
Abstract
Purpose
To investigate the frequency of infraorbital nerve enlargement (IONE) in orbital lymphoproliferative disorders, and to show that IONE can contribute to the clinical diagnosis of IgG4-related orbital diseases (IgG4-ROD).
Subjects and methods
71 cases in which orbital lymphoproliferative disorders were diagnosed at Okayama Medical Center and Mitoyo General Hospital from April, 2004 to March, 2011 were investigated. The male-to-female ratio was 39:32, and the age range 27–87 years old (average age 64.1 years). Whenever the coronal section of the infraorbital nerve was larger than that of the optic nerve on MRI, it was defined as IONE.
Results
The breakdown of the 71 cases was: 45 cases of non-Hodgkin lymphoma, 16 cases of IgG4-ROD, 5 cases of reactive lymphoid hyperplasia, and 5 cases of idiopathic orbital inflammation. Of these, a total of 9 cases had IONE. The incidence of IONE was compared between the IgG4-ROD patient group and the non-IgG4-ROD patient group and was significantly higher in the IgG4-ROD patient group (p < 0.0001).
Conclusion
If IONE is observed in a case of orbital lymphoproliferative disorders on MRI, then it is highly possible that such a case is IgG4-ROD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Imaging by CT and/or MRI is necessary for accurately diagnosing orbital lymphoproliferative disorders. However, on the basis of diagnostic imaging findings alone, orbital lymphoproliferative disorders cannot be further differentiated into lymphoma, IgG4-related orbital diseases [1–3], reactive lymphoid hyperplasia (RLH), idiopathic orbital inflammation, or other orbital inflammation [4]. A pathological diagnosis is essential in order to differentiate these conditions. We investigated the frequency of infraorbital nerve enlargement (IONE) in orbital lymphoproliferative disorders and found that IONE is helpful in the clinical diagnosis of IgG4-related orbital diseases.
Subjects and methods
The subjects consisted of 71 cases in which orbital lymphoproliferative disorders were diagnosed during the 7-year period from April 2004 to March 2011 at the Section of Ophthalmology, Okayama Medical Center and the Section of Ophthalmology, Mitoyo General Hospital.
The diagnostic method used to determine orbital lymphoproliferative disorders was as follows: we made a clinical diagnosis based on the MRI findings, and a definitive diagnosis based on the pathological findings. MRI was performed using the Achieva 1.5T (Philips Healthcare, Best, The Netherlands) in Okayama Medical Center and Intera 1.5T Pulsar (Philips Healthcare) and/or Signa TwinSpeed 1.5T (General Electrics Waukesha, WI, USA) in Mitoyo General Hospital. The entire orbit was scanned with a 3 mm slice thickness. T1-weighted and T2-weighted images were obtained in a coronal and axial direction, respectively.
In cases where the MRI coronal section of the infraorbital nerve was larger than that of the optic nerve, it was determined to be IONE. Cases meeting the histo-pathological criteria for IgG4-related diseases were diagnosed as being IgG4-related orbital diseases. An absolute IgG4+ cell count of more than 50 cells per high-power field, together with a ratio of IgG4+/IgG+ plasma cells >40 %, was considered immunophenotypic compatibility with IgG4-related disease. The diagnostic criteria were suggested by previous reports [5, 6]. The incidence of IONE was determined in both the IgG4-related orbital diseases patient group and the non-IgG4-related orbital diseases patient group, and the findings were statistically analyzed by Fisher’s exact test.
This study was carried out with the approval of the institutional review boards of Okayama Medical Center and Mitoyo General Hospital.
Results
The breakdown of the 71 cases of orbital lymphoproliferative disorders according to pathological diagnosis was: 45 cases of non-Hodgkin lymphoma, 16 cases of IgG4-related orbital diseases, and 5 cases of RLH, 5 cases of idiopathic orbital inflammation. The male to female ratio was 39:32, almost equal, and the age range was 27–87 years, (average age 64.1 years). There was an increase in the number of cases with age (Fig. 1).

Age distribution of the cases of orbital lymphoproliferative disorders (n = 71)
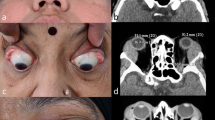
A chart classifying orbital lymphoproliferative disorders according to pathological diagnosis is shown (Table 1). The breakdown of non-Hodgkin lymphoma was: 32 cases of mucosa-associated lymphoid tissue lymphoma (MALT), 6 cases of MALT associated with IgG4-related orbital diseases (MALT + IgG4), 5 cases of diffuse large B cell lymphoma, and 2 cases of others. Therefore, there were 22 patients with IgG4-related diseases, including six patients with MALT + IgG4. Of these, a total of 9 cases were observed to have IONE, including 8 cases in IgG4-related orbital diseases and 1 case in MALT + IgG4. Hence, all cases observed to have IONE belonged to the IgG4-related orbital disease patient group (IgG4-related orbital diseases and MALT + IgG4) (Table 2). A typical case of IONE is shown in Fig. 2.

