
Abstract
The purpose of this study was to investigate the marginal adaptation and microleakage of SonicFill composite with different photopolymerization techniques. Class II cavities were prepared in 40 premolars and divided into groups according to the photopolymerization technique (n = 10): G1:1200 mW/cm2 for 20 s; G2:1200 mW/cm2 for 40 s; G3:Soft-start with 650 mW/cm2 for 5 s and 1200 mW/cm2 for 15 s; G4:Soft-start with 650 mW/cm2 for 10 s and 1200 mW/cm2 for 30 s. The cavities were restored with OptiBond FL adhesive and SonicFill. Epoxy resin replicas were obtained before and after thermocycling. The occlusal and cervical margins were analyzed with scanning electron microcopy and expressed as the percentage of continuous margins (%CM). The specimens were submitted to microleakage with silver nitrate. ANOVA and Tukey’s test revealed that the %CM at the linguo-occlusal margin for group 1 (83.19%) was significantly different from groups 2, 3 and 4, which had values over 95%. At the cervical margin, there was no statistically significant difference between the groups. After thermocycling, there was a significant decrease in %CM. The predominant score of microleakage was 1 in enamel and 3 in dentin. The SonicFill composite led to gap formation and microleakage, especially in the dentin at the cervical margin, regardless of the photopolymerization technique employed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
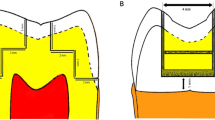
Composite resins designed for a single application, known as “bulk-fill composite resins,” were recently introduced. According to the manufacturer, these materials are suitable for insertion in a 4 or 5 mm bulk placement, depending on the brand, without a prolonged polymerization time. Therefore, bulk-fill composite resins eliminate incremental techniques and reduce the amount of work and number of clinical steps required [1].
The bulk polymerization of these materials is possible due to changes in their chemical composition that reduced polymerization stress [2, 3] and a greater translucency that allows for deeper light penetration and polymerization [4].
One of the bulk-fill composite resins is SonicFill (Kerr), which is inserted into the cavity by sonic activation using a SonicFill handpiece. The material is sculpted and contoured prior to photopolymerization. According to the manufacturer, this sonic activation produces a significant reduction in the viscosity of the composite resin and thus improving the adaptation of the material. The manufacturer of this composite resin also claims that it can be photopolymerized with a thickness of up to 5 mm in 20 s using a high-intensity light-curing unit. However, only one study has confirmed the indication of the manufacturer [5]. In contrast, other studies showed that photopolymerization with this thickness is not appropriate [2, 6–9]. The study by Ilie and Stark [10] suggested a minimum energy density of 47.03 J/cm2 (1176 mW/cm2 for 40 s) to photopolymerize the SonicFill and maintain its mechanical properties, such as flexural strength and microhardness [11], up to a depth of 5 mm.
As an important aspect for the clinical success of restorations, the quality and sealing of the margins depend on many factors, such as the adhesive system used [12] and the magnitude of shrinkage stresses that are generated during the placement and photopolymerization of the composite resin [13]. Clinically, these stresses can be transferred to the restoration margins and thus affect the marginal quality [14]. The adhesive system recommended for SonicFill composite resin is OptiBond FL. OptiBond FL is considered to be the gold standard for three-step etch-and-rinse adhesive systems. This adhesive system presents satisfactory results in bond strength to dental tissues in both in vitro studies and clinical trials [15–17]. Polymerization shrinkage stress depends on many factors, such as the volume of the material, the elastic modulus, and the photopolymerization technique employed [18].
The photoinitiator system for most composites resins is camphorquinone (CQ). A light-curing unit that provides sufficient light intensity for the monomer-polymer conversion is essential for obtaining adequate physical and mechanical properties of the composite resin [19, 20]. The more intense the light source, the more photons are available for absorption by the photosensors. Thus, in the presence of more photons, more CQ molecules are converted to an excited state and react with the tertiary amine to produce free radicals for polymerization [21]. However, a higher light intensity generates higher shrinkage stress in the composite resin [22]. To avoid the generation of high-polymerization shrinkage stress, the use of lower initial intensities with a gradual increase in intensity has been proposed for the photopolymerization of composite resins [23, 24]. The energy irradiated by the light-curing unit is equal to the intensity of the light multiplied by the irradiation time; thus, the amount of energy received by the composite resin can be calculated [25].
