
Abstract
Force control on the basis of prediction avoids time delays from sensory feedback during motor performance. Thus, self-produced loads arising from gravitational and inertial forces during object manipulation can be compensated for by simultaneous anticipatory changes in grip force. It has been suggested that internal forward models predict the consequences of our movements, so that grip force can be programmed in anticipation of movement-induced loads. The cerebellum has been proposed as the anatomical correlate of such internal models. Here, we present behavioural data from patients with cerebellar damage and data from brain imaging in healthy subjects further elucidating the role of the cerebellum in predictive force control. Patients with cerebellar damage exhibited clear deficits in the coupling between grip force and load. A positron-emission-tomography (PET) paradigm that separated the process of the grip force/load coupling from the isolated production of similar grip forces and loads was developed. Interaction and conjunction analyses revealed a strong activation peak in the ipsilateral posterior cerebellum particularly devoted to the predictive coupling between grip force and load. Both approaches clearly demonstrate that the cerebellum plays a major role in force prediction that cannot be compensated for by other sensorimotor structures in case of cerebellar disease. However, evidence suggests that also extra-cerebellar structures may significantly contribute to predictive force control: (1) grip force/load coupling may also be impaired after cerebral and peripheral sensorimotor lesions, (2) a coupling-related activation outside the cerebellum was observed in our PET study, and (3) the scaling of the grip force level and the dynamic grip force coupling are dissociable aspects of grip force control.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
When we manipulate objects, the grip force exerted against the object’s surface has to secure the object against slipping. On the other hand, excessive grip force has to be avoided, otherwise the object may be damaged and fatigue may occur. It has been shown that grip force normally meets both demands: grip force is only a small amount higher than the minimum force necessary to prevent object slip and is precisely scaled according to the physical object properties, such as weight, surface friction, and shape (Flanagan and Johansson 2002; Johansson 1998; Jenmalm and Johansson 1997; Johansson and Westling 1984, 1988). In addition to weight-dependent gravitational loads, acceleration-dependent inertial loads arise if the object is moved in space. Such time-varying loads impose particular demands on economical grip force control. Several studies have shown that grip force fluctuates in parallel with changes in load (Flanagan and Johansson 2002; Wing 1996; Flanagan and Wing 1993, 1995; Johansson and Cole 1992; Johansson and Westling 1984). This modulation is precisely synchronized; for example, a peak in grip force occurs at the same moment the inertial load peaks due to maximum acceleration or deceleration. During movements of a hand-held object, the muscles responsible for object transport are generally located more proximally than the muscles generating the grip. Consequently, load and grip forces are produced by mechanically largely independent muscle synergies. Synchronous modulation of grip and load forces suggests that these muscle synergies are activated simultaneously. Thus, the grip force controller does not await sensory feedback information about a change in load, since this information would be delayed by some 100 ms. Although feedback control is essential when interacting with the environment and for motor learning, complete reliance on such a mode of control would indeed result in an essential slowing of many manual activities of daily living (Witney et al. 2004; Flanagan and Johansson 2002; Wolpert and Flanagan 2001; Johansson 1998; Johansson et al. 1992).
One way to account for the simultaneity of grip and load force is to assume simultaneous planning of both forces, resulting in either one motor program for the generation of both forces or two independent motor programs, one for the arm movement and one for the grip force (Kawato et al. 2003). On the other hand, a computationally more efficient approach suggests that the grip force is predicted from the motor command for the arm movement. In this approach, only a motor plan for the arm movement is established and a copy of this motor command (efference copy) is used to plan grip force. Thus, the copy of the arm movement is processed by an internal representation of both the dynamic properties of the arm and environment to estimate the trajectory and acceleration of the arm and object. Knowledge of the physical properties of the object results in an estimate of the effective load and the grip force necessary for its manipulation (Kawato et al. 2003; Kawato 1999; Flanagan and Wing 1997; Flanagan and Tresilian 1994). Thus, the motor command for the grip force can be calculated and the grip synergy is activated synchronously or even in advance of the arm muscles causing the fluctuations in load.
The concept of internal forward models seems particularly well suited to explain the simultaneous modulation of grip force with movement-induced loads. However, grip force prediction is only one specific application of the concept. More generally, grip force prediction may be regarded a particular type of anticipatory postural adjustments. Such adjustments can be observed simultaneously with or prior to movements of the extremities which may displace the centre of gravity of the body and are processed in order to preserve postural stability (Massion 1992; Wing 1996; Forssberg et al. 1999). Internal forward models may also serve to predict the sensory outcome of movements to either enable faster and more precise programming of motor output or to cancel unwanted sensory effects of movements (re-afferent signals) (Blakemore et al. 1999; Wolpert 1997; Miall and Wolpert 1996; Wolpert et al. 1995). In a general computational framework, internal models were defined as representations of the motor system which use the current state of the motor system and motor command to predict the next state (Miall and Wolpert 1996). Forward models differ from inverse models as the latter use the desired trajectory of the arm as input to program joint movements and torques (inverse kinematics or inverse dynamics) (Kawato 1999; Wolpert 1997). It has been suggested that forward and inverse models may be combined in a pair-wise fashion in multiple modules, according to the demands of the motor task (Kawato 1999; Wolpert and Kawato 1998). Such modules are well suited to explain learning and adaptation in many varieties of motor tasks.
