. Heart rate was registered continuously by telemetry (Polar Sport Tester, Kempele, Finland). Criteria for exhaustion were a heart rate ≥185 beats per minute, failure to maintain a pedaling frequency of at least 30 revolutions per minute, and a subjective judgment by the observer that the child could no longer keep up, even after vocal encouragement. The power output was calculated as =W1+(W2 · t/180), where W1 is a work rate at fully completed stage, W2 is the work rate increment at final incomplete stage, and t is time in second at final incomplete stage. The “Hansen formula” for calculated maximum oxygen consumption (VO2max) in ml/min was = 12 x calculated power output + 5 x body weight in kg (Hansen et al. 1989). Cardiorespiratory fitness was expressed as VO2max per kilogram of body mass.
Metabolic risk score
The metabolic risk score was computed from the following six variables: insulin, glucose, HDLc, triglycerides, the sum of five skindfolds, and blood pressure (systolic and diastolic blood pressure). Each of these variables was standardized as follow: standardized value = (value − mean)/SD. The HDLc standardized value was multiplied by −1 to indicate higher cardiovascular risk with increasing value. The standardized values of systolic and diastolic blood pressure were averaged. The metabolic risk score was compiled by the sum of the six standardized scores divided by six. The resulting risk score is a continuous variable with a mean of zero by definition, with lower scores denominating a more favorable profile.
Statistical analysis
All variables were checked for normality of distribution before the analysis, and appropriate transformations were applied when necessary. Sum of five skinfolds, triglycerides, low-density lipoprotein cholesterol (LDLc), TC, and TC/HDLc were logarithmically transformed, and HOMA was transformed by taking it by the power of (1/3). Differences between metabolic syndrome individual variables and cardiorespiratory fitness quartiles, and metabolic syndrome risk score and cardiorespiratory fitness quartiles were assessed by analysis of variance (ANOVA). Differences of metabolic syndrome individual variables among cardiorespiratory fitness quartiles were assessed by Tukey’s test. All analyses were performed using the Statistical Package for Social Sciences (SPSS, version 13.0 for WINDOWS; SPSS Inc, Chicago, IL,USA), and the level of significance was set at P<0.05.
Results
The descriptive characteristics of the study sample are shown in Table 1. All subjects in this study were within the normal healthy ranges for all studied variables. The ANOVA showed significant differences among cardiorespiratory fitness quartiles for sum of five skinfolds, insulin resistance, triglycerides and TC/HDLc in girls whereas in boys, only sum of five skinfolds and insulin resistance were significantly different. Significant differences among cardiorespiratory fitness quartiles were also observed for metabolic risk score in girls and boys.
The Tukey’s test showed that the sum of five skinfolds was significantly higher in the first cardiorespiratory fitness quartile compared with the second, third and fourth cardiorespiratory fitness quartiles in girls and boys (Fig. 1). Moreover, sum of five skinfolds was significantly higher in the second cardiorespiratory fitness quartile compared with the fourth cardiorespiratory fitness quartile in girls. In boys, the sum of five skinfolds was significantly lower in the fourth cardiorespiratory fitness quartile compared with the first, second and third cardiorespiratory fitness quartiles (Fig. 1).

Associations between sum of five skinfolds and cardiorespiratory fitness quartiles in girls and boys. Data shown as mean and 95% confidence interval (CI). Girls in the first quartile (*) had a higher sum of five skinfolds than in superior quartiles (P<0.001), and girls in the second quartile (†) had a higher sum of five skinfolds than in the fourth quartile (P=0.004). Boys in the first quartile (‡) had a higher sum of five skinfolds than in superior quartiles. (P=0.007)
Insulin resistance was significantly higher in the first cardiorespiratory fitness quartile compared with the fourth cardiorespiratory fitness quartile in both girls and boys. Moreover, insulin resistance was significantly higher in the second cardiorespiratory fitness quartile compared with the fourth cardiorespiratory fitness quartile in girls (Fig. 2).