Few studies have evaluated the marginal adaptation of SonicFill composite resin; however, available data suggest that this composite resin does not provide better marginal adaptation when compared with conventional composite resins [9, 26]. Moreover, no study has evaluated marginal sealing by microleakage with silver nitrate or marginal adaptation and microleakage with different photopolymerization techniques.
This study evaluated the marginal adaptation and microleakage of class II restorations with SonicFill bulk-fill composite resin using different photopolymerization techniques. Our null hypothesis was that photopolymerization techniques do not influence the marginal adaptation or microleakage of class II cavities restored with the bulk-fill composite resin.
Materials and methods
Forty sound maxillary first premolars were donated by patients treated in the surgery clinic of the Dental School at Pontifical Catholic University of Rio Grande do Sul. An informed consent was signed by all patients after approval from the Ethics Committee (45085015.6.0000.5336). The teeth were cleaned and disinfected in 0.5% chloramine T for 24 h and then stored in distilled water at 4 °C. The buccolingual and mesiodistal dimensions of each tooth were measured with a digital caliper (Mitutoyo, Suzano, SP, Brazil). A maximum variation of 0.5 mm was allowed for each measurement to standardize the dimensions of the teeth.
Each tooth was mounted in a plastic cylinder with self-cured acrylic resin up to 2 mm below the cemento-enamel junction (CEJ) and then stored in distilled water at 4 °C. A single operator performed the MOD cavities with a 2133 diamond bur (KG Sorensen, Barueri, SP, Brazil) for the proximal boxes and a 3131 diamond bur (KG Sorensen, São Paulo, SP, Brazil) for occlusal boxes at high speed with a water coolant. The width between the buccal and lingual cavosurface angles was two-thirds of the distance between the buccal and lingual cusp tips, and the occlusal isthmus was 3 mm deep. The widths of the proximal boxes corresponded to one-third of the distance between the buccal and lingual surfaces of the tooth at the level of the gingival wall and 1.5 mm deep. The distal boxes were located 1 mm coronal to the CEJ, and the mesial boxes were located 1 mm below the CEJ. The internal line angles were rounded, and the cavosurface angles were approximately 90°. The final depth was measured with a periodontal Williams probe (Hu-Friedy, Chicago, IL, USA) as 5 mm in the mesial face and 3 mm in the distal face. The diamond bur was replaced every five preparations.
The Adapt SuperCap matrix system (Kerr Co, Orange, CA, USA) was used to restore the MOD cavities. Low-fusion godiva was placed on the proximal faces to stable the matrix. OptiBond FL (Kerr Co, Orange, CA, USA), a three-step etch-and-rinse adhesive, was applied according to the manufacturer’s instructions. A solution of 37.5% phosphoric acid (Kerr Co, Orange, CA, USA) was applied to the enamel and dentin for 30 s and 15 s, respectively. The teeth were then rinsed with an air/water spray for 15 s. The excess water was removed with cotton swabs. A layer of primer was applied to the dentin for 30 s, followed by gentle air-drying for 5 s. Subsequently, the bond was applied on the enamel and dentin and then light-cured with a Bluephase LED (Ivoclar Vivadent, Liechtenstein) at 650 mW/cm2 for 30 s. The SonicFill composite resin (Kerr Co, Orange, CA, USA), shade A2, was inserted into the preparation with the sonic device, sculpted with a composite spatula, and adapted to the cavosurface angle. Next, the composite resin was photopolymerized with a Bluephase LED with a tip diameter of 9 mm. The light tip was placed close to, but not touching, the surface of the specimen.
