
Abstract
Objectives
The present study aimed to provide normative data for the EQ-5D-5L questionnaire in Bulgaria, based on a nationally representative sample.
Methods
Random sampling was used. In September 2018, a total of 1005 respondents (aged 18–89 years) completed the self-administered paper-based EQ-5D-5L questionnaire, including a visual analogue scale (EQ VAS). Health state utility index scores were derived using the directly measured Polish value set.
Results
The study sample was representative of the general Bulgarian population in terms of age, sex, geographical region, educational level, social and professional status. Mean EQ-5D-5L and EQ VAS values decreased from 0.986 and 89.7 (age group 18–24 years) to 0.789 and 53.6 (age group ≥ 75 years), respectively. Perfect health (the “11,111” health state) was reported by half of the population (50.1%), more often by men than women (55.8% vs 44.9%). The most frequently reported complaints characterised pain/discomfort dimension (39.1%), followed by anxiety/depression (34.5%). Although the least commonly reported health limitations concerned the self-care dimension, their frequency (13.6%) was the highest among the seventeen identified EQ-5D-5L population norm studies. The mean severity index score for the whole study sample was 6.96. EQ-5D-5L index was higher in respondents from lower age groups and with a higher average income per household member.
Conclusions
Bulgarian population norms, which were developed for the descriptive part of the EQ-5D-5L and EQ VAS, can be used as reference values. The availability of such normative data should encourage the use of the EQ-5D-5L questionnaire in health-related quality-of-life studies in Bulgaria.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Medical advances in the past century have saved millions of lives, but the psychosocial well-being of patients has been of secondary importance during this time of technological progress. However, a recent resurgence of interest in caring for the mental state of patients is evident in guidelines published by organisations such as the American Medical Association (AMA) or the American College of Physicians (ACP) [1]. This recognition of 'whole-person' care is not limited to the United States. The World Health Organization (WHO) advises clinicians to measure the quality of life (QoL) of patients within six domains: physical health, psychological health, level of independence, social relations, environmental factors, and spirituality [2].
Measuring health-related quality of life (HRQoL) provides a focused assessment of the QoL by investigating the effects of a disease and its treatment on both medical and nonmedical aspects of the patient's life [3]. Increasing utilisation of HRQoL instruments is observed in patients and general population surveys. Although disease-specific measures are essential for more detailed QoL measurement, generic ones can be used across all diseases, conditions, different medical interventions and a wide range of populations [3,4,5]. Results obtained using a generic questionnaire provide an opportunity to make comparisons regarding average health status between age-matched and sex-matched population samples [6].
The EQ-5D instrument is the most widely used preference-based HRQoL questionnaire in cost-effectiveness analyses. The National Institute for Health and Care Excellence (NICE) in the United Kingdom and health technology assessment (HTA) agencies from Colombia, Czech Republic, France, The Netherlands, New Zealand, Poland, and Thailand recommend the use of EQ-5D in pharmacoeconomic analyses included in reimbursement dossiers. This partly explains the spreading use of the instrument in contemporary studies [7, 8].
The original EQ-5D questionnaire (EQ-5D-3L) has five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) and three distinct levels of functioning within each aspect (no problems, some problems and extreme problems) [9]. Extensive research supported the use of the instrument in many disease areas, but there was concern in the early 2000s over ceiling effect issues, particularly in general population samples [10, 11]. In response to this, the EuroQol Group proposed a new version of the instrument: the EQ-5D-5L. In the updated tool, the number of severity levels increased from three to five, thus improving the instrument's sensitivity and reducing the ceiling effects [12, 13].
Normative data tables from surveys of randomly selected subjects from the general population, provide a useful guide for interpretation of QoL results from other studies. Norms can comprise values for the general population or various subgroups, such as healthy people or patients with specific disease conditions [14].
EQ-5D-5L population norms have been developed for numerous countries and regions: Germany [15,16,17], Hong-Kong [18], Indonesia [19], Ireland [20], Japan [21], Poland [22], South Korea [23], Spain [24, 25], Trinidad and Tobago [26], United States [27], Uruguay [28], Vietnam [29], the Athens metropolitan area [30], the urban population of China [31], South Australia [32] and Quebec [33]. These norms are successfully used in pharmacoeconomic analyses and other patient-reported outcome-based studies.
