
Abstract
Digital imaging of dental casts has become an alternative to conventional cast analysis in orthodontic treatment planning. The reproducibility of angular measurements made on virtual digital models has not as yet been evaluated. In order to study reproducibility for and agreement between a conventional analysis technique and virtual 3D imaging, 20 dental casts from subjects in the early mixed dentition, were measured twice with each technique by two orthodontists. Variables of interest were incisor rotation, angulation and irregularity, arch width, arch circumference, overjet, and overbite. Standard deviation (Dahlberg 1940) and coefficient of variation were used for evaluation of reproducibility. Mean differences between methods and examiners, correlation between mean differences and mean levels and 95% limits of agreement were used for describing systematic errors. The conventional technique showed less intraexaminer variation for angular variables than the 3D imaging method. Linear variables, with the exception of overbite, showed no clear trend as regards differences in reproducibility between the two methods. In general, examiner 1 showed less intraexaminer variation than examiner 2. The mean differences between the two methods expressed higher values for assessment of rotations with the O3DM method. Both angular and linear variables exhibited poor 95% limits of agreement. The conventional technique showed better overall reproducibility and thus appears to be more suitable for scientific work. However, the reproducibility attained by O3DM is clearly acceptable for clinical use. The two methods should not be used interchangeably.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Dental casts have traditionally been used for orthodontic diagnosis and treatment planning. Tooth size, arch length discrepancies, overjet, and overbite are routinely measured and recorded. Rotation of incisors, a factor assumed to be of great importance as an indicator of post retention stability,2–4 is subjectively noted but seldom measured in the daily clinical work. Little’s irregularity index5 which measures the deviation of proximal contact point in anterior tooth segments is widely used to express incisor alignment. When it comes to the depiction of tooth rotation this index is of limited value since the outcome measure of the index represents a combined effect of tooth rotation and tooth inclination. Probably, these two components of a deviated tooth position have different etiology. Thus, a post-treatment change in irregularity index gives no hint about the reason for relapse of orthodontic treatment results.4,6,7
The introduction of modern computer-based orthodontic record systems with integrated digital photos and radiographic pictures will probably lead to the replacement of plaster casts with virtual digital models in the near future. There are a number of companies such as OrthoCad (Cadent Inc. 640 Gotham Parkway, Carlstadt, NJ, USA), OrthoProof (5620 Venice Ave NE, Suite G, Albuquerque, New Mexico, USA), and O3DM (O3DM Thunoegade 1, 8000 Aarhus C, Denmark) that offers software programs for analysis of digital models of both linear and angular parameters. Treatment planning and follow-up examinations would surely benefit from having total access to patient data, images of dental casts, and records of both linear and angular measurements available in digital format displayed on the monitor, provided measurement accuracy is acceptable. It must be pointed out that the digital technique offers a great opportunity to register reproducible reference points to be used in orthodontic treatment planning.
Earlier studies of reproducibility of recordings of tooth width, Bolton analysis, and dental arch width have shown that measurements with calliper and plaster casts exhibit equal or less variability than measurements based on software programs using virtual digital models.8–10 Accuracy of measurement regarding overjet and overbite show divergent results when virtual digital techniques are compared to conventional techniques using calliper and plaster casts.9,11–15 In spite of this, the reproducibility of both digital and more conventional techniques was regarded as sufficiently good and considered acceptable for clinical use.8–11,13,15–18 Difficulties in properly identifying landmarks on 3D models were mentioned as a probable cause of variability affecting accuracy.10,11,15–17,19 A certain amount of time to get familiar with the software programs during measurement on digital models is required and has been described as a cause of interexaminer variability.9–11,15,16,18
To the best of our knowledge, no studies of angular measurement accuracy on digital dental casts have been published, despite the fact that tooth rotation is of fundamental importance in orthodontic treatment planning and evaluation of post-treatment stability.4 The purpose of this study, therefore, was to investigate the reproducibility of and agreement between a traditional technique and the O3DM system.
Materials and Methods
The research ethics committee, Regionala Etikprövningsnämnden, Stockholm, Sweden, granted ethical approval for this study.