The teeth were randomly divided into four groups based on the polymerization technique employed (n = 10):
Group 1—conventional polymerization with an exposure time of 20 s at 1200 mW/cm2, corresponding to an energy density of 24 J/cm2;
Group 2—conventional polymerization with an exposure time of 40 s at 1200 mW/cm2, corresponding to an energy density of 48 J/cm2;
Group 3—soft-start polymerization with an exposure time of 5 s at 650 mW/cm2 and 15 s at 1200 mW/cm2, corresponding to an energy density of 21.25 J/cm2;
Group 4—soft-start polymerization with an exposure time of 10 s at 650 mW/cm2 and 30 s at 1200 mW/cm2, corresponding to an energy density of 42.5 J/cm2.
The restorations were completed using sequential aluminum oxide discs (Sof-Lex Pop-On Polishing discs, 3 M ESPE, St. Paul, MN, USA). A single operator performed all the restoration procedures. The teeth were stored in distilled water at 37 °C for 24 h. Next, impressions of the teeth were made using a polyvinyl siloxane material (3 M ESPE St. Paul, MN, USA), and epoxy resin replicas were obtained (Buehler, Lake Bluff, IL, USA). The specimens were thermocycled in water for 2500 cycles between 5 and 55 °C with a dwell time of 30 s. After thermocycling, a new set of epoxy resin replicas were obtained. Scanning electron microscopy (SEM) (Philips XL 30, Philips Electronic Instruments Inc., Mahwah, NJ, USA) was used to evaluate the occlusal, distal and mesial margins at a magnification of 200×. The values are expressed as a percentage of the continuous margin over the total margin length for the occlusal (buccal and lingual) and cervical (distal and mesial) margins [26]. A blinded evaluator performed the marginal analyses.
The teeth were completely covered with nail varnish, except for the restoration site and the surrounding 0.5 mm margin. The teeth were immersed in a 50% AgNO3 solution for 24 h in a dark room. After washing, the specimens were placed in a developer solution (Kodak, Rochester, NY, USA) and exposed to fluorescent light for 16 h [27]. The teeth were rinsed thoroughly with water and sectioned in the mesiodistal direction at the center of the crowns with a diamond disc mounted on a low speed laboratory cutting machine (Labcut 1010, Extec Corp., London, UK) with cooling. Three sections were obtained from each restoration. The cut surfaces were polished with 1000- and 1200-grit silicon carbide abrasive paper and wetted with water using manual pressure and rotary movements. The extent of dye penetration in the distal cervical margin (enamel) and mesial cervical margin (dentin) was assessed using a stereomicroscope at a magnification of 25× (Olympus Corp., Tokyo, Japan). The section with the greatest microleakage was selected for analysis. Dye penetration was scored using a 4-point scale: 0 = no penetration; 1 = dye penetration to half of the gingival wall; 2 = dye penetration along the gingival wall; 3 = dye penetration along the gingival and axial walls. A blinded evaluator performed the microleakage analyses.
The level of marginal adaptation between groups was analyzed using an ANOVA and Tukey’s test. The marginal adaptation before and after thermocycling was analyzed using a paired Student’s t test. Microleakage data were analyzed using the Kruskal–Wallis and Wilcoxon non-parametric tests. The significance level was set at 5%.
Results
ANOVA followed by Tukey’s post hoc comparisons revealed a significant difference between the photopolymerization techniques. At the bucco-occlusal margin after thermocycling (p ≤ 0.05), Group 1 showed the lowest percentage of continuous margin and was significantly different from group 3. At the linguo-occlusal margin, before and after thermocycling, group 1 showed a significant lower percentage of continuous margin when compared with the other groups (p ≤ 0.05) (Table 1). However, there were no significant differences between the groups in the dentin or enamel at the cervical margin (p ≥ 0.05) (Table 2).
Student’s t test revealed a statistically significant decrease in the mean percentage of continuous margins at the bucco-occlusal margin after thermocycling for groups 1, 2 and 4 (Table 1). There was also a significant decrease in the percentage of continuous margins after thermocycling in the dentin at the cervical margin for groups 1, 3 and 4 and in the enamel at the cervical margin for group 1 (Table 2).