The main limitation against the broader application of the EQ-5D in clinical and pharmacoeconomic studies in Bulgaria is the lack of both population norms and a national EQ-5D value set. The present study aimed to provide normative data for the EQ-5D-5L questionnaire in Bulgaria, based on a survey among a nationally representative sample.
Methods
Sample and interview procedure
Sample recruitment and interviewing was carried out by a market research company (MarketLinks) in September 2018. The study was run as a part of an omnibus survey—multiple research clients provided content for the survey but shared the common demographic data collected from each respondent. The sampling design included a two-stage cluster sample (the first stage was the region and the second the type of locality—capital city, large city, smaller city or town/village). For representativeness of the sample, quota by age and gender were used within each area. Approximately 1030 households were contacted, to obtain the target sample of about 1000 respondents. The sample was intended to be representative of the general adult Bulgarian population, at least concerning age, sex, level of education and place of residence according to the National Statistical Institute data (www.nsi.bg). Each respondent was asked to complete the EQ-5D-5L questionnaire (including the descriptive system and the visual analogue scale, EQ VAS) and answer questions about demographic characteristics and socioeconomic status. The official Bulgarian language version of the EQ-5D-5L was used, after receiving formal consent from the EuroQol group. The questionnaire was administered as a paper-and-pencil version. Respondents had to fill it out on their own in the presence of an interviewer. Answers to general questions were collected using the tablet-assisted personal interviewing (TAPI) system.
EQ-5D-5L
The descriptive system comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has five levels: no problems, slight problems, moderate problems, severe problems and extreme problems. The patient is asked to indicate his/her health state by ticking the box next to the most appropriate statement in each of the five dimensions. This decision results in a one-digit number that expresses the level selected for that dimension. The digits for the five dimensions can be combined into a five-digit number that describes the patient's health state, with 11,111 indicating perfect health and 55,555 the worst health state. The system defines 3125 (55) possible health states [34]. Each health state can be transformed into a weighted index score using a specific country-specific value set. As there is no available Bulgarian value set yet, we used the Polish EQ-5D-5L directly measured value set to estimate EQ-5D-5L index values. At the moment of the study, it was the only EQ-5D-5L value set coming from Central and Eastern Europe [35]. EQ-5D index values illustrate societal preferences for different health states and range from –0.590 to 1.0, where negative values correspond to bad health conditions (states worse than death), and 1.0 corresponds to perfect health.
The EQ VAS records the patient's self-rated health on a vertical visual analogue scale, where the endpoints are labelled 'The best health you can imagine' and 'The worst health you can imagine'. The VAS can be used as a quantitative measure of health outcome that reflects the patient's subjective judgement.
To enable objective comparisons of samples between studies (both within a country and internationally), an unweighted measure of health, so-called severity index (or misery index), may also be estimated. This index is calculated by summing the levels for each dimension. The outcome ranges from 5 (no health limitations at all, 11,111) to 25 (for state 55,555).
Socioeconomic status variables
Questions about demographic characteristics and socioeconomic status covered the following areas: age, sex, place of residence, level of education, social and professional status, the number of members of a given household, respondent's income level, ethnicity and religious affiliation.
Analysis
The distribution of answers to the questions in the descriptive part of the EQ-5D-5L was estimated. Results were presented for the whole sample, as well as for the predefined age groups (18–24, 25–34, 35–44, 45–54, 55–64, 65–74, and ≥ 75 years) in the EuroQol Group's standardised format to facilitate comparative research. Unpaired t-test and ANOVA were used to assess differences between two and several demographic groups, respectively, in interval data, such as the EQ-5D index, EQ VAS or the misery index [36]. Multiple linear regression was used to examine the associations of sociodemographic characteristics with the EQ-5D index and EQ VAS scores. We hypothesised that people with higher income, a higher education level and less advanced age would be characterised by having a better quality of life. All variables, including age, were entered into the models as categorical variables. We performed a backward selection procedure to remove covariates with p > 0.05. Regression coefficients with corresponding 95% confidence intervals were presented only for statistically significant variables. The analysis was conducted using the statistical software, StatsDirect 3.1.22 (StatsDirect Ltd, Altrincham, England).
Results
Study population
In September 2018, a total of 1005 interviews with adult Bulgarian citizens were completed. The characteristics of the study group are presented in Table 1. Respondents were aged from 18 to 89 years. The sample was similar to the Bulgarian population in terms of age, sex, geographical region, type of locality, educational level, and social and professional status.