Twenty sets of plaster models were consecutively sampled from subjects participating in a study to examine spontaneous alignment of incisors and arch form changes following extraction of deciduous canines. Because all subjects presented early mixed dentitions, the positions of a number of lateral incisors could not be measured due to insufficient eruption and crowding. Lateral incisors with less than half of the clinical crown erupted were excluded from measurement of angulation. In one model, a tooth (31) was fractured and consequently excluded.
Alginate impressions of the dental arches were taken by the patients’ general practitioners and dental stone models were made using BESV, BE-stone, white, Bo Ehrlander AB, Gothenburg, Sweden. The plaster models were sent to ORTOLAB (ORTOLAB Sp. z.o.o.-ul. Krotka 29/31-42–200 Czestochowa, Poland) for scanning and conversion into 3D virtual models in the O3DM basic version 1.4.00 software program (O3DM Thunoegade 1, 8000 Aarhus C, Denmark). The file format of the O3DM software program is proprietary and closed.
Variables of interest were the rotation, angulation (mesio-distal inclination), and irregularity (displacement of contact points) of maxillary and mandibular incisors, and the overjet, overbite, arch circumference, and arch width. Two orthodontists with 6 and 30 years of orthodontic experience respectively (examiner 1 and 2), carried out the recordings of all variables using both the conventional and virtual digital techniques (O3DM). Written instructions were presented to both examiners on how to perform the measurements. Both examiners underwent an 8-h introduction and calibration of the measuring techniques. After that the recording procedure was carried out with at least 2 weeks between measurement sessions. The recordings were performed in the following order O3DM, conventional, conventional and O3DM technique.
Instrumentation
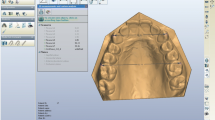
Linear variables were measured directly on the plaster casts with a digital calliper (Digital 6, Mauser, Winterthur, Switzerland) and recorded to the nearest 0.01 mm. A multithreaded wire Ormco Respond.0175 (Ormco Corp, Milwaukee, USA) was used for arch circumference measurements. For angular measurements, photographs were taken of the plaster models with a Konica Minolta Dynax 5D 6.1 mpixel camera (Konica Minolta Holdings Inc, Tokyo, Japan) in a fixed position using a SIGMA 50 mm 1:2,8 DG MACRO D lens (Sigma Corp, NY, USA). The plaster casts were placed in an adjustable rig with a metal plate marking a constructed reference plane (occlusal plane). A dose libel was used to adjust the reference plane so it became parallel and perpendicular to the lens of the camera. Photographs for measurements of rotation were taken with the lens parallel to the occlusal plane at a distance of 17 cm. Pictures for measurements of angulation were taken with the lens perpendicular to the occlusal plane with the buccal surface of the tooth in focus at a distance from the lens of 25 cm. Reference points on the plaster casts and the dose libel were matched to the outer focus frame of the camera in order to get standardized photographs. The digital photographs were imported to the software program Facad 2,2 (Ilexes AB, Linköping, Sweden) and afterwards magnified approximately 2.5 times. Angular measurements were subsequently carried out to the nearest 0.1° (Fig. 1). The digital models in the O3DM basic version 1.4.00 software program could be magnified, re-positioned, and rotated around one point making inspection of the model from any angle possible. Desired reference planes could be determined by selecting any three points. Longitudinal and transversal planes perpendicular to the reference plane were constructed at any point defined by the user. By placing red dot markers on suitable reference points, distances and angles were automatically calculated and recorded with an accuracy of 0.01° and 0.01 mm (Figs. 2, 3, 4 and 5). A Dell computer equipped with standard mouse and 17-inch Dell 1704FPVs monitors with 96 DPI, resolution 1,024 × 768 and 32-bit color were used for measurements with the software programs (Dell Inc, Limerick, Ireland).

Measurements of angulation with the “conventional” technique using a dose libel placed on the metal plate indicating the occlusal reference plane together with markers placed at the centre of the incisal edge and the most apical part of the gingival–enamel junction dissecting the buccal surface into two equal parts.