Figure 1 shows an example of a continuous margin, and Fig. 2 shows an example of a non-continuous margin at the occlusal margin observed using SEM.

Representative SEM image (200×) of a continuous margin at the occlusal surface (arrows)

Representative SEM image (200×) of a non-continuous margin at the occlusal surface (arrows)
The Kruskal–Wallis non-parametric test revealed no significant differences in the microleakage scores between groups for the enamel (p = 0.373) and dentin (p = 0.561). Figure 3 shows the microleakage score distribution for each group.

The distribution of microleakage scores for each group
The Wilcoxon non-parametric test revealed significant differences in the microleakage scores between the enamel and dentin for group 1 (p = 0.005), group 2 (p = 0.003), group 3 (p = 0.002) and group 4 (p = 0.004). The microleakage scores in the dentin were significantly higher when compared with the enamel scores. A score of 1 was predominant for the enamel, and a score of 3 was predominant for the dentin. Figure 4 shows representative images of microleakage.

Representative images of microleakage: Images a, b, and c correspond to the dye penetration in the distal cervical margin (enamel): a score 0; b score 1; c score 2. Image d corresponds to the dye penetration in the mesial cervical margin (dentin): score 3
Discussion
This study evaluated the marginal adaptation and microleakage of class II cavities restored with SonicFill bulk-fill composite resin using different photopolymerization techniques. Our null hypothesis for marginal adaptation was rejected because there was a significant difference in the percentage of continuous margins between the photopolymerization techniques for some of the margins evaluated.
The type of photopolymerization employed had a significant influence on the percentage of continuous margins before thermocycling for group 1 at the linguo-occlusal margin. Thus, continuous lower intensity light activation resulted in the lowest percentage of continuous margins. Although the single-session photopolymerization polymerized the composite resin in contact with both the linguo-occlusal and bucco-occlusal margins, there was no significant difference in the percentage of continuous margins at the bucco-occlusal margin before thermocycling.
The occlusal surface of the restoration is the region closest to the light-curing unit and thus has the smallest loss of energy density during curing [28]. However, class II restorations are challenging, particularly when the cervical margins are below the CEJ. Margins below the CEJ make it difficult to achieve efficient results for marginal sealing, polishing and longevity [29]. Thus, the present study also evaluated the microleakage at the cervical margins, including the mesial margin of dentin and the distal margin of enamel.
Although there was no statistically significant difference, conventional polymerization techniques (groups 1 and 2) resulted in a smaller percentage of continuous margins for dentin at the cervical margin before thermocycling when compared with the soft-start polymerization technique (groups 3 and 4). In the soft-start polymerization technique, the initial photopolymerization uses a lower intensity light, which then increases after 5 or 10 s. This technique may be more effective because it prolongs the pre-gel stage to better accommodate the newly formed polymer molecules. Consequently, the composite resin flow is improved and the internal shrinkage stress of the material is relaxed, which decreases the stresses inside the structure and improves marginal integrity [19]. Continuous and fast photopolymerization causes an increase in gap formation [25]. However, at the cervical margin of the enamel, there was a 100% continuous margin in groups 2, 3 and 4 and only a 3% non-continuous margin in group 1. Although the OptiBond FL adhesive system is considered the gold standard of etch-and-rinse adhesive systems [16], a lower percentage of continuous margins for dentin is expected, and the bond strength for enamel is more effective when 37% phosphoric acid etching is used [15]. Therefore, the type of photopolymerization technique employed was an important factor for the percentage of continuous margins for dentin but not enamel. The study by Campos et al. [26] also found lower marginal adaptation at dentin margins when compared with enamel margins.
The present study used the maximum depth of 5 mm for the cavity preparation on the mesial cervical margin. Although the manufacturer recommends further photopolymerization at the cervical margins after removal of the matrix in class II restorations, this procedure was not completed in this study. Similar to other studies, the photopolymerization was completed only at the occlusal surface [9, 26, 30]. The photopolymerization was only performed at the occlusal surface to accurately calculate the energy density for each technique. Regardless of the photopolymerization technique applied, there were non-continuous margins present that were not likely to disappear if an additional photopolymerization had been performed. Nevertheless, an additional photopolymerization at the cervical margins may have resulted in higher percentages of continuous margins after thermocycling and lower microleakage scores.