EQ-5D-5L dimensions
Table 2, Supplement Table S1 and Supplement Table S2 present the frequency of problems for particular EQ-5D-5L dimensions in different age groups for all respondents and separately for men and women. The results of the survey showed that people experienced most problems regarding the pain/discomfort (39.1%) and anxiety/depression (34.5%) dimensions, with self-care limitations reported with the least frequency (13.6%).
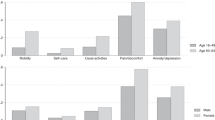
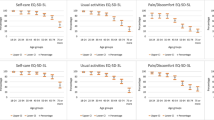
Perfect health (no problems across all five dimensions) was reported by half of the population (50.1%), more often by men than women (55.8% vs 44.9%). The frequency of reported health limitations increased with age, and this trend was observed for almost all dimensions (Fig. 1). In all dimensions, problems were more commonly reported by women than men, with the most significant difference in the anxiety/depression and pain/discomfort domains (40.6% vs 27.8% and 43.8% vs 33.9%, respectively; Supplement Table S1 and Supplement Table S2).

Rating of health limitations (any level of severity) for EQ-5D-5L dimensions in the different age groups
EQ-5D-5L index
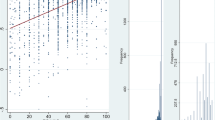
Similar trends were observed for EQ-5D index values (Table 3). EQ-5D-5L index scores significantly decreased with age (p < 0.0001, ANOVA; Fig. 2). In general, women were characterised by a lower index value of 0.935, compared to an index value of 0.950 in men (p = 0.04; unpaired t-test). The histogram for EQ-5D-5L index values is presented in Supplement Fig. S1.

EQ-5D-5L index and EQ VAS (divided by 100) in the various age groups
EQ VAS
The subjective assessment of respondents’ health, based on the EQ VAS for the whole study group and separately for men and women, is presented in Table 4 and Supplement Fig. S2. In general, women reported somewhat poorer health than men (77.1 vs 78.7; NS). Self-rated health, according to the VAS, declined consistently with age. The rate of this decline was similar to that in the EQ-5D-5L index (Fig. 2).
Severity index (an unweighted measure of health)
The results of the severity index by gender and age were consistent with the EQ-5D index results. The mean severity index score for the whole study sample was 6.96 (SE 0.09). Males, in comparison to females, were characterised by having lower values for the misery index, which corresponded to better health profiles (p < 0.01, unpaired t-test; Supplement Table S3).
Results by sociodemographic characteristics
In Table 5, we present the results of multivariate analysis on sociodemographic characteristics, which significantly predicted HRQoL outcomes. Average monthly income per household member over 400 BGN was positively associated with EQ-5D-5L index, whereas being in the group of respondents with more advanced age (over 45 years)—negatively. Sofia city inhabitants were found to have better subjective health status according to EQ VAS, while people from older age groups (over 35 years) characterised with lower EQ VAS scores.
Discussion
We developed Bulgarian population norms for the EQ-5D-5L descriptive system, EQ-5D index and EQ VAS, based on a sample that was highly representative of the entire population. These norms can be used as reference values by physicians, public health specialists, epidemiologists and health economists, as well as health care decision-makers.
The sample size of the present study may be perceived as a major limitation. EQ-5D-5L population norm studies differ significantly in sizes—from about 600 (South Korea, Uruguay) [23, 28] to about 20,000 (Spain) [24, 25]. Samples of a similar size to ours were used in population norm surveys in Hong Kong, Indonesia, Ireland and Japan [18,19,20,21]. The size of the population norm study is always a trade-off between sample representativeness and study sensitivity on the one hand, and the financial burden of carrying it out on the other. We believe that for the Bulgarian setting a sample close to 1000 should be sufficiently representative, as the country’s population is relatively small—about seven million people. When we estimate the number of respondents used in a study per million of inhabitants, it appears that only two studies—from Trinidad and Tobago [26] and from Spain [24, 25]—had more favourable ratios.
The main strength of the present study was the advanced sampling design, which resulted in the sample being representative of the Bulgarian population in terms of gender, age group, geographical region and type of locality. The main differences in the sample characteristics, compared to the general population, concerned a smaller representation of people aged 75 or above and overrepresentation of people with higher education.
