
Abstract
Purpose
The number of operations for laparoscopic antireflux surgery in Japan is much less than that in Western countries. This study’s aim was to evaluate outcome measures for redo antireflux surgery (redo-ARS) in Japanese patients.
Methods
Subjects consisted of 11 patients (2.3 %) who required redo-ARS, from an original group of 474 patients who had a primary ARS between December 1994 and January 2015. The mean age of the subjects was 57.7 years, and six of 11 patients were women (55 %). Clinical data were collected in a prospective manner, and were then reviewed retrospectively.
Results
The most common cause of failed primary ARS was dislocation of the wrap (6/11 or 54 %). Of the 11 patients, 10 (91 %) were approached laparoscopically, with one requiring conversion to open surgery. Eight (73 %) underwent redo fundoplication, and the others had hiatal hernia repair alone. Mean operation time and blood loss were 202 min and 56 mL, respectively. A perioperative gastric wall injury occurred in three patients. The postoperative course was uneventful in majority patients. Three (27 %) were required to take proton pump inhibitor (PPI), and two (18 %) had a recurrence of hiatal hernia. A postoperative questionnaire was answered by seven of 11 (63 %), and these all reported a high level of satisfaction with their surgery.
Conclusions
Redo-ARS can be performed safely under laparoscopy. There was no recurrence rate in almost 80 %, and more than 70 % of patients were withdrawn from PPI treatment postoperatively.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dallemagne et al. first reported laparoscopic antireflux surgery (LARS) in 1991 [1]. Since then, LARS has been established as a surgical treatment option for gastroesophageal reflux disease (GERD) with excellent resolution of subjective symptoms in most patients [2, 3]. In our institution, approximately 95 % of patients reported a high degree of satisfaction with the surgery on their postoperative questionnaire. On the other hand, some patients are expected to need a redo surgery, primarily for a recurrence of hiatal hernia and/or reflux esophagitis. Current literature on redo antireflux surgery (redo-ARS) has limitations due to small sample size; however, in 2015, Zhou et al. reported that out of a group of 13,050 patients who had a primary ARS, surgical reintervention was needed in 534 [4]. According to such reports, the failure rates for primary fundoplication ranged from 2 to 30 % [5–10]. Although many patients with mild recurrent symptoms can be managed nonoperatively, 3 to 6 % of primary antireflux procedures will require another surgical intervention [5, 11, 12].
A multitude of reports on redo surgeries after failed fundoplication have been submitted from Western countries. With the incidence of GERD increasing in Asia over the last 2 decades [13], the frequency with which LARS is performed in Japan has been rising as well; however, Japan’s rate of antireflux surgery is still much lower than that of Western countries. This study was performed to evaluate the outcome of redo surgery for failed LARS in Japanese patients.
Materials and methods
Information of all patients undergoing ARS at Jikei University School of Medicine (JUSM) was entered in a prospectively maintained database. After Institutional Review Board approval, the database was accessed to identify the patients. Additional informed consent was obtained from the patients whose identifying information is included in this article.
Between December 1994 and January 2015, a total of 474 patients underwent LARS at JUSM and 12 % (56/474) had recurrence of hiatal hernia, erosive reflux esophagitis, and dislocation of the wrap. Among them, 11 patients (20 %) who underwent reoperative intervention after one or more nonsurgical antireflux interventions were studied. Their clinical data were collected in a prospective manner and then reviewed retrospectively for this investigation.
Preoperative workup
The following information was extracted into a Microsoft Excel database: patient demographics, previous operative history, preoperative symptoms and evaluations, redo-ARS indication, time interval between first and second (or second and third) surgeries, operative course, perioperative outcomes, and subsequent follow-up data. Preoperative workup included barium esophagogram and esophagogastroduodenoscopy. Twenty-four-hour pH monitoring and esophageal manometry were done as indicated. Efforts were made to obtain previous operative reports.
Surgical technique
The choice of procedure was individualized based on preoperative assessments and intraoperative findings. Previous laparotomy was not considered a contraindication for laparoscopic reintervention. Regardless of the approach, laparoscopic or open, the basic steps of reoperative intervention were as follows: (1) mobilization of the fundic wrap from the hiatus and mediastinal space, (2) take down of the previous fundoplication if needed, (3) crural repair of the hiatus with or without mesh reinforcement, (4) redo fundoplication for those taken down, and (5) secure fixation using shoulder and anchor stitches to prevent recurrence of the hiatal hernia.