The idea that the trajectory of a transport movement may be planned by a different mechanism (inverse model) than the grip force applied against the transported object (forward model) has been supported by a recent study (Flanagan et al. 2003). In the experiment, the arm trajectory was perturbed by an external load. During repeated movements, the trajectory of the arm adapted much slower to the load perturbation than grip force. In addition, arm activity may induce an aberrant grip force response even in situations where the arm and grip synergies are mechanically decoupled, while, on the other hand, grip force activity does not necessarily elicit a response in arm muscles (Danion 2004). It has been pointed out, however, that alternative computational models exist that do not rely on movement prediction and simulation as distinct processes of motor control (Ostry and Feldman 2003; Todorov and Jordan 2002).
The idea that grip force is generated in a feedforward manner was encouraged by anaesthesia studies. Synchronous modulation of grip force with movement-induced loads was preserved in healthy subject moving a hand-held object after digital anaesthesia or cooling had been applied, blocking all cutaneous sensory feedback from the grasping fingers (Augurelle et al. 2003; Nowak and Hermsdörfer 2003; Nowak et al. 2001a, 2002a).However, subjects grasped the object more forcefully, suggesting that the efficiency of grip force control is impaired when the cutaneous sensibility of the grasping fingers is reduced. Grip force/load coupling is a very common strategy when manipulating objects and is observed for various types of grips and various modes of load production (Flanagan and Tresilian 1994). Even in situations where the environmental conditions change dramatically, such as a change in gravity during parabolic flight, a predictive mode of grip force control is rapidly established (Nowak et al. 2001b; Hermsdörfer et al. 2000). When we move a hand-held object that imposes artificial non-inertial loads on the grip, the novel load characteristics are incorporated into the forward controller within a few trials (Flanagan and Wing 1997). These findings suggest that internal forward models can be updated rapidly according to the demands of task and environment. It also appears as if the temporal regulation and the scaling of grip force are independently controlled (Nowak and Hermsdörfer 2003; Nowak et al. 2001a). While the synchronous modulation of grip force with the load is highly automatized and robust, grip force magnitude is more flexible, reflecting differences in task conditions.
The anatomical correlate of predictive grip forces prediction within the central nervous system is not completely understood. One structure which has been related to the neural representation of internal models is the cerebellum. Given its stereotyped cytoarchitecture, the widespread connections with spinal, cortical, and subcortical sensorimotor structures, and the neural activity of cerebellar Purkinje and nuclear cells during sensorimotor tasks, the cerebellum has long been considered to play a major role in the establishment and maintenance of sensorimotor representations related to voluntary movement. Such representations are necessary to predict the consequences of our movements. According to these theoretical concepts and both behavioural and imaging data, the cerebellum appears to be anatomically and functionally best suited to incorporate internal models (Blakemore et al. 2001; Kawato et al. 2003; Imamizu et al. 2000; Kawato 1999; Wolpert et al. 1998; Miall et al. 1993). Clinical studies in patients with cerebellar lesions clearly support this view, yielding deficits of predictive grip force coupling with self-generated loads in a variety of motor tasks (Nowak et al. 2002b; Babin-Ratté et al. 1999; Müller and Dichgans 1994; Fellows et al. 2001; Serrien and Wiesendanger 1999).
We further investigated the role of the cerebellum in grip force prediction. Here, we compare the findings of behavioural studies in patients with cerebellar lesions and cerebellar activation in healthy subjects as revealed by a brain imaging study. We investigated patients with cerebellar damage due to different aetiologies, illustrating impairments of grip force control during discrete arm movements with a hand-held load. In general, studies in cerebellar patients may be influenced by primary motor dysfunctions, such as tremor or ataxia. A functional imaging study was designed to investigate the structures involved in grip force prediction in healthy subjects. We developed an experimental paradigm which allowed us to localize brain activity especially related to grip force/load coupling by positron-emission tomography (PET) while controlling for the motor activity related to the load production and to the grip force changes.
Predictive grip force control in cerebellar patients
Methods
Predictive grip force control was analysed during movement-induced loading. Subjects were sitting in an upright position and moved a grasped object vertically in front of the trunk. The object had the form of a disc with a diameter of 9 cm, a width of 4 cm, and a mass of 372 g (Fig. 1). It was grasped with the thumb and the four fingers in opposition at the circular grip surfaces, which were covered with medium grain sandpaper (No. 240). The grip assured that loads from rotational torques were negligible. Subjects were requested to move the object up and down along a vertical line in front of the sternum while keeping the grip surfaces of the object in a frontal plane and avoiding object tilt. Movement amplitude was approximately 30 cm and was specified by practising with a ruler held beside the moving hand. Movements should be performed fast, but not necessarily at maximum speed. In between individual movements, breaks of 1- to 2-s duration were introduced. Eighteen upward and downward movements were recorded. The weight of the object generated a constant gravitational load, and the inertial forces due to acceleration and deceleration of the object produced additional dynamic loads (Fig. 1).