T2-weighted coronal MRI of a patient with infraorbital nerve enlargement. This patient was suffering from bilateral major lacrimal gland lesions (shaded triangles) and bilateral infraorbital nerve enlargement (shaded circles)
The incidence of IONE in the IgG4-related orbital disease patient group was 40.9 % and in the non-IgG4-related orbital disease patient group 0 %. The frequency of IONE was significantly higher in the IgG4-related orbital diseases patient group (p < 0.0001, Fisher’s exact test).
Discussion
Based on the diagnostic imaging findings alone, orbital lymphoproliferative disorders cannot be further differentiated into lymphoma, IgG4-related orbital diseases [1–3], reactive lymphoid hyperplasia (RLH), idiopathic orbital inflammation, or other orbital inflammations [4]. In IgG4-related orbital diseases, it is known that the major lacrimal gland and other soft tissues of the orbit may be involved. Moreover, it is reported that lesions can involve the orbital nerve [7, 8]. Until now, little attention has been paid to the abnormalities of the infraorbital nerve. When the infraorbital nerve is in a normal state, it is difficult to trace its route on MRI. To date, there are no authorized diagnostic criteria for diagnosing IONE on MRI. We provisionally established the diagnosis of IONE when a coronal section on MRI showed an infraorbital nerve that was larger than the optic nerve.
In this study, IONE was only observed in IgG4-related orbital diseases and MALT associated with IgG4-related orbital diseases, whereas it was not observed in MALT which does not associate with IgG4-related orbital diseases, RLH, or idiopathic orbital inflammation, which are not related to IgG4. It is, therefore, assumed that if IONE was observed in a case of orbital lymphoproliferative disorders on MRI, it is highly possible that such a case is an IgG4-related orbital disease.
Conclusion
If IONE is observed in a case of orbital lymphoproliferative disorders on MRI, then it is highly possible that it is an IgG4-related orbital disease.
References
Sato Y, Ohshima K, Ichimura K, Sato M, Yamadori I, Tanaka T, et al. Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathol Int. 2008;58:465–70.
Sato Y, Notohara K, Kojima M, Takata K, Masaki Y, Yoshino T, et al. IgG4-related disease: historical overview and pathology of hematological disorders. Pathol Int. 2010;60:247–58.
Oyama T, Takizawa J, Nakamura N, Aoki S, Aizawa Y. Abe H Multifocal mucosa-associated lymphoid tissue lymphoma associated with IgG4-related disease: a case report. Jpn J Ophthalmol. 2011;55:304–6.
De Potter P, Dolinskas C, Shields CL, Shields JA. Lymphoproliferative and histiocytic disorders. In: De Potter P, Shields CL, Shields JA, editors. MRI of the eye and orbit. Philadelphia: J. B. Lippincott Company; 1995. p. 245–53.
Sato Y, Kojima M, Takata K, Morito T, Asaoku H, Takeuchi T, et al. Systemic IgG4-related lymphadenopathy: a clinical and pathologic comparison to multicentric Castleman’s disease. Mod Pathol. 2009;22:589–99.
Cheuk W. IgG4-related sclerosing disease. A critical appraisal of an evolving clinicopathologic entity. Adv Anat Pathol. 2010;17:303–32.
Watanabe T, Fujinaga Y, Kawakami S, Hatta T, Hamano H, Kawa S, et al. Infraorbital nerve swelling associated with autoimmune pancreatitis. Jpn J Radiol. 2011;29:194–201.
Katsura M, Morita A, Horiuchi H, Ohtomo K, Machida T. IgG4-related inflammatory pseudotumor of the trigeminal nerve: another component of IgG4-related sclerosing disease? AJNR Am J Neuroradiol. 2011. doi:10.3174/ajnr.A2256.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Ohshima, Ki., Sogabe, Y. & Sato, Y. The usefulness of infraorbital nerve enlargement on MRI imaging in clinical diagnosis of IgG4-related orbital disease. Jpn J Ophthalmol 56, 380–382 (2012). https://doi.org/10.1007/s10384-012-0151-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-012-0151-6