Follow-up
A postoperative questionnaire (excellent: 5 points, good: 4 points, satisfactory: 3 points, poor: 2 points, bad: 1 point) was prepared to evaluate patient satisfaction with their treatment, including surgery and other treatment (medications such as acid suppression drugs).
Results
The mean age of the patients was 57.7 ± 15.1 (range 29–78) years, and six of them were women (55 %). Ten of the 11 patients had one prior antireflux surgery, and one patient (9 %) had two surgeries—endoscopic gastroplication followed by laparoscopic Toupet fundoplication. Overall, Toupet fundoplication was the most common primary procedure for patients, and Nissen fundoplication was the second. One patient who had reflux esophagitis and duodenal ulcer had selective proximal vagotomy along with Toupet fundoplication. The patients’ characteristics are summarized in Table 1.
The most common presenting symptom was dysphagia in 55 % (6/11). Other symptoms were heartburn in 18 % (2/11, one was severe); as well as chest pain, back pain, vomiting, regurgitation, and belching each at a rate of 9 % (1/11). Some patients had more than one symptom.
Ten (91 %) and eight patients (73 %) underwent preoperative barium swallow and esophagogastroduodenoscopy, respectively. Dislocation of the wrap, found in six patients (54 %), was the most common cause of failed ARS. Other findings included recurrent hiatal hernia and erosive reflux esophagitis in three (27 %) patients each; and tight Nissen, esophageal motility disorder, and chronic idiopathic intestinal pseudo-obstruction (CIIP) in one (9 %) patient each (Table 2). In the patient with CIIP, increased abdominal pressures caused wrap dislocation and reflux esophagitis due to delay in gastric emptying. This patient underwent open sigmoidectomy for CIIP, and then experienced the sudden onset of CIIP 2 years after the prior surgery. Indications for redo-ARS were far from straightforward. Obstruction to the passage of food was found in six patients (55 %); discomfort of the chest or back from abnormal anatomy, and persistent vomiting and regurgitation in two (18 %); and proton pump inhibitor-resistant severe heartburn in one (9 %) (Table 3).
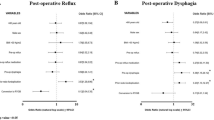
Table 4 provides findings for different variables (type of hiatal herniation, grade of erosive reflux esophagitis, and wrap status—intact or dislocated) used for the comparison of the patients who needed redo-ARS with those who did not.
Only two patients (18 %) underwent both 24-h pH monitoring and esophageal manometry and the other nine (82 %) had neither of these. Of the two patients who were evaluated, weak peristalsis was seen in one, but no evidence of abnormal gastroesophageal reflux was observed in either. The mean time interval between first and second (or third) surgery was 46 ± 43 months (0–126). No operative mortality occurred. Ten (91 %) were approached laparoscopically, and one of them (9 %) required conversion to open surgery due to extensive adhesions. Eight (73 %) underwent redo fundoplication, and the other three had hiatal hernia repair alone. The most common antireflux procedure was Toupet fundoplication (6/11, 55 %). One patient who underwent a Nissen procedure had redo surgery during the same hospitalization period. This patient was unable to eat due to esophageal dysmotility, and an open Dor fundoplication was performed. Another patient who had a shortened esophagus required a switch of fundoplication procedures from Toupet to Collis gastroplasty and Nissen. Mesh was utilized in two patients (18 %) as a component of the repair (Table 5). The mean operation time was 202 ± 46 min (125–256) and the mean blood loss was 56 ± 100 mL (0–292). No patient required a blood transfusion. A perioperative gastric wall injury was observed in three patients (27 %). Almost all postoperative courses were uneventful, with the median time to start postoperative oral intake and median postoperative hospital stay of 1 and 8 days, respectively.
The mean follow-up period after redo-ARS was 43.1 ± 46.6 months (1–130). Three patients (27 %) continued to take proton pump inhibitors despite redo surgery, and two (18 %) had a recurrence of hiatal hernia. Postoperative questionnaire answered by seven of 11 patients (63 %), and all seven reported an excellent level of satisfaction (scoring it as 5/5) with their surgery and overall treatment.