SonicFill composite resin requires the use of a device that emits sonic vibration. This vibration decreases the viscosity of the composite resin and allows for a better adaptation of the material to the margins of the cavity. After deactivation of the sonic vibration, the viscosity increases to allow for sculpting of the restoration [9, 30]. Thus, SonicFill composite resin is different from conventional composite resins that use the standard 2-mm incremental technique [31]. However, the bulk-fill technique used by SonicFill facilitates and expedites the restoration procedure, but it does not solve the clinical problem of gap formation at the interface due to polymerization shrinkage, particularly at the cervical margin of dentin.
In the present study, the two different energy densities used in each photopolymerization technique did not significantly influence the percentage of continuous margins, except at the linguo-occlusal margin of group 1. According to the study by Bucuta and Ilie [4], the amount of light transmitted through the SonicFill composite resin was lower than the composite resins: x-tra base, Venus Bulk Fill, Filtek Bulk Fill, x-tra fil, and Tetric EvoCeram Bulk Fill. According to these authors, this finding is explained by the fact that SonicFill is not as translucent to blue light due to its high content of inorganic particles (84% by weight, 66% by volume) and the irregular shape of the particles, thus increasing light scattering and decreasing light transmittance [2, 4, 6]. Due to the low translucency of SonicFill, it is necessary to use a higher energy density, approximately 47.03 J/cm2, to obtain the minimum degree of conversion needed for a thickness of 5 mm [10]. The energy density only affected marginal adaptation in the linguo-occlusal margin; however, it is not advisable to use lower energy densities because other parameters are important for the longevity of the restoration, such as hardness and flexural strength. These properties are directly related to the degree of conversion provided by the light-curing unit [7, 8].
The present study used thermocycling to simulate the degradation of the bond interface that occurs over time in the oral cavity. The effectiveness of thermocycling as a clinical aging simulator has been controversial [32, 33]. In addition, no evidence of the number of cycles likely to be experienced in vivo was found, but a provisional estimate of approximately 10,000 cycles per year was suggested [34]. In our study, 2500 cycles were applied to the specimens, and these thermal cycles were effective at decreasing the percentage of continuous margins. This effect was minor at the occlusal margins and more significant at cervical margins, particularly for dentin. However, the hypothesis cannot be ruled out that a higher number of thermal cycles could decrease the percentage of continuous margin at the occlusal margins [34]. The restorations could also have been submitted to mechanical loading test that tries to simulate the masticatory loads applied on the restorations [35]. However, mechanical loading was not performed, being one of the limitations of the present study, since different results could have been obtained if the restorations had received occlusal loads [36].
The cervical margins of dentin, which corresponded to a 5 mm depth, showed less than 50% of continuous margins after thermocycling for all groups. These results support the study by Benetti et al. [9] that found large gaps in dentin margins when a bulk-fill composite resin was used. The difference in continuous margin between the cervical (dentin) and occlusal (enamel) margins may be related to the higher bond strength of the adhesive to etched enamel in comparison with etched dentin [37], contributing to greater resistance to the thermal changes at the enamel margins. Furthermore, due to the cavity geometry, the cervical margin was farther from the curing light that was applied only at the occlusal surface. As a result, it is expected lower conversion degree of the composite resin at the cervical margin in comparison with the occlusal margin that received the curing light directly [38].