The blue triangle indicates the originally constructed occlusal reference plane. The blue plane show’s the occlusal plane adjusted vertically to enable reference points for measurements of rotation with the help of a sagittal plane (green).

Arch circumference was measured for both techniques around the dental arch and alveolar bone following a constructed plane here indicated by the blue triangle and blue plane. The O3DM method measured the sum of the segments around the dental arch, here represented by red markers at half the mesiodistal tooth width. The “conventional” method added two measurements from the first molars on each side to the reference point between the incisors.

The triangle indicates the originally constructed occlusal reference plane. The plane show’s the occlusal plane adjusted vertically to enable placing of reference points for indication of the incisal edge. Markers are placed at reference points and at the extension of the incisal edge for measurement of angulation.

Measurements of overjet were performed from a point at the centre of the incisal edge of tooth 41 to a frontal plane intersecting the centre of incisal edge of tooth 11.
Definition of Variables and Measurement Procedures
Reference plane maxilla (occlusal plane)—a plane defined by points at the ideal medial contact point of the upper right incisor and the mesiopalatal cusp tips of the first molars (Fig. 2). Reference plane mandible (occlusal plane)—a plane defined by points at the ideal medial contact point of the lower left incisor and the mesiolingual cusp tips of the first molars. Irregularity—according to Little’s irregularity index.5 Arch circumference—was defined as the distance between the buccal centre of the first permanent molars around the dental arch and alveolar bone following a constructed plane, defined by points placed at the buccal gingival–enamel junction half-way between the central incisors and at half the mesio-distal width of the first permanent molars (Fig. 3). Arch width—was defined as the distance between the mesiolingual cusp tips of the first permanent molars in the mandible, and between the mesiopalatal cusp tips of the first permanent molars in the maxilla. Rotation—was defined as the angle between a subjectively assessed line indicating the longitudinal extension of the incisal edge of the incisor seen in occlusal projection and a perpendicular to a line drawn between the mesiolingual cusp tips of the first permanent molars in the mandible or between the mesiopalatal cusp tips of the first permanent molars in the maxilla (Fig. 2). Angulation—was defined as the angle between a line parallel to the constructed occlusal plane and a line drawn from the centre of the incisal edge (defined as half the mesio-distal crown width) to the most apical part of the gingival–enamel junction dissecting the buccal surface into two equal parts. The side of the angle parallel to the constructed occlusal plane was adjusted to indicate the extension of the incisal edge with O3DM method (Fig. 4). Overjet—was defined as the horizontal distance between incisors 11 and 41 and was measured directly on the plaster casts from the centre of the buccal surfaces. For assessments on the digital models a point to plane technique was used. The measurements were performed from a point at the centre of the incisal edge of the lower left central incisor (41) to a constructed frontal plane (normal to the reference plane of the maxilla) intersecting the centre of the incisal edge of the upper right central incisor (11) (Fig. 5). Overbite—was defined as the vertical distance between incisors 11 and 41 was measured directly on the plaster casts between the centres of the incisal edges. A pencil marking indicating the upper incisor edge was made on the buccal surface of the lower incisor. For assessments on the digital models a point at the centre of the incisal edge of incisor 41 was measured to the reference plane of the maxilla (occlusal plane) levelled to intersect the centre of the incisal edge of incisor 11. Individual reference planes were constructed for measurements of rotation, angulation, and arch circumference.
Statistical Analyses
All analysed variables showed reasonable symmetric normal distributions according to detrended normal QQ-plot and Shapiro Wilks test. Reproducibility of the angular and linear measurements was presented as the standard deviation SD of duplicated measurements according to Dahlberg’s formula (\(s = \pm \surd {\left( {{\Sigma {\text{d}}^{2} } \mathord{\left/ {\vphantom {{\Sigma {\text{d}}^{2} } {2{\text{n}}}}} \right. \kern-\nulldelimiterspace} {2{\text{n}}}} \right)}\))1 and the coefficient of variation COV = (SD/mean) × 10020 for each examiner and method. The mean of the duplicated measurements for each patient under each condition (method and examiner) was calculated and used in the subsequent analyses. Differences in the angular and linear measurements between methods are described and analysed using mean, standard deviation, and 95% confidence interval. The Pearson correlation coefficient with p-values, testing the null hypothesis that the correlation is zero, was calculated between these differences and the means of the two methods. This calculation was made in order to evaluate whether the estimated differences between methods were homogeneous over the range of measurements; 95% limits of agreement (mean difference ± 2*(SD diff)21 was calculated to describe the variation on an individual level. A p-value less than 0.05 was considered statistically significant.