Associations between insulin resistance estimated from the homeostasis model assessment (HOMA) equation and cardiorespiratory fitness quartiles in girls and boys. Data shown as mean and 95% confidence interval (CI). Girls in the first quartile (*) had a higher HOMA than in the fourth quartile (P<0.001), and girls in the second quartile (†) had a higher sum of five skinfolds than in the fourth quartile (P<0.001). Boys in the first quartile (‡) had a higher HOMA than in the fourth quartile (P=0.007)
Triglyceride values were significantly higher in the first cardiorespiratory fitness quartile compared with the fourth cardiorespiratory fitness quartile in girls (Fig. 3). The ratio of TC/HDLc was significantly higher in the first cardiorespiratory fitness quartile compared with the second and fourth cardiorespiratory fitness quartiles in girls (Fig. 4).

Associations between triglycerides (TG) and cardiorespiratory fitness quartiles in girls and boys. Data shown as mean and 95% confidence interval (CI). Girls in the first quartile (*) had a higher TG values than in the fourth quartile (P<0.001)

Associations between total cholesterol (TC) and high-density lipoprotein cholesterol (HDLc) ratio and cardiorespiratory fitness quartiles in girls and boys. Data shown as mean and 95% confidence interval (CI). Girls in the first quartile (*) had a higher TC/HDLc ratio than in the second and fourth quartiles (P<0.001)
Metabolic risk score was significantly higher in the first cardiorespiratory fitness quartile than in the second, third and fourth cardiorespiratory fitness quartiles in girls and boys (Fig. 5). Significant differences were also found between metabolic risk score in the second and fourth cardiorespiratory fitness quartiles in girls (Fig. 5).

Associations between metabolic risk score and cardiorespiratory fitness quartiles in girls and boys. Data shown as mean and 95% confidence interval (CI). Girls in the first quartile (*) had a higher risk score than in the second, third and fourth quartiles (P<0.007), and girls in the second quartile (‡) had a higher risk score than in the fourth quartile (P<0.02). Boys in the first quartile (†) had a higher risk score than in the second, third and fourth quartiles (P=0.007)
Discussion
The association between cardiorespiratory fitness and features of metabolic syndrome was investigated in a population sample of Swedish and Estonian children aged 9–10 years. Cardiorespiratory fitness was negatively associated with a clustering of metabolic risk factors in girls and boys, and the lowest values of sum of five skinfolds, insulin resistance, triglyceride and TC/HDLc were in the highest cardiorespiratory fitness quartile.
Theses results may suggests that cardiorespiratory fitness should be proposed as a health marker in children. In fact, it is biologically plausible that a high cardiorespiratory fitness provides more health protection than low cardiorespiratory fitness, even in healthy children as well as it has been found in adults (Balady 2002; Myers et al. 2002; Carnethon et al. 2003; Gulati et al. 2003; Kurl et al. 2003; Mora et al. 2003; Church et al. 2005; Katzmarzyk et al. 2004, 2005; LaMonte el al. 2005). Risk-factor levels are lower in children than in adults, but similar patterns have been seen in children. Previous cross-sectional studies in children have shown significant associations between cardiorespiratory fitness and plasma lipids and between cardiorespiratory fitness and clustering of metabolic syndrome risk factors (Table 2). In our study, triglyceride and TC/HDLc values differed among cardiorespiratory fitness quartiles (Fig. 3). Moreover, negative associations between increased cardiorespiratory fitness and clustering of metabolic syndrome risk factors in both girls and boys have been shown here (Fig. 5). Cardiorespiratory fitness has recently been associated with arterial compliance in children aged 9–11 years, which may support the concept that fitness may exert a protective effect on the cardiovascular system (Reed et al. 2005).