As we had no data on the number of persons in the household, we were not able to estimate equivalised income. In consequences, our results may not be entirely accurate as decreasing marginal consumption with increased household size was not taken into account.
Moreover, the use of the Polish EQ-5D-5L value set to estimate the EQ-5D index in the current study may also be seen as a limitation. We made this decision because of the lack of a directly measured Bulgarian value set, and no plans currently exist to develop such a value set in the near future. At the time of the survey, Poland was the only country from the cultural circle of Central and Eastern Europe that had its own value set. We have assumed that, due to similar historical and cultural determinants, the health preferences of Bulgarian society will be closer to the Polish equivalents than those in Western European countries. Of course, this assumption requires scientific verification at some point in the future. It goes without saying that the ideal situation would be the development of a Bulgarian country-specific EQ-5D-5L value set.
Looking at EQ-5D-5L population norm studies, it is evident that societies differ in the context of health and its perception. The percentage of citizens stating 'no problems' within EQ-5D-5L dimensions (health state ‘11,111’) varies from 21% in Quebec (Canada) [33] to 72% in Trinidad and Tobago [26]. The proportion for Bulgaria (50%) lies in the middle, between the median and third quartile for 17 of the population norms we have identified [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33].
Further analysis, focused on individual EQ-5D-5L dimensions and the percentage of citizens reporting 'any problems' within a dimension, brings a less optimistic picture of the situation in Bulgaria. The society is characterised by the highest percentage of health limitations within the self-care domain (13.6%), and the second-highest with regards to mobility (27.2%), among all the identified norms studies. The ratings for the dimensions of usual activities and anxiety/depression both correspond to the third quartile in this ranking. Only the rating for the pain/discomfort dimension (39.2%) lies below the median. Looking at Poland, the only other country from Central and Eastern Europe in this list, we can see quite similar results, with slightly lower limitations within 'physical' dimensions (mobility, self-care, usual activities) and higher within 'mental' dimensions [22]. The only substantial difference is seen in the feeling of pain/discomfort, where Bulgarian society has significantly fewer problems than its Polish counterpart.
Subjective perception of health, measured with EQ VAS, also varies between societies. The highest rating can be observed in Asian countries (Vietnam and China) [29, 31]; the lowest in developed countries—Germany, Poland, Spain and Canada (Quebec) [17, 22, 24, 33]. EQ VAS outcomes place Bulgaria low on the scale—just ahead of the developed countries mentioned above.
Factors that improved perception of HRQoL in our study independently included higher income, living in Sofia (the capital of Bulgaria) and younger age. Two of these factors are well described as influential in the literature, income in Ireland, Japan and Vietnam [20, 21, 29], among others, and age in Australia, Germany and Japan [16, 21, 32]. A highly cited factor—education level (Australia, Germany, Hong Kong, Ireland, Japan) [16, 18, 20, 21, 32] was not significant in the Bulgarian data. Our third most significant factor, living in the capital, is not so straightforward, even though it might appear so at first glance. For instance, in Ireland, living in an urban area has a negative influence on the quality of life [20]. Other factors that are not so straightforward include sex and retirement status. Being male is associated with the perception of a lower quality of life in China and Ireland [20, 31] but a higher one in Germany [16]. Moreover, being retired negatively influences HRQoL in China and Vietnam [29, 31] but has a positive effect in Australia [32].
Our study is the first general Bulgarian population study using the EQ-5D questionnaire. In 2016, Vankova et al. published the results of a local population survey from the city of Burgas (a major city in south-east Bulgaria with over 400,000 inhabitants) [37]. Both studies had similar sizes (about 1000 respondents) but differed in the year of the survey (2018 vs 2011), representativeness (whole country vs. one city), the type of EQ-5D questionnaire (five-level vs. three-level) and the results obtained. In general, Vankova et al. found lower quality of life among respondents—within EQ VAS (scores about 8 points lower) and within the EQ-5D descriptive system (the percentage of ‘no problems’ answers across all five dimensions was 26.5%, versus 50.1% in the present study). In Burgas, there were also about 20% fewer respondents with 'no problems' answers within two dimensions—pain/discomfort and anxiety/depression. Analysis of the Burgas subpopulation from our study (5.8%), showed similar results to the Vankova study for the dimensions of mobility, self-care and usual activities. However, for the anxiety/depression domain, the results for the Burgas subpopulation in our study are similar to the general population of Bulgaria. Although we may hypothesise that the gap in time between the two surveys (7 years) influenced the perception of anxiety in Burgas inhabitants, this would need to be tested in a separate study.