Discussion
In Japan, the number of patients undergoing surgery for GERD is much lesser than that in Western countries, and the number of reports on the results of ARS of all types is significantly less [14]. Omura et al. reported that recurrence after laparoscopic fundoplication for erosive reflux esophagitis could be predicted by anatomy–function–pathology classification, but they did not address redo operations [15]. To our knowledge, we are the first to report on outcomes of redo surgery for failed laparoscopic fundoplication in Japanese patients. We have performed LARS on 474 patients, so far, and the cumulative reoperation rate in our institution was 2.3 % (11/474). According to data from Western countries, reoperation rates were 3–6 % slightly higher than ours [16–19]; however, one report stated that 30 % of reoperations had been performed at a different hospital from that of the initial fundoplication. The authors concluded that existing literature does not reflect the true operation rate [4]. Indeed, in this study, there were two patients (18 %) who had their initial surgery in other hospitals.
Zhou et al. reported that the reoperation rate was highest at 1 year, and then steadily declined until 4 years after surgery [4]. In our study, the mean time interval between the first and second (or third, in one case) surgery was 46 ± 43 months (range 0–126). Eight of our patients (73 %) underwent redo-ARS within 3 years of their primary surgery, and two of those (18 %) were within 1 year. One to two years after surgery was the most common period for redo-ARS to be performed in this study.
Many articles comparing the outcomes of laparoscopic Nissen and Toupet fundoplication have been published [20–24]. In the current study, in terms of indications for redo-ARS, the most common cause of failure of the prior ARS was dislocation of the wrap and recurrence of the hiatal hernia. This does not suggest that the type of fundoplication procedure used is a risk factor for redo-ARS. According to our data, the most significant factors in preventing reoperations include complete crural repair, with or without mesh reinforcement, and fundic wrap fixation. Furthermore, these surgeries should be performed in centers with dedicated foregut surgeons.
During a median follow-up of 43.1 months, 18 % of the patients in this study had failure of the redo procedure. These patients did not receive reinforcement of the hiatus using a mesh and hiatal hernia recurred. This finding is similar to that of other studies. Awais et al. reported that 11 % of their patients had failure of the redo procedure requiring reoperation at a median follow-up of 39.6 months [5]. Similarly, Deschamps et al. reported that 10.8 % of their patients required reoperation at a median follow-up of 31 months [25]. In the current study, however, none of the patients have required reoperation to date.
Simorov et al. reported data showing many patients remain on PPI after ARS despite being symptom free, and the proportion taking medications increases with time [26]. In our study, while the seven patients (63 %) who answered the postoperative questionnaire all reported excellent satisfaction with surgery, two of these seven (29 %) remained on PPI therapy. This may suggest that the use of PPI in patients following redo-ARS is associated with a tendency to take PPI for psychosomatic symptoms.
Conclusions
Compared to Western countries, the number of patients undergoing reoperation for GERD in Japan is far less, and the cumulative reoperation rate appears to be slightly lower than that in Western countries. Otherwise, our study shows that patient outcomes for redo-ARS are similar in Japan to those in Western countries.
References
Dallemagne B, Weerts JM, Jehaes C, et al. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc. 1991;1:138–43.
Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA. 1995;273:59–65.
Yano F, Sherif AE, Turaga K, et al. Gastrointestinal quality of life in patients after anti reflux surgery. Dis Esophagus. 2009;22:177–84.
Zhou T, Harnsberger C, Broderick R, et al. Reoperation rates after laparoscopic fundoplication. Surg Endosc. 2015;29:510–4.
Awais O, Luketich JD, Schuchert MJ, et al. Reoperative antireflux surgery for failed fundoplication: an analysis of outcomes in 275 patients. Ann Thorac Surg. 2011;92:1083–9 (discussion 1089–90).
Little AG, Ferguson MK, Skinner DB. Reoperation for failed antireflux operations. J Thorac Cardiovasc Surg. 1986;91:511–7.
DeMeester TR, Bonavina L, Albertucci M. Nissen fundoplication for gastroesophageal reflux disease. Evaluation of primary repair in 100 consecutive patients. Ann Surg. 1986;204:9–20.
Peters JH, DeMeester TR. Indications, benefits and outcome of laparoscopic Nissen fundoplication. Dig Dis. 1996;14:169–79.
Hunter JG, Trus TL, Branum GD, et al. A physiologic approach to laparoscopic fundoplication for gastroesophageal reflux disease. Ann Surg. 1996;223:673–85 (discussion 685–7).
