
Abstract
Objective
Compensatory sweating (CS) is the most common adverse event and the main cause of dissatisfaction among patients undergoing a VATS sympathectomy for the treatment of primary hyperhidrosis. It has been described that obese individuals experience more sweating than thinner ones. The aim of this study is to identify the Body Mass Index (BMI) and the level of resection as predictive factors for CS and its relation to levels of patient satisfaction following the procedure.
Methods
From October 1998 to June 2003, 102 patients undergoing VATS sympathectomies (51 for palmar hyperhidrosis, PH, and 51 for axillary hyperhidrosis, AH) were prospectively surveyed. They were divided into three groups according to their BMI: Group I was composed of 19 patients with BMI<20 (9 patients with PH and 10 with AH); Group II was composed of 52 patients with 20 ≤BMI<25 (25 with PH and 27 with AH); and Group III was composed of 31 patients with BMI ≥ 25 (17 with PH and 14 with AH). Each procedure was simultaneously and bilaterally performed under general anesthesia using two 5.5mm trocars and a 30° optic system.
Results
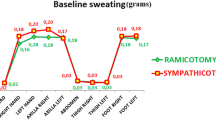
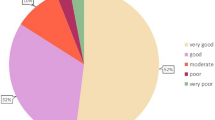
Patients treated for PH (resection of T2-T3) had more severe CS than those with AH (resection of T3-T4) (p=0.007) and the greater the BMI, the greater the severity of the CS (p<0.001). No statistically significant difference was found between the BMI bands in relation to the degree of satisfaction (p=0.644), nor when we compared the degree of satisfaction to the degree of CS (p=0.316).
Conclusions
The greater the BMI, the more severe the CS, but this did not correlate with the patients’ level of satisfaction. Avoiding the resection of T2 sympathetic ganglia is also important in reducing the intensity of CS.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Alric P, Branchereau P, Berthet JP, Leger P, Mary H, Mary-Ane C (2002) Video-assisted thoracoscopic sympathectomy for palmar hyperhidrosis: results in 102 cases. Ann Vasc Surg 16(6):708–713
Bray GL (1985) Obesity definition, diagnosis and disadvantages. Med J Aust 142:52–58
De Campos JR, Kauffman P, Werebe EC, Andrade Filho LO, Kusniek S, Wolosker N, Jatene FB (2003) Quality of life, before and after thoracic sympathectomy: report on 378 operated patients. Ann Thorac Surg 76(3):886–891
Doblas M, Gutierrez R, Fontcuberta J, Orgaz A, Lopez P, Criado E (2003) Thoracodorsal sympathectomy for severe hyperhydrosis: posterior bilateral versus unilateral staged sympathectomy. Ann Vasc Surg 17(1):97–102
Drott C, Gothberg G, Claes G (1995) Endoscopic transthoracic sympathectomy: an efficient and safe method for the treatment of hyperhidrosis. J Am Acad Dermatol 33(1):78–81
Ferro-Luzzi A, Sette S, Franklin M, James WPT (1992) A simplified approach to assessing adult chronic energy deficiency. Eur J Clin Nut 46:173–186
Gossot D, Toledo L, Fritsch S, Celerier M (1997) Thoracoscopic sympathectomy for upper limb hyperhidrosis: looking for the right operation. Ann Thorac Surg 64(4):975–978
James WPT, Ferro-Luzzi A, Waterlow JC (1988) Definition of chronic energy deficiency in adults. Report of working party of the International Dietary Energy Consultative Group. Eur J Clin Nut 42:961–981
Kenchaiah S, Evans JC, Levy D, Wilson, PWF, Benjamim EJ, Larson MG, Kannel WB, Vasan RS (2002) Obesity and the risk of heart failure. N Engl J Med 347(5):305–313
Lai YT, Yang LH, Chio CC, Chen HH (1997) Complications in patients with palmar hyperhidrosis treated with transthoracic endoscopic sympathectomy. Neurosurgery 41(1):110–115
Lecerf JM, Reitz C, De Chasteigner A (2003) Evaluation of discomfort and complications in a population of 18,102 overweight or obese patients. Presse Med 32(15):689–695
Leseche G, Castier Y, Thabut G, Petit MD, Combes M, Cerceau O, Besnard M (2003) Endoscopic transthoracic sympathectomy for upper limb hyperhidrosis: limited sympathectomy does not reduce postoperative compensatory sweating. J Vasc Surg 37(1):124–128
Lin CC, Wu HH (2001) Lin-Telaranta classification: the importance of different procedures for different indications in sympathetic surgery. Ann Chir Gynaecol 90(3):161–166
Moran KT, Brady MP (1991) Surgical management of primary hyperhidrosis. Br J Surg 78(3):279–283
O’Riordain DS, Maher M, Waldron DJ, O’Donovan B, Brady MP (1993) Limiting the anatomic extent of upper thoracic sympathectomy for primary palmar hyperhidrosis. Surg Gynecol Obstet 176(2):151–154
Pichard C, Kyle UG (1998) Body composition measurements during wasting diseases. Curr Opin Clin Nutr Metab Care 1(4):357–361
Pietrobelli AAB, Wang ZA, Heymsfield SBA (1998) Techniques used in measuring human body composition. Curr Opin Clin Nutr Metab Care 1(5):439–448
Shachor D, Jedeikin R, Olsfanger D, Bendahan J, Sivak G, Freund U (1994) Endoscopic transthoracic sympathectomy in the treatment of primary hyperhidrosis. A review of 290 sympathectomies. Arch Surg 129(3):241–244
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented as a lecture at the 5th International Symposium on Sympathetic Surgery May 29–31, 2003, Erlangen, Germany.
Rights and permissions
About this article
Cite this article
Ribas Milanez de Campos, J., Wolosker, N., Takeda, F.R. et al. The body mass index and level of resection. Clin Auton Res 15, 116–120 (2005). https://doi.org/10.1007/s10286-005-0259-6
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s10286-005-0259-6