Associations between cardiorespiratory fitness and cardiovascular risk factors have also been found in adolescents (Table 2). Gutin et al. (2004) found inverse associations between cardiorespiratory fitness and insulin concentrations. Furthermore, inverse associations between cardiorespiratory fitness and the likelihood of having hypertension were shown in 15- to 20-year-old subjects (Nielsen and Andersen 2003). In the present study, insulin resistance was significantly lower in the fourth cardiorespiratory fitness quartile compared with the first cardiorespiratory fitness quartile in both girls and boys (Fig. 2). However, no differences were found in systolic or diastolic blood pressure among cardiorespiratory fitness quartiles (data not shown).
A summary of recent prospective cohort studies examining the associations between cardiorespiratory fitness and health-related variables in children and adolescents is shown in Table 3. A number of longitudinal studies have suggested that a low cardiorespiratory fitness during childhood and adolescence is associated with later cardiovascular risk factors, such as hyperlipidemia, hypertension and obesity (Boreham et al. 2001, 2002; Hasselstrøm et al. 2002; Janz et al. 2002; Twisk et al. 2002; Ferreira et al. 2005). In an 8-year follow-up study, fitness during adolescence was not associated to risk factors of cardiovascular disease in adulthood, but changes in fitness from adolescence to adulthood were related to risk in adulthood. Moreover, subjects who decreased their fitness levels also changed to a worse risk factor profile (Hasselstrøm et al. 2002). Changes in cardiorespiratory fitness from adolescence to adulthood were also inversely and significantly associated with large arterial stiffness (a major risk factor for cardiovascular disease) (Ferreira et al. 2003; Boreham et al. 2004). Taken together, these results seem to support the existence of a strong association between cardiorespiratory fitness and health-related outcomes in the young population, which may suggest the importance of including cardiorespiratory fitness tests in the monitoring system.
The test used to calculate cardiorespiratory fitness in this study was objectively and accurately measured, and it has been previously validated in children of the same age (Riddoch et al. 2005). However, laboratory tests present some disadvantages, as necessity of sophisticated instruments, qualified technicians and cost and time constraints, and it may cause problems for the subjects to go to the laboratory, etc. Therefore, in some circumstances, field tests may be a better option because a large number of subjects can be tested at the same time, as the tests are simple, safe and often the only feasible methods.
The cross-sectional nature of this study limits the ability to determine any causality in the results. We also do not know if an extrapolation of the association may be made for overweight and obese children or those with subclinical manifestations of cardiovascular pathologies. Nevertheless, with regular reports of increasing childhood obesity and related disease prevalence world wide, the results of this study are noteworthy. The ideal study to answer the question as to whether high levels of cardiorespiratory fitness during childhood lower the risk of developing cardiovascular diseases later in life is a randomized controlled trial with a lifetime follow-up, in which a large number of children is assigned to either an active or a sedentary life style.
In conclusion, the present study shows negative associations between cardiorespiratory fitness and features of metabolic syndrome in children aged 9–10 years. The results suggest that cardiorespiratory fitness in children, as has been shown in adults, is potentially an important health marker and should be considered to be included in a pan-European health monitoring system.