Results
Intraexaminer Variation (Reproducibility)
The statistical analysis showed that the conventional method had a higher reproducibility overall in so far as both examiners had less variation for all variables of maxillary and mandibular incisor rotation, and for all but one of the angular variables (Table 1). Reproducibility of maxillary arch width was also found to be more accurate for both examiners using the conventional technique, while overbite was more accurate with the virtual 3D technique (Table 1).
The analysis of intraexaminer variability showed that there was no conformity between the examiners with regard to mandibular arch width, mandibular and maxillary arch circumference, overjet, and dental irregularity (Table 1).
Examiner 1 displayed less intraexaminer variation for both angular and linear measurements compared to examiner 2 (Table 1).
Intermethod Variation
The O3DM method expressed a tendency for higher values for measurement of rotation. Thus, it was shown that examiner 1 registered higher values for five out of eight incisors measurements, while examiner 2 displayed higher values for all measurements with the O3DM technique compared to the conventional method (Tables 2 and 3). Maxillary arch circumference on the other hand showed significantly lower values for both examiners with the O3DM method. The measurements made by examiner 1 with the O3DM method were significantly higher for rotation at high mean values (Fig. 6, Table 2). Lower values were seen in connection with high mean values for angulation, irregularity, and maxillary arch circumference (Table 2). Examiner 2 showed generally lower values at high means for angular measurements with the O3DM method compared to the conventional technique (Table 3). Both angular and linear variables exhibited poor 95% limits of agreement (Tables 2 and 3).

Measurements of upper incisor rotation (12, 11, 21, 22) by examiner 1. Description of homogeneity over the range of measurements. Difference between O3DM and conventional technique (O3DM−conv) plotted against average values of digital and conventional technique (O3DM+conv)/2.
Interexaminer Variation
Regardless of the method the measurements made by examiner 1 displayed significantly lower values than examiner 2 for mandibular arch width but greater for mandibular arch circumference (Table 4). In Table 4 it is shown that examiner 1 had significantly greater values for overbite, and there was also a tendency for lower values of rotations with the O3DM method as compared to examiner 2. Both angular and linear variables showed poor 95% limits of agreement that is shown in Table 4.
Discussion
This study contributes to our knowledge about benefits and drawbacks of using 3D digital technique for assessment of tooth irregularity and dental arch changes. The O3DM 1.4.00 version was compared to a conventional measuring technique and in general, reproducibility was found to be better for angular variables when assessed with the conventional technique. Furthermore, more extreme values were found among the measurements of rotation of lateral incisors where the 3D technique had been used.
This could be explained by the difficulty in placing landmarks properly on the virtual 3D models when assessing rotation and angulation. Both sides of a measured angle required adjustment into the two-dimensional constructed reference plane, so the virtual third dimension (depth) of the digital model restricted the possible areas for placing landmarks correctly (Figs. 2 and 4).
For linear measurements, the two techniques presented less conformity between examiners. Unlike mandibular arch width, maxillary arch width showed greater intraexaminer variation for both examiners when using the O3DM technique. The less distinct anatomy of the maxillary mesiopalatal cusp tips, compared to the mandibular mesiolingual cusps (Fig. 2) and the “smooth” surfaces of the digital models, probably made the identification of landmarks and the correct placement of markers more difficult (Fig. 2). This phenomenon has been described in earlier studies10,11,15–17,19 and the option to enlarge the measurement areas and flipping the models facilitated this procedure only marginally.