Conclusions
In summary, the Bulgarian population norms which were developed for the descriptive part of EQ-5D-5L and EQ VAS may be used as reference values. The availability of such normative data should encourage the use of the EQ-5D-5L questionnaire in health-related quality-of-life studies in Bulgaria.
References
Puchalski, C.M.: Integrating spirituality into patient care: an essential element of person-centered care. Pol. Arch. Med. Wewn. 123, 491–497 (2013)
World Health Organization: WHOQOL: measuring quality of life, https://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/index4.html. Accessed 24 March 2020
Lin, X.J., Lin, I.M., Fan, S.Y.: Methodological issues in measuring health-related quality of life. Tzu Chi Med. J. 25, 8–12 (2013)
Fayers, P.M., Hays, R.: Assessing quality of life in clinical trials. Oxford University Press, Oxford (2005)
Lambert, C.M., Hurst, N.P.: Health economics as an aspect of health outcome: basic principles and application in rheumatoid arthritis. Br. J. Rheumatol. 34, 774–780 (1995)
Golicki, D., Niewada, M.: General population reference values for 3-level EQ-5D (EQ-5D-3L) questionnaire in Poland. Pol. Arch. Med. Wewn. 125, 18–26 (2015)
The National Institute for Health and Care: Guide to the methods of technology appraisal 2013. NICE. https://www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781/ (2018)
EuroQol Research Foundation: EQ-5D is a recommended tool for use in cost-utility analyses around the globe. https://euroqol.org/eq-5d-is-a-recommended-tool-for-use-in-cost-utility-analyses-around-the-globe/ (2018). Accessed 24 March 2020
Devlin, N.J., Brooks, R.: EQ-5D and the EuroQol Group: past, present and future. Appl. Health Econ. Health Policy. 15, 127–137 (2017)
Bharmal, M., Thomas, J.: Comparing the EQ-5D and the SF-6D descriptive systems to assess their ceiling effects in the US general population. Value Health. 9, 262–271 (2006)
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., Bonsel, G., Badia, X.: Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 20, 1727–1736 (2011)
Janssen, M.F., Pickard, A.S., Golicki, D., Gudex, C., Niewada, M., Scalone, L., Swinburn, P., Busschbach, J.: Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual. Life Res. 22, 1717–1727 (2013)
Buchholz, I., Janssen, M.F., Kohlmann, T., Feng, Y.S.: A systematic review of studies comparing the measurement properties of the three-level and five-level versions of the EQ-5D. Pharmacoeconomics. 36, 645–661 (2018)
Fayers, P.M., Machin, D.: Quality of life: the assessment, analysis and interpretation of patient-reported outcomes. Wiley, Chichester (2007)
Hinz, A., Kohlmann, T., Stobel-Richter, Y., Zenger, M., Brahler, E.: The quality of life questionnaire EQ-5D-5L: psychometric properties and normative values for the general German population. Qual. Life Res. 23, 443–447 (2014)
Huber, M.B., Felix, J., Vogelmann, M., Leidl, R.: Health-related quality of life of the general German population in 2015: results from the EQ-5D-5L. Int. J. Environ. Res. Public Health. 14(4), 426 (2017)
Grochtdreis, T., Dams, J., Konig, H.H., Konnopka, A.: Health-related quality of life measured with the EQ-5D-5L: estimation of normative index values based on a representative German population sample and value set. Eur. J. Health Econ. 20, 933–944 (2019)
Wong, E.L., Cheung, A.W., Wong, A.Y., Xu, R.H., Ramos-Goni, J.M., Rivero-Arias, O.: Normative profile of health-related quality of life for Hong Kong general population using preference-based instrument EQ-5D-5L. Value Health. 22, 916–924 (2019)