References
Andersen LB, Hasselstrøm H, Grønfeldt V, Hansen SE, Froberg K (2004) The relationship between physical fitness and clustered risk, and tracking of clustered risk from adolescence to young adulthood: eight years follow-up in the Danish Youth and Sport Study. Int J Behav Nutr Phys Act 1:6
Balady GJ (2002) Survival of the fittest-more evidence. N Engl J Med 346:852–854
Boreham C, Twisk J, Murray L, Savage M, Strain JJ, Cran G (2001) Fitness, fatness, and coronary heart disease risk in adolescents: the Northern Ireland Young Hearts Project. Med Sci Sports Exerc 33:270–274
Boreham C, Twisk J, Neville C, Savage M, Murray L, Gallagher A (2002) Associations between physical fitness and activity patterns during adolescence and cardiovascular risk factors in young adulthood: The Northern Ireland Young Hearts Project. Int J Sports Med 23:22S–26S
Boreham CA, Ferrera I, Twisk JW Gallagher AM, Savage MJ, Murray LJ (2004) Cardiorespiratory fitness, physical activity, and arterial stiffness: The Northern Ireland Young Hearts Project. Hypertension 44:721–726
Brage S, Wedderkopp N, Ekelund U, Franks PW, Wareham NJ, Andersen LB, Froberg K (2004) European Youth Heart Study (EYHS): Features of the metabolic syndrome are associated with objectively measured physical activity and fitness in Danish children: the European Youth Heart Study (EYHS). Diabetes Care 27:2141–2148
Carnethon MR, Gidding SS, Nehgme R, Sidney S, Jacobs DR, Liu K (2003) Cardiorespiratory fitness in young adulthood and the development of cardiovascular disease risk factors. JAMA 290:3092–3100
Church TS, LaMonte MJ, Barlow CE, Blair SN (2005) Cardiorespiratory fitness and body mass index as predictors of cardiovascular disease mortality among men with diabetes. Arch Intern Med 10:2114–21220
Eisenmann JC, Katzmarzyk PT, Perusse L, Tremblay A, Despres JP, Bouchard C (2005a) Aerobic fitness, body mass index, and CVD risk factors among adolescents: the Quebec family study. Int J Obes Relat Metab Disord 29:1077–1083
Eisenmann JC, Wickel EE, Welk GJ, Blair SN (2005b) Relationship between adolescent fitness and fatness and cardiovascular disease risk factors in adulthood: the Aerobics Center Longitudinal Study (ACLS). Am Heart J 149:46–53
Ferreira I, Twisk JW, Stehouwer CD, van Mechelen W, Kemper HC. (2003) Longitudinal changes in VO2max: associations with carotid IMT and arterial stiffness. Med Sci Sports Exerc 35:1670–1678
Ferreira I, Twisk JW, Stehouver CD, van Mechelen W, Kemper HC (2005) The metabolic syndrome, cardiopulmonary fitness, and subcutaneous trunk fat as independent determinants of arterial stiffness: the Amsterdam growth and health longitudinal study. Arch Intern Med 25:875–882
Gulati M, Pandey DK, Arnsdorf MF, Lauderdale DS, Thisted RA, Wicklund RH, Al-Hani AJ, Black HR (2003) Exercise capacity and the risk of death in women: the St. James women take heart project. Circulation 108:1554–1559
Gutin B, Litaker M, Islam S, Manos T, Smith C, Treiber F (1996) Body-composition measurement in 9-11-y-old children by dual-energy X-ray absorptiometry, skinfold thickness measurements, and bioimpedance analysis. Am J Clin Nutr 63:287–292
Gutin B, Yin Z, Humphries MC, Bassali R, Le NA, Daniels S, Barbeau P (2004) Relations of fatness and fitness to fasting insulin in black and white adolescents. J Pediatr 145:737–743
Gutin B, Yin Z, Humphries MC, Bassali R, Le NA, Daniels S, Barbeau P (2005) Relations of body fatness and cardiovascular fitness to lipid profile in black and white adolescents. Pediatr Res 58:78–82
Hansen HS, Froberg K, Nielsen JR, Hyldebrandt N (1989) A new approach to assessing maximal aerobic power in children: the odense school child study. Eur J Appl Physiol Occup Physiol 58:618–624
Hasselstrøm H, Hansen SE, Froberg K, Andersen LB (2002) Physical fitness and physical activity during adolescence as predictors of cardiovascular disease risk in young adulthood. Danish youth and sports study. An eight-year follow-up study. Int J Sports Med 23:27S–31S
Janz KF, Dawson JD, Mahoney LT (2002) Increases in physical fitness during childhood improve cardiovascular health during adolescence: The muscatine study. Int J Sports Med 23:15S–21S