a Autonomous grip object containing sensors to measure grip force (GF) and three-dimensional accelerations (AccX, -Y, -Z). The load (LF) was calculated from the mass (m), gravity (G), and accelerations (see text). b Vertical acceleration (AccZ, gravitational acceleration subtracted), load (LF), and grip force (GF) in a control subject during an upward and a downward directed movement. The broken lines indicate: 1 start of the upward movement, 2 maximum upward acceleration and maximum load, 3 start of downward movement, 4 maximum downward acceleration and minimum load, 5 maximum downward deceleration and maximum load
The object contained a force sensor to measure grip force (Rieger ETMS, 0 to 80 N, accuracy ±0.1 N) and three acceleration sensors to measure accelerations in three spatial dimensions (ICS 3021, ±50 m/s2, accuracy ±0.2 m/s2). By means of internal electronics, the data were A/D-converted (12 bit) with a sampling rate of 100 Hz and stored inside the object. After the experiment, the object was connected to a PC for data transfer. During data registration, the object was completely autonomous with no connection to external devices.
From the acceleration signals the load force (LF) was determined as the vectorial summation of the load due to the object‘s weight (acting vertically: m×G) and the acceleration-dependent inertial loads in the vertical Z direction and in the horizontal Y directions (m×AccZ, m×AccY, see Fig. 1). The corresponding vertical and horizontal loads acted tangentially to the grip surface and therefore had to be compensated for by the grip. Loads acting orthogonally to the grip surfaces due to X accelerations (see Fig. 1) were not considered since they do not directly destabilize the grip. However, post hoc data analysis showed that accelerations other than in the Z direction were small, suggesting that the object was moved quite precisely along the vertical axis with only minor rotations and tilts. The load force was calculated as follows: LF=m×sqrt[(AccZ + G)2 + AccY2]. The start of an upward or downward movement was obvious from an upward or downward deviation of the vertical acceleration from its baseline (time points 1 and 3 in Fig. 1). Maxima of acceleration were determined for upward and downward movements (time points 2 and 4). Maxima of load occurred early during upward movements (time point 2) and late during downward movements when downward deceleration was greatest (time point 5). Maximum grip force was determined for each movement. In control subjects, the grip maximum typically coincided with the load maximum (Fig. 1). Maximum grip force was considered as a measure of grip force economy. To quantify the modulation of the grip force with the load force, the gain of the relationship between both forces was calculated in a defined time interval. The interval between movement start and the next peak in the load profile (upward: interval between time points 1 and 2, downward: intervals between time points 3 and 4) was selected for linear regression, and the resulting slope corresponded with the gain of the modulation. The gain of modulation indicates whether the grip force is programmed in advance of the movement to change in parallel with the load profile, which depends on the direction of the movement.
Eight subjects with unilateral or bilateral cerebellar pathology (five males, three females aged between 40 years and 76 years, mean age 56.7 years) took part in the experiment. Five patients presented with degenerative cerebellar disorders, two with spinocerebellar ataxia type 6 (SCA6: CA 2 and CA 4), and three with idiopathic cerebellar ataxia (IDCA: CA 1, 3, 7). Three patients had focal cerebellar lesions: two presented with cerebellar ischemic lesions (left superior cerebellar artery: SUCA 6; left posterior inferior cerebellar artery: PICA 8), and one with a surgical lesion (removal of an aneurysm and cyst in the right cerebellar hemisphere: OP 5). The patients with degenerative cerebellar disorders revealed moderate to severe cerebellar ataxia, whereas the degree of cerebellar ataxia was mild in the patients with focal cerebellar lesions. There were no relevant extra-cerebellar signs based on a detailed neurological examination. None of the patients revealed sensory abnormalities including proprioception. Cranial MRI (magnetic resonance imaging) scans showed moderate to severe cerebellar atrophy in the five patients with degenerative disorders and focal lesions of either hemisphere in the three patients with focal lesions. Eight age and gender matched healthy subjects (five males, three females, aged between 40 years and 76 years, mean age 57.0 years) served as the control group. Subjects gave their informed consent according to the Declaration of Helsinki. The study was approved by the local ethics committee. Subjects with unilateral cerebellar damage performed the tasks with the affected hand; subjects with bilateral damage used their dominant hand. Hand-dominance matched control subjects performed the experiments with the same hand as the corresponding patient.
Results
Figure 1b shows the performance of a healthy control subject. During the upward movement, the maximum load occurred at maximum acceleration early in the movement; the deceleration was supported by the weight of the object. During the downward movement, the initial downward acceleration was supported by the weight and the net load was near zero during the first movement phase; the maximum load occurred during deceleration close to the end of the movement. Grip force anticipated the load force profile. Thus, maximum values in grip and load force occurred nearly simultaneously. In addition, the grip force increased with increasing load right from the start of the upward movement. During the downward movement, a slight decrease in the grip force profile with decreasing load is obvious, the grip force modulation being less brisk than in the case of the upward movement.
In Fig. 2, examples of load and grip force profiles obtained from successive upward and downward directed movements are shown for each cerebellar patient. The load profile (grey line) directly results from the acceleration of the object and therefore reflects the kinematics of the arm movement. Comparison with the load profile of the control subject in Fig. 1b indicates that patients CA 1, CA 3, and CA 4 moved with normal kinematics characterized by distinct acceleration and deceleration phases for both movement directions with no additional irregularities in the load profile (the irregularity in the load profile near zero in patient CA 3 results from a change in load direction, not from irregular movement). In the other patients, irregularities in the load profile probably resulted from primary motor disorders such as tremor or ataxia of the arm movements. Patients CA 2 and CA 7 were most seriously affected. Nevertheless, each patient produced load profiles that were consistent with the characteristic pattern for upward and downward movements.