In the present study, microleakage was more severe (score 3) at the cervical margins located in dentin than at the cervical margins located in enamel (score 1). The microleakage results are consistent and expected based on the lower percentage of continuous margins for dentin. Similarly, previous studies showed that microleakage tends to be higher in dentin than in enamel [39, 40]. Dentin has higher biological variability than enamel, which makes it a more difficult substrate to obtain a high bond strength with the adhesive that must resist thermal stresses and the interfacial stresses generated by the polymerization shrinkage of the composite resin [41]. The results of our study support the research by Kalmowicz et al. [30], which found that the microleakage in enamel was significantly lower when compared with dentin, regardless of the material, C-factor, or insertion technique. Another possible explanation for less infiltration in enamel when compared with dentin is the use of an etch-and-rinse adhesive system that employs 37% phosphoric acid etching. This etching procedure is more effective at increasing the bond strength for enamel when compared with self-etch adhesive systems [42–44]. None of the photopolymerization techniques used in our study prevented microleakage, and there was no significant difference in the microleakage scores between groups; thus, the null hypothesis was rejected.
The results of laboratory studies should be carefully extrapolated to the clinical reality. However, the findings of this study show that obtaining 100% of continuous margins along all margins in a class II cavity is a challenge when using SonicFill composite resin and the OptiBond FL adhesive system. These findings are concerning because the presence of non-continuous margins can increase the occurrence of microleakage and secondary caries, two factors that compromise the longevity of restorations [45]. Although the present study did not compare the bulk-fill composite resin with a traditional composite resin, other in vitro studies have shown that bulk-fill materials do not allow better marginal adaptation than standard composite [26, 44, 46,47,48]. Besides that, clinical trials showed that bulk-fill composite resin had similar clinical performance when compared to the conventional 2 mm layering technique in posterior composite resin restorations [49–51].
Despite the limitations of this in vitro study, it can be concluded that the bulk-fill technique with SonicFill composite resin and the OptiBond FL adhesive system for class II cavities resulted in non-continuous margins and microleakage, especially in the dentin at the cervical margin, regardless of the photopolymerization technique employed. In addition, the soft-start technique resulted in a higher percentage of continuous margins for dentin at the cervical margin. However, there was a loss of continuous margins after thermocycling, regardless of the photopolymerization technique employed.
References
Walter R. Critical appraisal: bulk-fill flowable composite resins. J Esthet Restor Dent. 2013;25:72–6.
Garcia D, Yaman P, Dennison J, Neiva G. Polymerization shrinkage and depth of cure of bulk fill flowable composite resins. Oper Dent. 2014;39:441–8.
Al Sunbulh H, Silikas N, Watts DC. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composite. Dent Mater. 2016;32:998–1006.
Bucutas S, Ilie N. Light transmittance and micro-mechanical properties of bulk fill vs. conventional resin based composites. Clin Oral Investig. 2014;18:1991–2000.
Alrahlah A, Silikas N, Watts DC. Post-cure depth of cure of bulk fill dental resin-composites. Dent Mater. 2014;30:149–54.
Garoushi S, Säilynoja E, Vallittu PK, Lassila L. Physical properties and depth of cure of a new short fiber reinforced composite. Dent Mater. 2013;29:835–41.
Goracci C, Cadenaro M, Fontanive L, Giangrosso G, Juloski J, Vichi A, Ferrari M. Polymerization efficiency and flexural strength of low-stress restorative composites. Dent Mater. 2014;30:688–94.
Tarle Z, Attin T, Marovic D, Andermatt L, Ristic M, Tauböck TT. Influence of irradiation time on subsurface degree of conversion and microhardness of high-viscosity bulk-fill resin composites. Clin Oral Investig. 2014;19:831–40.
Benetti AR, Havndrup-Pedersen C, Honoré D, Pedersen MK, Pallesen U. Bulk-fill resin composites: polymerization contraction, depth of cure, and gap formation. Oper Dent. 2015;40:190–200.
Ilie N, Stark K. Curing behaviour of high-viscosity bulk-fill composites. J Dent. 2014;42:977–85.
Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013;38:618–25.
Geerts S, Bolette A, Seidel L, Guéders A. An in vitro evaluation of leakage of two etch and rinse and two self-etch adhesives after thermocycling. Int J Dent. 2012;12:1–7.
Gregor L, Bortolotto T, Feilzer AJ, Krejci I. Shrinkage kenetics of a methacrylate- and a silorane-based resin composite: effect on marginal integrity. J Adhes Dent. 2013;15:245–50.