Katzmarzyk PT, Church TS, Blair SN (2004) Cardiorespiratory fitness attenuates the effects of the metabolic syndrome on all cause and cardiovascular disease mortality in men. Arch Intern Med 164:1092–1097
Katzmarzyk PT, Church TS, Janssen I, Ross R, Blair SN (2005) Metabolic syndrome, obesity, and mortality: impact of cardiorespiratory fitness. Diabetes Care 28:391–397
Kurl S, Laukkanen JA, Rauramaa R, Lakka TA, Sivenius J, Salonen JT (2003) Cardiorespiratory fitness and the risk for stroke in men. Arch Intern Med 163:1682–1688
LaMonte MJ, Barlow CE, Jurca R, Kampert JB, Church TS, Blair SN (2005) Cardiorespiratory fitness is inversely associated with the incidence of metabolic syndrome: a prospective study of men and women. Circulation 26:505–512
Lee CD, Blair SN, Jackson AS (1999) Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am J Clin Nutr 69:373–380
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Mora S, Redberg RF, Cui Y, Whiteman MK, Flaws JA, Sharrett AR, Blumenthal R (2003) Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women: a 20-year follow-up of the lipid research clinics prevalence study. JAMA 290:1600–1607
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE (2002) Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 346:793–801
Nielsen GA, Andersen LB (2003) The association between high blood pressure, physical fitness, and body mass index in adolescents. Prev Med 36:229–234
Park MK, Menard SM (1987) Accuracy of blood pressure measurement by the Dinamap monitor in infants and children. Pediatrics 79:907–914
Poortvliet E, Yngve A, Ekelund U, Hurtig-Wennlöf A, Nilsson A, Hagströmer M, Sjöström M (2003) The European Youth Heart Survey (EYHS). An international study that addresses the multi-dimensional issues of CVD risk factors. Forum Nutr 56:254–256
Reed KA, Warburton DE, Lewanczuk RZ, Haykowski MJ, Scott JM, Whitney CL, McGavock JM, McKay HA (2005) Arterial compliance in young children: the role of aerobic fitness. Eur J Cardiovasc Prev Rehabil 12:492–497
Riddoch C, Edwards D, Page A, Froberg K, Anderssen SA, Wedderkopp N, Brage S, Cooper AR, Sardinha LB, Harro M, Klasson-Heggebø L, van Mechelen W, Boreham C, Ekelund U, Bo Andersen L, and the European Youth Heart Study team (2005) Cardiovascular disease risk factors in children: Rationale, aims, study, design, and validation of methods. J Phys Act Health 2:115–129
Twisk JW, Kemper HC, van Mechelen W (2002) The relationship between physical fitness and physical activity during adolescence and cardiovascular disease risk factors at adult age. The Amsterdam growth and health longitudinal study. Int J Sports Med 23:S8–S14
Sjöström M, Poortvliet E, Nelson M (2005) Monitoring public health nutrition in Europe: nutritional indicators and determinants of health status. J Public Health1 3:74–83
Wennlöf AH, Yngve A, Sjöström M (2003) Sampling procedure, participation rates and representativeness in the Swedish part of the European Youth Heart Study (EYHS). Public Health Nutr 6:291–299
Wennlöf AH, Yngve A, Nilsson TK, Sjöström M (2005) Serum lipids, glucose and insulin levels in healthy schoolchildren aged 9 and 15 years from Central Sweden: reference values in relation to biological, social and lifestyle factors. Scand J Clin Lab Invest 65:65–76
Acknowledgements
The Swedish part of the study was supported by grants from the Stockholm County Council (MS), and the Estonian part was supported by a grant from the Estonian Science Foundation No. 3277 and 5209, and by Estonian Centre of Behavioural and Health Sciences. JRR and FBO were supported by a grant from Ministerio de Educación y Ciencia de España (AP2003-2128, AP2004-2745) and CSD (109/UPB31/03, 13/UPB20/04).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ruiz, J.R., Ortega, F.B., Meusel, D. et al. Cardiorespiratory fitness is associated with features of metabolic risk factors in children. Should cardiorespiratory fitness be assessed in a European health monitoring system? The European Youth Heart Study. J Public Health 14, 94–102 (2006). https://doi.org/10.1007/s10389-006-0026-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-006-0026-8