Loads (grey) and grip forces (black) during single successive upward and downward movements with the grasped object produced by eight patients with degenerative or focal cerebellar lesions. The shaded area indicates the duration of the movement, the left border corresponding with movement onset. Arrows indicate maxima of load (grey) and grip force (black)
A comparison of the occurrence of maxima in load and grip force (cf. grey and black arrows in Fig. 2) revealed frequent aberrations from the synchronicity observed in healthy control subjects (cf. Fig. 1b). During the upward movement of patients CA 1, CA 3, CA 4, OP 5, and CA 7, the maximum grip force usually lagged behind maximum load. During downward movements, the delays between maximum load and grip forces were typically smaller than during upward movements but were usually longer than that for control subjects (cf. Fig. 1b). Inspection of the force profiles close to the start of the upward movement revealed an absent or even decreasing grip force response despite increasing loads in some of the patients (most obvious in patients OP 5 and CA 7). A comparable paradox modulation of grip force with the load was also evident at the start of downward movements when grip force increased despite a decrease in the load (see the movements of patients CA 3, SUCA6, and CA 7). Notably, a disturbed modulation of grip force with the movement-induced load seems to be associated with impaired load production due to irregularities of the arm in some patients (see CA 7), while in other patients, these two aspects of performance seem to dissociate. For example, the force coupling was disturbed in patient CA 3 despite normal arm movements, and patients CA 2 and PICA 8 modulated their grip force in parallel with irregular load force profiles resulting from impaired smoothness of the arm movement.
Figure 3 shows variables characterizing task performance for each patient averaged across movements in each movement direction. The upper graph indicates that the maximum grip forces of patients were increased compared to controls (Mann-Whitney U-test, up: P=0.021, down: P=0.038). The overshoot of grip forces could already be inferred from the labelling of the grip force axes in Fig. 2. Figure 3 seems to suggest that the grip force output was especially pronounced in patients with degenerative cerebellar disease. However, since there were only three patients with very different focal lesions, such a conclusion should be drawn with care. Since the maximum accelerations and the resulting maximum loads produced by patients did not differ from those produced by healthy control subjects (up and down: P>0.2: compare Figs. 2, 1b), the harder grip found for patients cannot be attributed to greater loads.

Maximum grip force and gain of GF/LF modulation averaged across all upward and downward directed movements. For control subjects, group mean and standard deviation is indicated, for patients, individual performance is displayed. The gain of modulation was calculated from the linear regression of grip force versus load during the first movement phase (cf. Methods). Note that in the gain plot the symbols for some patients are overlapping (up: CA 1, 2, 3; down: CA 1, 3, 7)
The gain of modulation of grip force with load force displayed in Fig. 3 clearly confirms our qualitative description of individual performance (Figs. 1b, 2). The increase in grip force with increasing load at the beginning of an upward movement and the decrease in grip force with decreasing load at the beginning of a downward movement is typical for healthy subjects and results in a positive gain of modulation. A negative gain indicates disturbed modulation and is evident for movements of single patients in Fig. 3, regardless of movement direction. Abnormally high gains, either positive or negative, suggest an exaggerated grip response to a change in load.
Discussion
Predictive grip force control during transport movements of a grasped object was clearly impaired in patients with cerebellar disease.
Patients produced excessive grip forces. This finding is in accordance with other studies on grip force control during object manipulation in comparable patient samples (Babin-Ratté et al. 1999; Fellows et al. 2001; Nowak et al. 2002b; Rost et al. 2004). Grip force increase may directly reflect impaired motor function or may be a strategic response to motor deficits, such as ataxia or tremor. The strategic response may be adequate for preserving grip despite ataxic arm movements, or may be exaggerated causing uneconomically high grip forces. Grip force increases were also reported under conditions of sensory deficits of the hands due to peripheral or central pathologies (Nowak et al. 2001a, 2004; Augurelle et al. 2003; Hermsdörfer et al. 2003). Basal ganglia disease, such as Parkinson’s disease, may also be associated with an excessive grip force output, especially in situations of drug-induced dyskinesias (Fellows et al. 1998; Gordon et al. 1997; Wenzelburger et al. 2002). Also, an isolated deficit of spinal and cortical motor pathways as observed in motor neuron disease may induce an exaggerated grip force output (Nowak et al. 2003). Therefore, an increase in grip force appears to be a more general phenomenon and many central and peripheral sensorimotor structures are involved in the scaling of the grip force level. Abnormal grip force levels in patients should therefore not be considered an unequivocal indicator of disturbed predictive force control and a dysfunction of the internal model.
The modulation of the patient’s grip force profile with the self-generated load exhibited clear deteriorations from normal performance. The data of individual patients suggested that grip force peaks did not anticipate the peaks in load force as observed in control subjects. In patients, both forces were desynchronized. A delay in the grip force peak in relation to the load force peak may indicate a rather feedback-based than a predictive control mechanism to compensate for the changes in load destabilizing the grip. In addition, the gain of the modulation deviated from normal values, regardless of the movement direction. During downward movements, the gain was negative in five out of eight patients, indicating that the initial load decrease was accompanied by an early paradoxical grip force increase. This may indicate that patients regulate their fingertip forces in a stereotypical way increasing grip force at the beginning of the movement irrespective of movement direction. However, the finding that two patients relaxed the grip paradoxically at the beginning of upward movements (CA 7 and OP 6 in Fig. 3) does not support such a hypothesis. Since the gain was calculated for a very early phase during the movement, the observed deficits suggest a failure in the planning of the grip force profile in anticipation of the direction-dependent load force variation.
