
Abstract
The purpose of this study was to clarify the stability of masticatory movement after placement of implant-supported denture. Fourteen patients (patient group) with mandibular implants denture and maxillary complete denture and 30 dentate adults (control group) were asked to chew a boiled fishpaste, and the masticatory movement was recorded using MKG. For the 10 cycles beginning with the 5th cycle of mastication, the parameters representing the stability of masticatory movement were calculated. Data collected at 1, 3, 6, 9 months and 1, 2, 3 years after insertion of implants denture were compared between sessions and also between the patient and control groups. The mean and standard deviation of the values in the patient group at 1 month after insertion of implants denture were large, but gradually decreased 6 to 9 months after insertion of implants denture. Each parameter maintained almost the same value from 1 to 3 years. The parameter values of the patient group were significantly larger than those of control group from 1 to 9 months after insertion of implants denture, but 1 year after insertion of implants denture, there was no significant difference between the two groups in 5 out of 7 parameters. From these results, it was suggested that a certain duration, about 9 months to 1 year, was necessary for patients with implants denture to adapt to the new masticatory function and that the timing of functional evaluation should be set to 1 year after insertion of implants denture.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With the improvement in the national consciousness on health and quality of life in recent decades, high-quality medical care based on objective evidence of therapeutic effects is being sought. Under these circumstances, the need for an objective evaluation of masticatory function has been emphasized more than ever before, because the main purpose of dental treatment is to restore and maintain masticatory function.
To objectively evaluate masticatory function, analyses of the masticatory movement, muscular activity, occlusal force, masticatory performance have been conducted. Progress in electronic technologies has enabled quantitative analyses of the movement path and rhythm during mastication. In particular, there have been reports documenting that individual cycles of the mandibular incisal point movement during mastication are regular and stable in healthy dentate adults, whereas they are irregular and unstable in subjects with malocclusion and temporomandibular disorder (TMD) [1,2,3,4]; furthermore, improvement of the irregularity and instability in the latter has been reported in response to treatment [1, 3]. Thus, quantitative analysis of the stability of masticatory movement has been demonstrated to enable objective evaluation of masticatory function. A rhythmic pattern of mastication is maintained under the control of the brainstem pattern generator [5], whereby masticatory movement is modulated via feedback signals from peripheral organs such as the teeth, masticatory muscles and temporomandibular joints [6,7,8], which allow regular and stable masticatory movements in healthy dentate adults [9]. It remains to be clarified whether patients who do not have periodontal ligament receptors and have undergone dental implant treatment would also be capable of performing regular, rhythmic masticatory movements as healthy dentate adults.
It has been reported that masticatory function is reduced due to tooth loss and is improved by prosthetic treatment [10,11,12]. Regarding masticatory movements, prosthetic treatment has been reported to increase the amount of movement during mastication and shorten the cycle time [13,14,15,16], but there is also a report stating that there is no significant change [17,18,19,20]. One of the causes of this discrepancy is the timing of the evaluation of masticatory function. This is because it takes a certain duration to adapt to the new oral environment after insertion of new denture, and the functional evaluation should be performed after the patient adapts to the new denture [21, 22].
Therefore, to clarify the changes and the time taken for the restoration of masticatory function in patients with implants denture, the stability of the movement path and rhythm during mastication was investigated after insertion of new implants denture. The examination of the changes and the time taken to achieve stability of masticatory movement is clinically significant because it would help clarify the appropriate time for functional evaluation for patients with implants denture.
Materials and methods
Ethic statement
This study was approved by the Ethics Committee of the Nippon Dental University School of Life Dentistry (NDU-T2010-20). Prior to participation in the study, informed consent was obtained from the subjects after explaining the purpose of the study to them.
Subjects
Fourteen patients (patient group: 7 males and 7 females; average 75.8 years old) with mandibular implants denture and maxillary complete denture and 30 dentate adults (control group: 15 males and 15 females; 23–49 years old; average 33.2 years old) participated in this study. The inclusion criteria of patient group were as follows: (1) complete edentulousness; (2) indication for a mandible implants denture; (3) sufficient amount of alveolar bone in the anterior region of the mandible; (4) good general health or adequately controlled systemic disease; and (5) satisfactory cognitive function. The exclusion criteria were: (1) clinical abnormalities in the masticatory system; (2) signs or symptoms of TMD and/or orofacial pain. The inclusion criteria of control group were as follows: (1) no clinical abnormalities in the masticatory system; (2) natural dentition, with the possible exception of the third molars; and (3) no complaints related to occlusion. The exclusion criteria of control group were: (1) previous/current orthodontic treatments; (2) currently undergoing dental treatment; and (3) signs or symptoms of TMD and/or orofacial pain. The dentures were adjusted at 2-week intervals up to 2 months after insertion of implants denture. Thereafter, adjustments were made as needed. If the denture was adjusted at the regular inspection, an interval of one week before recording was set.