Braga RR, Hilton TJ, Ferracane JL. Contraction stress of flowable composite materials and their efficacy as stress-relieving layers. J Am Dent Assoc. 2003;134:721–8.
Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, Vijay P, Van Landuyt K, Lambrechts P, Vanherle G. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent. 2003; 28:215–35.
Sarr M, Kane AW, Vreven J, Mine A, Van Landuyt KL, Peumans M, Lambrechts P, Van Meerbeek B, De Munck J. Microtensile bond strength and interfacial characterization of 11 contemporary adhesives bonded to bur-cut dentin. Oper Dent. 2010;35:94–104.
de Paula EA, Tay LY, Kose C, Mena-Serrano A, Reis A, Perdigão J, Loguercio AD. Randomized clinical trial of four adhesion strategies in cervical lesions: 12-month results. Int J Esthet Dent. 2015;10:122–45.
Ilie N, Hickel R. Resin composite restorative materials. Aust Dent J. 2011;56:59–66.
Rueggeberg F. Contemporary issues in photocuring. Compend Contin Educ Dent Suppl. 1999;25:S4–15.
Kwon TY, Bagheri R, Kim YK, Kim KH, Burrow MF. Cure mechanisms in materials for use in esthetic dentistry. J Investig Clin Dent. 2012;3:3–16.
Vandewalle KS, Ferracane JL, Hilton TJ, Erickson RL, Sakaguchi RL. Effect of energy density on properties and marginal integrity of posterior resin composite restorations. Dent Mater. 2004;20:96–106.
Lim BS, Ferracane JL, Sakaguchi RL, Condon JR. Reduction of polymerization contraction stress for dental composites by two-step light-activation. Dent Mater. 2002;18:436–44.
Charton C, Colon P, Pla F. Shrinkage stress in light-cured composite resins: influence of material and photoactivation mode. Dent Mater. 2007;23:911–20.
Oliveira KM, Lancellotti AC, Ccahuana-Vásquez RA, Consani S. Shrinkage stress and degree of conversion of a dental composite submitted to different photoactivation protocols. Acta Odontol Latinoam. 2012; 25:115–22.
Asmussen E, Peutzfeldt A. Polymerization contraction of resin composite vs. energy and power density of light-cure. Eur J Oral Sci. 2005;113:417–21.
Campos EA, Ardu S, Lefever D, Jassé FF, Bortolotto T, Krejci I. Marginal adaptation of class II cavities restored with bulk-fill composites. J Dent. 2014;42:575–81.
Tay FR, Hashimoto M, Pashley DH, Peters MC, Lai SC, Yiu CK, Cheong C. Aging affects two modes of nanoleakage expression in bonded dentin. J Dent Res. 2003;82:537–41.
Bennett AW, Watts DC. Performance of two blue light-emitting-diode dental light curing units with distance and irradiation-time. Dent Mater. 2004;20:72–9.
Krämer N, Reinelt C, Frankenberger R. Ten-year clinical performance of posterior resin composite restorations. J Adhes Dent. 2015;17:433–41.
Kalmowicz J, Phebus JG, Owens BM, Johnson WW, King GT. Microleakage of class I and II composite resin restorations using a sonic-resin placement system. Oper Dent. 2015;40:653–61.
Sakaguchi RL, Douglas WH, Peters MC. Curing light performance and polymerization of composite restorative materials. J Dent. 1992;20:183–8.
Doerr CL, Hilton TJ, Hermesch CB. Effect of thermocycling on the microleakage of conventional and resin-modified glass ionomers. Am J Dent. 1996;9:19–21.
Yap AU. Effects of storage, thermal and load cycling on a new reinforced glass-ionomer cement. J Oral Rehabil. 1998;25:40–4.
Gale MS, Darvell BW. Thermal cycling procedures for laboratory testing of dental restorations. J Dent. 1999;27:89–99.
Amaral FLB, Colucci V, Palma-Dibb RG, Corona SAM. Assessment of in vitro methods used to promote adhesive interface degradation: a critical review. J Esthet Restor Dent. 2007;19:340–53.