Purba, F.D., Hunfeld, J.A.M., Iskandarsyah, A., Fitriana, T.S., Sadarjoen, S.S., Passchier, J., Busschbach, J.J.V.: Quality of life of the Indonesian general population: test-retest reliability and population norms of the EQ-5D-5L and WHOQOL-BREF. PLoS ONE 13(5), e0197098 (2018)
Hobbins, A., Barry, L., Kelleher, D., O'Neill, C.: The health of the residents of Ireland: population norms for Ireland based on the EQ-5D-5L descriptive system—a cross sectional study. HRB Open Res 1, 22 (2018)
Shiroiwa, T., Fukuda, T., Ikeda, S., Igarashi, A., Noto, S., Saito, S., Shimozuma, K.: Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual. Life Res. 25, 707–719 (2016)
Golicki, D., Niewada, M.: EQ-5D-5L Polish population norms. Arch. Med. Sci. 13, 191–200 (2017)
Kim, T.H., Jo, M.W., Lee II, S., Kim, S.H., Chung, S.M.: Psychometric properties of the EQ-5D-5L in the general population of South Korea. Qual. Life Res. 22, 2245–2253 (2013)
Garcia-Gordillo, M.A., Adsuar, J.C., Olivares, P.R.: Normative values of EQ-5D-5L: in a Spanish representative population sample from Spanish Health Survey, 2011. Qual. Life Res. 25, 1313–1321 (2016)
Hernandez, G., Garin, O., Pardo, Y., Vilagut, G., Pont, A., Suarez, M., Neira, M., Rajmil, L., Gorostiza, I., Ramallo-Farina, Y., Cabases, J., Alonso, J., Ferrer, M.: Validity of the EQ-5D-5L and reference norms for the Spanish population. Qual. Life Res. 27, 2337–2348 (2018)
Bailey, H., Janssen, M.F., La Foucade, A., Kind, P.: EQ-5D-5L population norms and health inequalities for Trinidad and Tobago. PLoS ONE 14(4), e0214283 (2019)
Craig, B.M., Pickard, A.S., Lubetkin, E.I.: Health problems are more common, but less severe when measured using newer EQ-5D versions. J. Clin. Epidemiol. 67, 93–99 (2014)
Augustovski, F., Rey-Ares, L., Irazola, V., Garay, O.U., Gianneo, O., Fernandez, G., Morales, M., Gibbons, L., Ramos-Goni, J.M.: An EQ-5D-5L value set based on Uruguayan population preferences. Qual. Life Res. 25, 323–333 (2016)
Nguyen, L.H., Tran, B.X., Le Hoang, Q.N., Tran, T.T., Latkin, C.A.: Quality of life profile of general Vietnamese population using EQ-5D-5L. Health Qual. Life Outcomes. 15, 199 (2017)
Yfantopoulos, J.N., Chantzaras, A.E.: Validation and comparison of the psychometric properties of the EQ-5D-3L and EQ-5D-5L instruments in Greece. Eur. J. Health Econ. 18, 519–531 (2017)
Yang, Z., Busschbach, J., Liu, G., Luo, N.: EQ-5D-5L norms for the urban Chinese population in China. Health Qual. Life Outcomes. 16, 210 (2018)
McCaffrey, N., Kaambwa, B., Currow, D.C., Ratcliffe, J.: Health-related quality of life measured using the EQ-5D-5L: South Australian population norms. Health Qual. Life Outcomes. 14, 1–12 (2016)
Poder, T.G., Carrier, N., Kouakou, C.R.C.: Quebec health-related quality-of-life population norms using the EQ-5D-5L: decomposition by sociodemographic data and health problems. Value Health. 23, 251–259 (2020)
EuroQol Research Foundation. EQ-5D-5L User Guide. https://euroqol.org/publications/user-guides/ (2019). Accessed 24 March 2020
Golicki, D., Jakubczyk, M., Graczyk, K., Niewada, M.: Valuation of EQ-5D-5L Health States in Poland: the first EQ-VT-based study in Central and Eastern Europe. Pharmacoeconomics. 37, 1165–1176 (2019)
Altman, D.G.: Practical statistics for medical research. Chapman and Hall, London (1991)
Vankova, D., Kerekovska, A., Kostadinova, T., Todorova, L.: Researching health-related quality of life at a community level: results from a population survey conducted in Burgas, Bulgaria. Health Promot. Int. 31, 534–541 (2016)
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Encheva, M., Djambazov, S., Vekov, T. et al. EQ-5D-5L Bulgarian population norms. Eur J Health Econ 21, 1169–1178 (2020). https://doi.org/10.1007/s10198-020-01225-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-020-01225-5