Smith CD, McClusky DA, Rajad MA, et al. When fundoplication fails: redo? Ann Surg. 2005;241:861–9 (discussion 869–71).
Anvari M, Allen C. Five-year comprehensive outcomes evaluation in 181 patients after laparoscopic Nissen fundoplication. J Am Coll Surg. 2003;196:51–7 (discussion 57–8; author reply 58–9).
Byrne JP, Smithers BM, Nathanson LK, et al. Symptomatic and functional outcome after laparoscopic reoperation for failed antireflux surgery. Br J Surg. 2005;92:996–1001.
Fock KM, Talley NJ, Fass R, et al. Asia-Pacific consensus on the management of gastroesophageal reflux disease: update. J Gastroenterol Hepatol. 2008;23:8–22.
Tsuboi K, Omura N, Kashiwagi H, et al. Laparoscopic Collis gastroplasty and Nissen fundoplication for reflux esophagitis with shortened esophagus in Japanese patients. Surg Laparosc Endosc Percutan Tech. 2006;16:401–5.
Omura N, Kashiwagi H, Yano F, et al. Prediction of recurrence after laparoscopic fundoplication for erosive reflux esophagitis based on anatomy-function-pathology (AFP) classification. Surg Endosc. 2007;21:427–30.
Yamamoto SR, Hoshino M, Nandipati KC, et al. Long-term outcomes of reintervention for failed fundoplication: redo fundoplication versus Roux-en-Y reconstruction. Surg Endosc. 2014;28:42–8.
Booth MI, Jones L, Stratford J, et al. Results of laparoscopic Nissen fundoplication at 2–8 years after surgery. Br J Surg. 2001;89:476–81.
Carlson MA, Frantzides CT. Complications and results of primary minimally invasive antireflux procedures: a review of 10,735 reported cases. J Am Coll Surg. 2001;193:428–39.
Catarci M, Gentileschi P, Papi C, et al. Evidence-based appraisal of antireflux fundoplication. Ann Surg. 2004;239:325–37.
Gad El-Hak N, Mostafa M, Hamdy E, et al. Short and long-term results of laparoscopic total fundic wrap (Nissen) or semifundoplication (Toupet) for gastroesophageal reflux disease. Hepatogastroenterology. 2014;61:1961–70.
Memon MA, Subramanya MS, Hossain MB, et al. Laparoscopic anterior versus posterior fundoplication for gastro-esophageal reflux disease: a meta-analysis and systematic review. World J Surg. 2015;39:981–96.
Qin M, Ding G, Yang H. A clinical comparison of laparoscopic Nissen and Toupet fundoplication for gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2013;23:601–4.
Tsuboi K, Omura N, Yano F, et al. Body mass index has no effect on the results of laparoscopic fundoplication in Japanese patients with reflux esophagitis. Esophagus. 2009;6:237–41.
Omura N, Kashiwagi H, Yano F, et al. Postoperative recurrence factors of GERD in the elderly after laparoscopic fundoplication. Esophagus. 2010;7:31–5.
Deschamps C, Trastek VF, Allen MS, et al. Long-term results after reoperation for failed antireflux procedures. J Thorac Cardiovasc Surg. 1997;113:545–50 (discussion 550–1).
Simorov A, Ranade A, Jones R, et al. Long-term patient outcomes after laparoscopic anti-reflux procedures. J Gastrointest Surg. 2014;18:157–62 (discussion 162–3).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Statement
Our work conforms to the guidelines set forth in the Helsinki Declaration of 1975, as revised in 2000 (5), concerning Human and Animal Rights, and that we followed the policy concerning Informed Consent.
Conflict of interest
Drs. Fumiaki Yano, Nobuo Omura, Kazuto Tsuboi, Masato Hoshino, Se Ryung Yamamoto, Shunsuke Akimoto, Takahiro Masuda, Norio Mitsumori, Hideyuki Kashiwagi, and Katsuhio Yanaga have no conflict of interest or financial ties to disclose in association with this study.
Rights and permissions
About this article

Cite this article
Yano, F., Omura, N., Tsuboi, K. et al. Outcomes of redo surgery for failed laparoscopic fundoplication. Esophagus 13, 290–294 (2016). https://doi.org/10.1007/s10388-016-0532-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-016-0532-x