The finding of impaired grip force/load modulation in the cerebellar patients is in accordance with studies using comparable motor tasks (Babin-Ratté et al. 1999; Nowak et al. 2002b; Rost et al. 2004). For example, during cyclic vertical movements with a grasped object, cerebellar patients produced grip force profiles which only coarsely matched the oscillation in the load force profiles (Rost et al. 2004). Other authors used tasks, which involved grasping, lifting, or pulling a drawer to demonstrate impaired coupling between grip force and load in cerebellar disorders (Fellows et al. 2001; Müller and Dichgans 1994; Serrien and Wiesendanger 1999). Despite the fact that performance in these kinds of tasks could be more easily influenced by inaccurate posturing of the hand and arm, the concordant results may, nevertheless, suggest that the lack of coordination and anticipation of finger forces is a more general consequence of cerebellar dysfunction.
In extension of our earlier work in patients with cerebellar degeneration using a comparable paradigm (Nowak et al. 2002b), the present study reveals that also focal unilateral cerebellar damage can cause deficits in the grip force/load coupling of the ipsilesional hand. A related finding was reported in a study of grip force control during grasping and lifting movements in patients with cerebellar degeneration and cerebellar vascular disorders (Fellows et al. 2001). Grip force coordination was impaired in patients with degeneration and in patients with focal lesions in the region of the superior cerebellar artery (SUCA), while infarction of the territory of the posterior inferior cerebellar artery (PICA) caused less impairment. The location of the lesion also appears critical from the results of the present study, since the patient with the PICA lesion (PICA 8) was less impaired than the patient with the SUCA lesion (SUCA 6) and the patient with the surgically caused focal lesion (OP 5). In agreement with the poor performance, the lesion was particularly extensive in patient OP 5 and included large parts of the cerebellar hemisphere and of the cerebellar output nuclei. However, the small sample size does not allow more definite conclusions about the correlation between lesion location and performance deficits. The present results also suggest that the efficiency of grip force scaling may be less affected in patients with focal lesions than in patients with global degeneration (Fig. 3). Apart from differences in structural brain damage, it may be speculated that preserved ipsilesional and unaffected contralateral cerebellum compensates for ipsilateral damage in the patients with focal lesions and/or these patients may benefit from daily experience with their unimpaired hand.
Although the present results confirm a major role of the cerebellum in grip force prediction, direct attribution of this function exclusively to cerebellar processing is not possible. First, extra-cerebellar lesions also cause deficits of the grip force/load modulation. Thus, the predictive grip force regulation may also be impaired in some patients with cortical lesions, in patients with pure motor-neuron disorder, such as amyotrophic lateral sclerosis, and in cases of complete peripheral sensory deafferentation (Hermsdörfer et al. 2003, 2004; Nowak et al. 2003, 2004). Second, it is difficult to disentangle any effects of cerebellar motor deficits, such as hypermetria, ataxia, and tremor on the grip force/load modulation. As we found a dissociation of performance deficits for arm movements kinematics and grip force coupling in individual patients (Fig. 2) and the grip force deficits were in general not strongly correlated with ataxia scores (Rost et al. 2004), a major influence of the underlying disorder on grip force prediction seems unlikely but cannot be excluded.
Imaging techniques are well suited to further pursue the question regarding the anatomical representation of grip force prediction, while at the same time avoiding the problems frequently encountered by lesion studies, as discussed above. We used PET in healthy subjects to determine the cerebral structures particularly devoted to the coupling between grip force and self-generated loads during object manipulation.
The representation of grip force/load modulation as revealed by PET
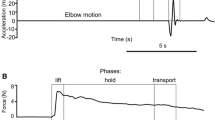
Recently, we examined the functional anatomical correlates of predictive motor control by H 152 O PET in healthy subjects performing an automatized grip force/load force coupling task (Boecker et al. 2005). Differing from the clinical study reported above, load forces were not produced by object movements, but by pulling a grasped object against a fixed resistance. In this case, the load was produced isometrically without associated arm movements. Figure 4a shows the experimental setup and Fig. 4b displays exemplary grip force and load data in a subject undergoing PET. A 2×2 factorial design was chosen to reveal the interaction effect of the grip force/pull force coupling. The factors were pull force (with/without associated grip force modulation) and grip force (with/without associated pull force generation). In the experimental condition (grip and pull force coupled), subjects were requested to pull the grasped object against an isometric resistance. This induced simultaneous modulation of the grip forces with the self-generated load, indicating perfect grip force prediction (Fig. 4b). There were three control conditions: (1) a motor control condition “pull” during which only the pull force was produced while the hand was relaxed, (2) a motor control condition “grip” during which grip force was produced isolated, and (3) a visual control condition during which subjects observed the target movement but no related motor activity occurred. All conditions were tested at three force levels (low, medium, high: 5, 7.5, and 10 N). In the experimental design, grip and load forces were well matched between experimental and motor control conditions (compare Fig. 4b).