Test food
The test food used in this study was one cubic centimeter-sized boiled fishpaste (Kibun foods inc., Japan). Boiled fishpaste was used as a test food because it has no adhesiveness and has few fluctuations during chewing [23].
Recording method
Before the experiment, the subjects were allowed to chew boiled fishpaste freely. They were then asked which side it was easier to chew to identify the habitual chewing side. Subjects were asked to chew boiled fishpaste on their habitual chewing side from the beginning of chewing until swallowing, and the movement of the mandibular incisor point was recorded using MKG K6-I. For the ten cycles beginning with the fifth cycle of mastication, the parameters representing the stability of masticatory movement path and rhythm were calculated [9]. Data were collected at 7 sessions of 1, 3, 6, 9 months and 1, 2, 3 years after insertion of implants denture.
Stability of masticatory movement path
Based on the opening and closing paths, consists of vertical and lateral components of mandibular movement for 10 cycles from the 5th cycle, the average path was calculated (Fig. 1A–D). The average of the 11 standard deviations (SD) from level 0 to the 10th level in the horizontal direction during the opening movement, in the horizontal direction during the closing movement, and in the vertical direction were calculated as the opening lateral component, closing lateral component and vertical component, respectively. These three values were then divided by the opening distance (OD), and the value (SD/OD) was used as the parameter representing the stability of masticatory movement path (Fig. 1E).

Method used to calculate average path. A Ten cycles from the 5th cycle after the start of mastication. B The masticatory path was divided vertically into ten equally spaced sections from the intercuspal position (XA, YA) to the open position (XB, YB), and the crossing position of the path at each level (X, Y) was calculated from two points before and after ((X1, Y1) and (X2, Y2)) (example of the fifth cycle). C Coordinates for each cycle were determined by vertically division into ten equally spaced sections. D Average path and standard deviation (SD) of each level. The opening distance (OD) was defined as the vertical distance from the intercuspal position (IP) to the open position. E Numerical data of the average path. F Overlapping of each cycle and average path (○)
Stability of masticatory movement rhythm
For 10 cycles from the 5th cycle, the opening time, closing time, occluding time and cycle time were calculated. The coefficient of variation (CV) was then determined from the mean time of the 10 cycles and its standard deviation, and these four values were used as the parameter representing the stability of masticatory movement rhythm.
Statistical analysis
All data were analyzed using statistical software (SPSS version 27.0, IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to confirm normality. Next, the difference of the parameters representing stability of masticatory movement path and rhythm among the 7 sessions was investigated by ANOVA, and then Bonferroni’s multiple comparison was performed. Furthermore, the data obtained from the patient and control groups in each session were compared using an independent t test. A post hoc power analysis was performed to confirm the validity of the sample size. All statistical analyses were performed with a significance level set at P values of 0.05.
Results
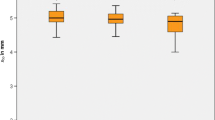
The mean and standard deviation values in the patient group at 1 month after insertion of implants denture were large, but both mean and standard deviation gradually decreased from 6 to 9 months after insertion of implants denture. Each parameter value was maintained at almost the same value from 1 to 3 years (Table 1). In the comparison between the patient group and the control group, the values in the patient group were significantly larger than in the control group from 1 to 9 months after insertion of implants denture (Table 2), but 1 year after insertion of implants denture, there was no significant difference between the two groups in 5 out of 7 parameters (Table 3). As a result of power analysis of the cycle time, the power of 7 sessions was 0.888–1.000, confirming the validity of the sample size.
Discussion
Prosthetic treatments, such as removable dentures and implants denture, are performed for the management of tooth loss, but the timing of functional evaluation after wearing these dentures has not been investigated thoroughly. It is said that sufficient adjustment is required to obtain good masticatory function after insertion of new denture, and functional evaluation should be performed after adapting to the denture [21, 22]. In addition, it has been reported that the masticatory performance of patients with complete dentures significantly improved 3 months after insertion of new dentures [12]. From these reports, Kuramochi et al. [16] set the timing of functional evaluation to 3 months insertion of new complete dentures and investigated the masticatory movement before and after insertion of new complete dentures. The results showed that the amount of opening and masticatory width were significantly large, and the cycle time was significantly less after the treatment. On the other hand, the evaluation timing of masticatory function for implants denture wearers varies from several weeks to 10 years [13, 15, 17,18,19,20, 24, 25], and results with [13,14,15,16] and without [17,18,19,20] significant improvement have been reported. With regard to the changes in the masticatory function over time, after insertion of new denture in patients wearing implant-supported dentures, Vieira et al. [24] examined the masticatory performance before, at 20 days, and at 8 months after insertion of implants denture for 14 edentulous patients, and found that the masticatory performance had improved in some patients but not in others at 20 days, whereas significant improvement was noted at 8 months after the insertion. It has also been reported that masticatory movement is not significantly improved 6 months after insertion of implants denture [18]. These reports indicate that it takes time for patients to adapt to changes in the oral environment and acquire a new masticatory function after insertion of implants denture.