The overbite measurements, on the other hand, expressed larger variability for both examiners with the conventional technique than with the 03DM method. Corresponding results were expected for overjet and irregularity considering the difficulties in replicating these measurements with a caliper on plaster models, due to tooth and arch curvature and lack of reference planes. No significant differences or marked trend of better performance could though be detected for overjet and irregularity with the O3DM program despite an accuracy of 0.025 mm for adjustment of planes and markers. Standard deviation and coefficient of variation recorded for angular measurements were small, considering that the measurements were replicated only once and on a small number of models. Thus, the obtained results must be considered as clinically acceptable for both techniques. Reproducibility was found to be in accordance with earlier studies for linear variables such as arch width,8–10 overjet,11 and overbite15 and the differences found between the conventional and the virtual digital techniques was considered to be of no or minor clinical relevance.8–11,13,15–18
In method comparison studies, high correlation coefficients are used as an indicator of good agreement. However, using the correlation coefficient has been questioned as it measures the degree of linear association between two variables instead of agreement directly related to the measurements. High correlation coefficient values may be obtained even though agreement is clinically poor.20,21 Analysis of agreement was therefore made as estimations of difference of one method compared to the other and assessments of how well the two techniques agreed in a single subject.20,21 Systematic errors were analyzed as intermethod and interexaminer variation.
When measurements with the O3DM technique were performed a tendency to produce lower values for linear variables and higher values for incisor rotation was observed compared to the conventional technique. Lateral incisors showed greater mean difference between the two techniques as compared with the central incisors, which could possibly be due to the fact that only a comparatively small number of lateral incisors were available for measurement. The estimated differences between methods were not homogeneous over the range of measurements. Examiner 1 measured higher values at high means for rotation with the O3DM system compared to the conventional method (Fig. 6), while examiner 2 showed generally lower values at high means for both rotation and angulation with this technique. Interexaminer differences were found for both methods, but the differences were not of such magnitude that the quality of the evaluations of clinical treatment outcome on a group level would be compromised. Our attempt to minimize the variation by using detailed written manuals and by calibration of the investigators may have contributed in a positive way to reduce variability. However, before measurements started, examiner 1 had approximately 6 months experience of the O3DM method and was thus quite familiar with the method while examiner 2 had no previous experience with the method. This could explain the somewhat higher intraexaminer values with examiner 2 when measuring on digital models. It has been shown in a number of papers that the ability to carry out measurement on digital models seems to be related to a “learning curve”.9–11,15,18
The intervals between the 95% limits of agreement were very wide and this indicates that the agreement between the O3DM and conventional methods was poor, both in respect of angular and linear variables. Consequently, these two methods should not be used interchangeably in the clinic for measurements on an individual basis.
The digital technique offers great opportunities to register reproducible reference points to be used in orthodontic treatment planning, but still there are difficulties on how to identify the reference points accurately.
The determination of reference planes and points in combination with the recording of a considerable number of variables on each set of models, made the measuring procedure time-consuming. The measuring of one set of models took at least 45 min with the conventional technique and seldom less then 60 min with the 3D technique. Thus, there is need for a more user-friendly technique to be developed if the 3D technique will be the method of choice for routine treatment planning. However, there are improvements made in the latest version from the O3DM company (version 2.2) where an option of placing both sides of an angle in a fixed constructed plane, which should make angular measurements easier, faster, and probably more accurate than the technique used in this study. Changes in the x, y, z coordinates are used to register differences in superimposed digital models. In the near future this can hopefully be used for development of a user-friendly tool for registration of orthodontic parameters such as rotation.
Conclusions
In summary, the conventional method showed better reproducibility for angular variables. The differences between the two methods in reproducibility of linear variables did not show any clear pattern except for overbite, which showed less variability when measured with the 03DM system. Reproducibility was considered clinically acceptable for both methods. Systematic errors indicated that the two methods should not be used interchangeably.