a Experimental setup for the production and recording of grip forces (GF) and pull forces (PF) during the PET measurements. b Grip and load force profiles during the four experimental conditions. 20-s intervals for the high force level condition are shown. Experimental condition: the grasped object is pulled against a steel wire indicated by the upper line according to a target signal (0.5 Hz, 2–10 N). Simultaneous and precise modulations of the grip force are produced as obvious from the grip force/pull force plot below the two profiles. Control condition PULL: only the pulling load is produced according to the target, while the hand is relaxed. The steel wire is fixed to the splint at the subject’s forearm (indicated by the lower broken line). Control condition GRIP: only the grip force is produced according to the target. The wire is loosened. REST: only the oscillating target line is visible, no motor activity occurs
The PET measurements were performed on a Siemens Ecat HR+ scanner (Siemens, CTI, Knoxville, TN). Further details concerning data acquisition and analysis with SPM2 (Wellcome Department of Cognitive Neurology, London, UK) are reported elsewhere (Boecker et al. 2005). Eight healthy volunteers (56.8±5.1 years; 4 male, 4 female) participated in the experiments.
As predicted, our analyses (conjunction and interaction) identified force-coupling-related activity in the ipsilateral posterior cerebellum (Fig. 5). Furthermore, force-coupling-related effects were recorded in the anterior cingulate and the frontal association regions, the right caudate nucleus, and the left lingual gyrus. Importantly, activity did not depend on the force level, since force-dependent masking did not change the main findings.

PET data: interaction effect reflecting grip force–pull force coupling (at P<0.05, FDR corrected) in the ipsilateral posterior cerebellar hemisphere. The PET rCBF data are superimposed onto three orthogonal MRI sections. The left side of the brain corresponds to the left hemisphere (adapted from Boecker et al. 2005)
Our findings are in general accordance with recent neuroimaging studies suggesting that the cerebellum is a principal site involved in storage (Imamizu et al. 2000), retrieval (Kawato et al. 2003), and switching (Imamizu et al. 2003) of internal models. The anticipatory synchronous modulation of grip force with the changing load force was more specifically characterized as forward internal model to emphasize its predictive character (cf. Introduction). So far, only two studies have investigated the central representation of forward internal models with fMRI using a grip force control paradigm (Ehrsson et al. 2003; Kawato et al., 2003). Compared to studies on newly acquired motor representations, a major advantage of the use of grip-load force coupling tasks in experimental designs is that grip force control represents a completely automated control mechanism that is not subject to online conscious control. Hence, neuronal activity related to learning per se is only of minor importance. However, the existing fMRI data have some disadvantages with respect to the functional contribution of the cerebellum in predictive grip force control. For example, one study did not measure the forces resulting from the behavioural task during fMRI acquisitions, thus rendering the interpretation of the described cerebellar activation changes difficult (Kawato et al. 2003). Nevertheless, force-coupling-related activity was detected in the cerebellum at a very similar, however contra-lateral site, within the posterior cerebellum. In another fMRI study, the cerebellum was outside their field of view of the fMRI scanner (Ehrsson et al. 2003). This study favoured the intraparietal cortex as the anatomical region specifically engaged in the predictive grip force/load force coupling, but less in the isolated production of either grip or load forces.
We have shown that the ipsilateral cerebellum plays a major role in predictive force coupling, presumably by connected processing throughout cerebro-cerebellar networks. The processing seems to be independent of the generated force level, suggesting that a generalized model can be scaled according to the actual force requirements.
Conclusion
The clinical and brain imaging studies under discussion here point to a major role of the cerebellum in predictive grip force control during object manipulation. The major advantage of combining both experimental approaches to investigate predictive force control is that one approach compensates for the limitations of the other. Interestingly, the lesion study and the imaging study provided converging results on one important aspect of cerebellar function. Despite this evidence our results should not be interpreted as direct proof that the cerebellum is the only anatomical substrate for predictive force control. From clinical data, it is obvious that also non-cerebellar lesions may impair grip force/load coupling. Our brain imaging study also has revealed extra-cerebellar activation related to the force coupling, and other structures involved may have been dismissed because either their activity was weak or they also participated in the isolated load and grip force production tested under control conditions. Nevertheless, the clinical data suggest that the role of the cerebellum is essential and the deteriorating effects of a structural lesion to the cerebellum cannot be compensated by other brain structures.
The sites of cerebellar activation found in different imaging studies, including the posterior cerebellum in our study, and the behavioural observation of selective deficits in patients with circumscribed cerebellar lesions promotes further speculation on the anatomical location of different forms of internal forward or inverse models (Boecker et al. 2005; Imamizu et al. 2003; Kawato et al. 2003). The cerebellar activation peak found in our PET study is located within Crus II neighbouring Crus I of the cerebellar hemisphere (Schmahmann et al. 2000). This region was affected by atrophy in all patients with cerebellar degeneration. Coincidence between PET activation, lesion site, and motor deficit was also obvious in patient OP 5. The coincidence was less obvious in patient SUCA 6 with moderately impaired performance but a lesion only neighbouring Crus II, and patient PICA 8 with relatively good performances but a lesion probably extending into Crus II. Discrepancies may arise from individual differences in the cerebellar representation of the internal model. Also, the fact that loads were produced by movements in the clinical study and isometrically in the PET study may have caused different locations of the cerebellar representation (cf. Imamizu et al. 2003). However, grip force/load force modulation has been tested only in small numbers of patients with focal lesions so that definite conclusions are not possible. Future work should include larger patient samples with focal lesions at various anatomical sites to enable reasonable comparisons with imaging findings in healthy subjects.