To the best our knowledge, there are no studies investigating changes in the stability of masticatory movements over time after insertion of implants denture. In the present study investigating to the stability of the masticatory movement path and rhythm after insertion of implants denture, large means with large standard deviations were obtained for the parameters assessed at 1 month after insertion of implants denture; the means and standard deviations gradually decreased by 6 to 9 months after, essentially plateauing thereafter. These results appear to imply that the masticatory movement is unstable and there is a large individual difference until 6 to 9 months after insertion of implants denture; however, as the patient acquires new masticatory function by 9 to 12 months, the function is maintained at the acquired levels thereafter. In this study, masticatory performance was not investigated, so it cannot be made a definite statement. However, since it had been reported that there was a positive correlation between stability of masticatory movement and masticatory performance [26], it is easy to speculate that masticatory performance increases as masticatory movement stabilizes. Actually, it was reported that masticatory performance didn’t improve at 20 days, but improved 8 months after insertion of implants denture [24]. The finding of this study also supports the notion that a certain length of time, usually about 9 months to 1 year after insertion of implants denture, is required for the patient to adapt to the newly acquired masticatory function. This supports the report that there was no significant improvement in the masticatory movement at 6 months after insertion of implants denture [18]. Thus, follow-up for at least 9 months, preferably 1 year after implant treatment, is needed for appropriate evaluation of the masticatory function in patients with implants denture.
Trulsson et al. [27] measured the force for holding a peanut between the upper and lower jaw incisors for approximately 3 s, using a strain gauge in dentate subjects (natural teeth) with intact periodontal ligament receptors, a complete denture group with intact oral mucosal receptors, and an implant-supported denture group, and found that the mean hold force was remarkably less in the natural teeth group (0.59 N) as compared to the significantly greater hold force in the complete denture group (2.21 N) and implant-supported denture group (2.63 N), and the standard deviations were also markedly higher in the complete denture group (1.02 N) and implant-supported denture group (1.05 N) than in the natural teeth group (0.23 N). These findings suggest that the loss of the periodontal ligament receptors is not compensated for in the complete denture group and implant-supported denture group. It may be noted that all subjects enrolled in the complete denture and implant-supported denture groups had been wearing dentures for more than 1 year and were satisfied with their dentures. Grigoriadis et al. [28] investigated the masticatory movement and muscular activity during mastication of two kinds of foods with differing hardnesses between subjects with implant-supported bridges in both jaws 1 year earlier and subjects with a set of natural teeth. They described that the subjects with implant-supported bridges showed smaller differences in the degree of vertical movement and a smaller decrease in the muscular activity associated with progressing mastication, and hence resulting in failure to adapt to foods of varying hardness. The results of the present study demonstrated that patients acquired new masticatory movement during the first 9 to 12 months after insertion of implants denture, and although each parameter value representing stability of masticatory movement approached the value of the control group, there were significantly differences on the 2 parameters out of 7 parameters. These results may be due to the inability to compensate for the loss of periodontal ligament receptors in toothless patients with implants denture [27]. It may be said, therefore, that the masticatory function of the patients with implant-supported denture is slightly inferior to that of dentate adults.
Conclusion
To clarify the changes and the time to restoration in the masticatory function over time in patients with implants denture, the parameters representing the stability of the masticatory movement of patients after insertion of implants denture were calculated and compared between sessions. The results suggested that a certain duration, about 9 months to 1 year, to adapt to the newly masticatory function was needed for the patients with implants denture and that the timing of functional evaluation should be set to 1 year after insertion of implants denture.
References
Sato S, Nasu F, Motegi K. Analysis of kinesiograph recordings and masticatory efficiency after treatment of non-reducing disk displacement of the temporomandibular joint. J Oral Rehabil. 2003;30:708–13.
Rilo B, da Silva JL, Mora MJ, Cadarso-Suárez C, Santana U. Unilateral posterior crossbite and mastication. Arch Oral Biol. 2007;52:474–8.
Takeda H, Nakamura Y, Handa H, Ishii H, Hamada Y, Seto K. Examination of masticatory movement and rhythm before and after surgical orthodontics in skeletal class III patients with unilateral posterior cross-bite. J Oral Maxillofac Surg. 2009;67:1844–9.
Piancino MG, Frongia G, Dalessandri D, Bracco P, Ramieri G. Reverse cycle chewing before and after orthodontic-surgical correction in class III patients. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115:328–31.
Lund JP. Mastication and its control by the brain stem. Crit Rev Oral Biol Med. 1991;2:33–64.