Aggarwal V, Logani A, Jain V, Shah N. Effect of cyclic loading on marginal adaptation and bond strength in direct vs. indirect class II MO composite restorations. Oper Dent. 2008;33:587–92.
Juloski J, Goracci C, Rengo C, Giovannetti A, Vichi A, Vulicevic ZR, Ferrri M. Enamel and dentin bond strength of new simplified adhesive materials with and without preliminary phosphoric acid-etching. Am J Dent. 2012;25:239–43.
Catelan A, De Araújo LS, Da Silveira BC, Kawano Y, Ambrosano GM, Marchi GM, Aguiar FH. Impact of the distance of light curing on the degree of conversion and microhardness of a composite resin. Acta Odontol Scand. 2015;73:298–301.
Hasanreĭsoğlu U, Sönmez H, Uçtaşli S, Wilson HJ. Microleakage of direct and indirect inlay/onlay systems. J Oral Rehabil. 1996;23:66–71.
Gerdolle DA, Mortier E, Loos-Ayav C, Jacquot B, Panighi MM. In vitro evaluation of microleakage of indirect composite inlays cemented with four luting agents. J Prosthet Dent. 2005;93:563–70.
Manhart J, Schmidt M, Chen HY, Kunzelmann KH, Hickel R. Marginal quality of tooth-colored restorations in class II cavities after artificial aging. Oper Dent. 2001;26:357–66.
Hannig M, Reinhardt KJ, Bott B. Self-etching primer vs phosphoric acid: an alternative concept for composite-to-enamel bonding. Oper Dent. 1999;24:172–80.
Pashley DH, Tay FR. Aggressiveness of contemporary self-etching adhesives. Part II: etching effects on unground enamel. Dent Mater. 2001;17:430–44.
Al-Harbi F, Kaisarly D, Michna A, ArRejaie A, Bader D, El Gezawi M. Cervical interfacial bonding effectiveness of class II bulk versus incremental fill resin composite restorations. Oper Dent. 2015;40:622–35.
Nedeljkovic I, Teughels W, De Munck J, Van Meerbeek B, Van Landuyt KL. Is secondary caries with composites a material-based problem? Dent Mater. 2015;31:e247–77.
Agarwal RS, Hiremath H, Agarwal J, Garg A. Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: an in vitro study. J Conserv Dent. 2015;18:56–61.
Heintze SD, Monreal D, Peschke A. Marginal quality of class II composite restorations placed in bulk compared to an incremental technique: evaluation with SEM and stereomicroscope. J Adhes Dent. 2015;17:147–54.
de Assis FS, Lima SN, Tonetto MR, Bhandi SH, Pinto SC, Malaquias P, Loguercio AD, Bandéca MC. Evaluation of bond strength, marginal integrity, and fracture strength of bulk- vs incrementally-filled restorations. J Adhes Dent. 2016;18:317–23.
Van Dijken JW, Pallesen U. A randomized controlled three year evaluation of “bulk-filled” posterior resin restorations based on stress decreasing resin technology. Dent Mater. 2014;30:245–51.
Van Dijken JW, Pallesen U. Posterior bulk-filled resin composite restorations: a 5-year randomized controlled clinical study. J Dent. 2016;51:29–35.
Bayraktar Y, Ercan E, Hamidi MM, Colak H. One-year clinical evaluation of different types of bulk-fill composites. J Investig Clin Dent. 2016;22:1–9.
Acknowledgements
The authors thank the Central Laboratory of Microscopy and Microanalysis of PUCRS for the images of Scanning Electron Microscopy. The present study was carried out with the support of the Program Students-Agreement of Post-Graduation—PEC-PG, CAPES/CNPq, Brazil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Gamarra, V.S.S., Borges, G.A., Júnior, L.H.B. et al. Marginal adaptation and microleakage of a bulk-fill composite resin photopolymerized with different techniques. Odontology 106, 56–63 (2018). https://doi.org/10.1007/s10266-017-0294-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-017-0294-5