One particularly interesting conclusion derived from both lesion and imaging studies is the obvious independence of the control mechanisms to scale the grip force level and to regulate the coupling between grip force and load. Thus, a grip force overshoot was found with a variety of neurological disorders including cerebellar disease, but the deficit of force scaling was not correlated with deficits in grip force modulation (Rost et al. 2004; Hermsdörfer et al. 2003). Imaging data are consistent with this finding, indicating that cerebellar activity is closely related to grip/load force coupling, but does not depend on the force level. Thus, controlling the level of grip force and modulating the grip force with self-generated loads appear to be to largely independent processes which are mediated by different brain structures. The close temporal coupling between grip and load forces strongly depends on a normal cerebellar function.
References
Augurelle AS, Smith AM, Lejeune T, Thonnard JL (2003) Importance of cutaneous feedback in maintaining a secure grip during manipulation of hand-held objects. J Neurophysiol 89:665–671
Babin-Ratté S, Sirigu A, Gilles M, Wing A (1999) Impaired anticipatory finger grip-force adjustments in a case of cerebellar degeneration. Exp Brain Res 128:81–85
Blakemore SJ, Frith CD, Wolpert DM (1999) Spatio-temporal prediction modulates the perception of self-produced stimuli. J Cogn Neurosci 11:551–559
Blakemore SJ, Frith CD, Wolpert DM (2001) The cerebellum is involved in predicting the sensory consequences of action. NeuroReport 12:1879–1884
Boecker H, Lee A, Mühlau M, Ceballos-Baumann AO, Ritzl A, Spilker M, Marquardt C, Hermsdörfer J (2005) Force level independent representations of predictive grip force–load force coupling: a PET activation study. Neuromage (in press)
Danion F (2004) How dependent are grip force and arm actions during holding an object? Exp Brain Res 158:109–119
Ehrsson HH, Fagergren A, Johansson RS, Forssberg H (2003) Evidence for the involvement of the posterior parietal cortex in coordination of fingertip forces for grasp stability in manipulation. J Neurophysiol 90:2978–2986
Fellows SJ, Schwarz M, Noth J (1998) Precision grip and Parkinson’s disease. Brain 121:1771–1784
Fellows SJ, Ernst J, Schwarz M, Töpper R, Noth J (2001) Precision grip deficits in cerebellar disorders in man. Clin Neurophysiol 112:1793–1802
Flanagan JR, Johansson RS (2002) Hand movements. Encyclopedia of the human brain. Elsevier, New York, pp 399–414
Flanagan JR, Tresilian J (1994) Grip-load force coupling: a general control strategy for transporting objects. J Exp Psychol Human Perform 20:944–957
Flanagan JR, Wing AM (1993) Modulation of grip force with load force during point-to-point arm movements. Exp Brain Res 95:131–143
Flanagan JR, Wing AM (1995) The stability of precision grip forces during cyclic arm movements with a hand held load. Exp Brain Res 105:455–464
Flanagan JR, Wing AM (1997) The role of internal models in motion planning and control-evidence from grip force adjustments during movements of hand-held loads. J Neurosci 17:1519–1528
Flanagan JR, Vetter P, Johansson RS, Wolpert DM (2003) Prediction precedes control in motor learning. Curr Biol 13:146–150
Forssberg H, Jucaite A, Hadders-Algra M (1999) Shared memory representations for programming of lifting movements and associated whole body postural adjustments in humans. Neurosci Lett 273:9–12
Gordon AM, Ingvarsson PE, Forssberg H (1997) Anticipatory control of manipulative forces in Parkinson’s disease. Exp Neurol 145:477–488
Hermsdörfer J, Marquardt C, Philipp J, Zierdt A, Nowak DA, Glasauer S, Mai N (2000) Moving weightless objects: grip force control during microgravity. Exp Brain Res 132:52–64
Hermsdörfer J, Hagl E, Nowak DA, Marquardt C (2003) Grip force control during object manipulation in cerebral stroke. Clin Neurophysiol 114:915–929
Hermsdörfer J, Hagl E, Nowak DA (2004) Deficits of anticipatory grip force control after damage to peripheral and central sensorimotor systems. Hum Mov Sci 23:643–662
Imamizu H, Miyauchi S, Tamada T, Sasaki Y, Takino R, Putz B, Yoshioka T, Kawato M (2000) Human cerebellar activity reflecting an acquired internal model of a new tool. Nature 403:192–195
Imamizu H, Kuroda T, Miyauchi S, Yoshioka T, Kawato M (2003) Modular organization of internal models of tools in the human cerebellum. Proc Natl Acad Sci USA 100:5461–5466
Jenmalm P, Johansson RS (1997) Visual and somatosensory information about object shape control manipulative fingertip forces. J Neurosci 17:4486–4499
Johansson RS (1998) Sensory input and control of grip. Sensory Guid Move 218:45–63
Johansson RS, Cole KJ (1992) Sensory-motor coordination during grasping and manipulative actions. Curr Opin Neurobiol 2:815–823