Trulsson M, Johansson RS. Encoding of tooth loads by human periodontal afferents and their role in jaw motor control. Prog Neurobiol. 1996;49:267–84.
van der Bilt A, Engelen L, Pereira LJ, van der Glas HW, Abbink JH. Oral physiology and mastication. Physiol Behav. 2006;89:22–7.
Trulsson M. Sensory–motor function of human periodontal mechanoreceptors. J Oral Rehabil. 2006;33:262–73.
Shiga H, Stohler CS, Kobayashi Y. The effect of bolus size on the chewing cycle in humans. Odontology. 2001;89:49–53.
Sun X, Zhai JJ, Liao J, Teng MH, Tian A, Liang X. Masticatory efficiency and oral health-related quality of life with implant-retained mandibular overdentures. Saudi Med J. 2014;35:1195–202.
Ishida K, Nogawa T, Takayama Y, Saito M, Yokoyama A. Does neuroticism influence oral health-related QOL in patients with removable partial dentures? JDR Clin Trans Res. 2017;2:370–5.
Yamamoto S, Shiga H. Masticatory performance and oral health-related quality of life before and after complete denture treatment. J Prosthodont Res. 2018;62:370–4.
Heckmann SM, Heussinger S, Linke JJ, Graef F, Pröschel P. Improvement and long-term stability of neuromuscular adaptation in implant-supported overdentures. Clin Oral Implants Res. 2009;20:1200–5.
Toman M, Toksavul S, Saracoglu A, Cura C, Hatipoglu A. Masticatory performance and mandibular movement patterns of patients with natural dentitions, complete dentures, and implant-supported overdentures. Int J Prosthodont. 2012;25:135–7.
Amaral CFD, Souza GA, Pinheiro MA, Campos CH, Garcia RCMR. Sensorial ability, mastication and nutrition of single-implant overdentures wearers. Braz Dent J. 2019;30:66–72.
Kuramochi A, Shiga H. Effect of denture treatment on masticatory movement in patients with complete dentures. J Prosthodont Res. 2019;63:245–9.
Spitzl C, Pröschel P, Wichmann M, Heckmann S. Long-term neuromuscular status in overdenture and complete denture patients with severe mandibular atrophy. Int J Oral Maxillofac Implants. 2012;27:155–61.
Veyrune JL, Opé S, Nicolas E, Woda A, Hennequin M. Changes in mastication after an immediate loading implantation with complete fixed rehabilitation. Clin Oral Investig. 2013;17:1127–34.
Gonçalves TM, Campos CH, Garcia RCR. Mastication and jaw motion of partially edentulous patients are affected by different implant-based prostheses. J Oral Rehabil. 2014;41:507–14.
Suzuki Y, Kono K, Shimpo H, Sato Y, Ohkubo C. Clinical evaluation of implant-supported removable partial dentures with a stress-breaking attachment. Implant Dent. 2017;26:516–23.
Panek H, Krawczykowska H, Dobosz A, Napadłek P, Panek BA, Sosna-Gramza M. Follow-up visits as a measure of adaptation process to removable prostheses. Gerodontology. 2006;23:87–92.
Eberhard L, Oh K, Eiffler C, Rammelsberg P, Kappel S, Schindler HJ, Giannakopoulos NN. Adaptation to new complete dentures-is the neuromuscular system outcome-oriented or effort-oriented? Clin Oral Investig. 2018;22:2309–17.
Inaba J, Shiga H, Kobayashi Y. Peripheral feedback adjustment in chewing various types of food. J Jpn Prosthodont Soc. 2001;45:271–82.
Vieira RA, Melo AC, Budel LA, Gama JC, de Mattias Sartori IA, Thomé G. Benefits of rehabilitation with implants in masticatory function: is patient perception of change in accordance with the real improvement? J Oral Implantol. 2014;40:263–9.
Meena A, Jain V, Singh N, Arora N, Jha R. Effect of implant-supported prosthesis on the bite force and masticatory efficiency in subjects with shortened dental arches. J Oral Rehabil. 2014;41:87–92.
Uesugi H, Shiga H. Relationship between masticatory performance using a gummy jelly and masticatory movement. J Prosthodont Res. 2017;61:419–25.
Trulsson M, Gunne HS. Food-holding and -biting behavior in human subjects lacking periodontal receptors. J Dent Res. 1998;77:574–82.
Grigoriadis A, Johansson RS, Trulsson M. Adaptability of mastication in people with implant-supported bridges. J Clin Periodontol. 2011;38:395–404.
Funding
The authors received no support from any grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shiga, H., Ogura, S., Hiraga, Y. et al. Stability of masticatory movements after placement of implant-supported denture. Odontology 110, 216–222 (2022). https://doi.org/10.1007/s10266-021-00646-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-021-00646-9