References
Dahlberg G: Statistical Methods for Medical and Biological Students. London: George Allen & Unwin Ltd, 1940, pp 122–132
Edwards JG: A long-term prospective evaluation of the circumferential supracrestal fiberotomy in alleviating orthodontic relapse. Am J Orthod Dentofacial Orthop 93:380–387, 1988
Reitan K: Tissue rearrangement during the retention of orthodontically rotated teeth. Angle Orthod 29:105–113, 1959
Surbeck B, Årtun J: Associations between initial, posttreatment and postretention alignment of maxillary anterior teeth. Am J Orthod 113(2):186–195, 1998
Little RM: The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod 68:554–563, 1975
Naraghi S, Andren A, Kjellberg H, Mohlin BO: Relapse tendency after orthodontic correction of upper front teeth retained with a bonded retainer. Angle Orthod 76:570–576, 2006
Little RM, Riedel RA, Artun J: An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop 93:423–428, 1988
Gracco A, Buranello M, Cozzani M, Siciliani G: Digital and plaster models: a comparison of measurements and times. Prog Orthod 8:252–259, 2007
Quimby ML, Vig KW, Rashid RG, Firestone AR: The accuracy and reliability of measurements made on computer-based digital models. Angle Orthod 74:298–303, 2004
Zilberman O, Huggare JA, Parikakis KA: Evaluation of the validity of tooth size and arch width measurements using conventional and three-dimensional virtual orthodontic models. Angle Orthod 73:301–306, 2003
Asquith J, Gillgrass T, Mossey P: Three-dimensional imaging of orthodontic models: a pilot study. Eur J Orthod 29:517–522, 2007
Hildebrand JC, Palomo JM, Palomo L, Sivik M, Hans M: Evaluation of a software program for applying the American Board of Orthodontics objective grading system to digital casts. Am J Orthod Dentofacial Orthop 133:283–289, 2008
Mok CW, Zhou L, McGrath C, Hagg U, Bendeus M: Digital images as an alternative to orthodontic casts in assessing malocclusion and orthodontic treatment need. Acta Odontol Scand 65:362–368, 2007
Okunami TR, Kusnoto B, BeGole E, Evans CA, Sadowsky C, Fadavi S: Assessing the American Board of Orthodontics objective grading system: digital vs plaster dental casts. Am J Orthod Dentofacial Orthop 131:51–56, 2007
Stevens DR, Flores-Mir C, Nebbe B, Raboud DW, Heo G, Major PW: Validity, reliability, and reproducibility of plaster vs digital study models: comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am J Orthod Dentofacial Orthop 129:794–803, 2006
Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S: Evaluation of the accuracy of digital model analysis for the American Board of Orthodontics objective grading system for dental casts. Am J Orthod Dentofacial Orthop 128:624–629, 2005
Mullen SR, Martin CA, Ngan P, Gladwin M: Accuracy of space analysis with emodels and plaster models. Am J Orthod Dentofacial Orthop 132:346–352, 2007
Santoro M, Galkin S, Teredesai M, Nicolay OF, Cangialosi TJ: Comparison of measurements made on digital and plaster models. Am J Orthod Dentofacial Orthop 124:101–105, 2003
Tomassetti JJ, Taloumis LJ, Denny JM, Fischer Jr., JR: A comparison of 3 computerized Bolton tooth-size analyses with a commonly used method. Angle Orthod 71:351–357, 2001
Bland M: An Introduction to Medical Statistics, Oxford: Oxford University Press, 1991
Altman DG: Practical Statistics for Medical Research, UK: Chapman & Hall/CRC, 1999
Acknowledgements
We would like to thank Christian Melsen, O3DM, Aarhus, Denmark and Bengt Schmeling, Ilexis AB, Linköping, Sweden for technical advice, statistical consultant Anders Magnuson, Örebro University Hospital for statistical expertise and Dr. Björn Svensson, Department of Oral Radiology, Postgraduate Dental Education Center, Örebro, Sweden for fruitful discussions and manuscript work.
Fundings
This study was supported by grants from the Research Committee of Folktandvården, Örebro County Council, Örebro, Sweden. No commercial/financial relationship, interest, or association that might pose a conflict of interest in connection with the article has been present.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sjögren, A.P.G., Lindgren, J.E. & Huggare, J.Å.V. Orthodontic Study Cast Analysis—Reproducibility of Recordings and Agreement Between Conventional and 3D Virtual Measurements. J Digit Imaging 23, 482–492 (2010). https://doi.org/10.1007/s10278-009-9211-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10278-009-9211-y