Johansson RS, Westling G (1984) Roles of glabrous skin receptors and sensorimotor memory control of precision grip when lifting rougher or more slippery objects. Exp Brain Res 56:550–564
Johansson RS, Westling G (1988) Coordinated isometric muscle commands adequately and erroneously programmed for the weight during lifting tasks with precision grip. Exp Brain Res 71:59–71
Johansson RS, Riso R, Häger C, Bäckström L (1992) Somatosensory control of precision grip during unpredictable pulling loads. I. Changes in load force amplitude. Exp Brain Res 89:181–191
Kawato M (1999) Internal models for motor control and trajectory planning. Curr Opin Neurobiol 9:718–727
Kawato M, Kuroda T, Imamizu H, Nakano E, Miyauchi S, Yoshioka T (2003) Internal forward models in the cerebellum: fMRI study on grip force and load force coupling. Prog Brain Res 142:171–188
Massion J (1992) Movement, posture and equilibrium: interaction and coordination. Prog Neurobiol 38:35–56
Miall RC, Wolpert DM (1996) Forward models for physiological motor control. Neural Networks 9:1265–1279
Miall RC, Weir DJ, Wolpert DM, Stein JF (1993) Is the cerebellum a Smith predictor? J Motor Behav 25(3):203–216
Müller F, Dichgans J (1994) Dyscoordination of pinch and lift forces during grasp in patients with cerebellar lesions. Exp Brain Res 101:485–492
Nowak DA, Hermsdörfer J (2003) Digit cooling influences grasp efficiency during manipulative tasks. Eur J Appl Physiol 89:127–133
Nowak DA, Hermsdörfer J, Glasauer S, Philipp J, Meyer L, Mai N (2001a) The effects of digital anaesthesia on predictive grip force adjustments during vertical movements of a grasped object. Eur J Neurosci 14:756–762
Nowak DA, Hermsdörfer J, Philipp J, Marquardt C, Glasauer S, Mai N (2001b) Effects of changing gravity on anticipatory grip force control during point-to-point movements of a hand-held object. Motor Control 5:231–253
Nowak DA, Glasauer S, Meyer L, Mai N, Hermsdörfer J (2002a) The role of cutaneous feedback for anticipatory grip force adjustments during object movements and externally imposed variation of the direction of gravity. Somatosens Motor Res 19:49–60
Nowak DA, Hermsdörfer J, Marquardt C, Fuchs HH (2002b) Load force coupling during discrete vertical movements in patients with cerebellar atrophy. Exp Brain Res 145:28–39
Nowak DA, Hermsdörfer J, Topka H (2003) When motor execution is selectively impaired: Control of manipulative finger forces in amyotrophic lateral sclerosis. Motor Control 7:304–320
Nowak DA, Glasauer S, Hermsdörfer J (2004) How predictive is grip force control in the complete absence of somatosensory feedback? Brain 127:182–192
Ostry DJ, Feldman AG (2003) A critical evaluation of the force control hypothesis in motor control. Exp Brain Res 153:275–288
Rost K, Nowak DA, Timmann D, Hermsdörfer J (2004) Preserved and impaired aspects of predictive grip force control in cerebellar patients. Clin Neurophysiol (in press)
Schmahmann JD, Doyon J, Toga AW, Petrides M, Evans AC (2000) MRI atlas of the human cerebellum. Academic, San Diego
Serrien DJ, Wiesendanger M (1999) Grip-load force coordination in cerebellar patients. Exp Brain Res 128:76–80
Todorov E, Jordan MI (2002) Optimal feedback control as a theory of motor coordination. Nat Neurosci 5:1226–1235
Wenzelburger R, Zhang BR, Pohle S, Klebe S, Lorenz D, Herzog J, Wilms H, Deuschl G, Krack P (2002) Force overflow and levodopa-induced dyskinesias in Parkinson’s disease. Brain 125:871–879
Wing AM (1996) Anticipatory control of grip force in rapid arm movement. In: Wing AM, Haggard P, Flanagan JR (eds) Hand and brain. Academic, San Diego, pp 301–324
Witney AG, Wing A, Thonnard JL, Smith AM (2004) The cutaneous contribution to adaptive precision grip. Trends Neurosci 27:637–643
Wolpert DM (1997) Computational approaches to motor control. Trends Cogn Sci 1:209–216
Wolpert DM, Flanagan JR (2001) Motor prediction. Curr Biol 11:R729–R732
Wolpert DM, Kawato M (1998) Multiple paired forward and inverse models for motor control. Neural Networks 11:1317–1329
Wolpert DM, Ghahramani Z, Jordan MI (1995) An internal model for sensorimotor integration. Science 269:1880–1882
Wolpert DM, Miall RC, Kawato M (1998) Internal models in the cerebellum. Trends Cogn Sci 2:338–347
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by: Irene Ruspantini and Niels Birbaumer
Rights and permissions
About this article
Cite this article
Hermsdörfer, J., Nowak, D.A., Lee, A. et al. The representation of predictive force control and internal forward models: evidence from lesion studies and brain imaging. Cogn Process 6, 48–58 (2005). https://doi.org/10.1007/s10339-004-0042-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10339-004-0042-y