
Abstract
This study aims at disentangling the causal effects of unemployment on physical and mental health from the selection of the unhealthy into unemployment. To identify causal effects, it explores hypotheses concerning how physical and mental health deterioration gain additional momentum with a longer duration of unemployment. In contrast, mere selection into unemployment implies time-constant effects of unemployment on physical and mental health. Fixed-effects models are applied to data from the German Socio-Economic Panel (GSOEP, 2002–2014, 74,572 observations). Pointing at causal effects of unemployment, the findings show that physical health does not deteriorate before, during or immediately after the period in which individuals lose their jobs, but that deterioration gains momentum later. The effect further depends on age at transition to unemployment. In contrast, a large part of the poorer mental health of the unemployed might be due to the selection of the unhealthy into unemployment; mental health declines even before job loss. Only for people who experience unemployment early in life, mental health deterioration gains some momentum in the time after the transition, indicating a (weak) causal effect of unemployment on mental health for younger individuals.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Unemployment, unemployment duration, and health: selection or causation?
In industrial and post-industrial societies, employment is a central aspect of social inequality because it provides access to both economic and social resources. In recent years, it has become increasingly apparent that health is another important dimension of inequality because it is essential to a long, satisfying and autonomous life. There is overwhelming empirical evidence that there is an association between inclusion in the working world and mental and physical health (for a meta-analysis of unemployment and mental health see [1], for a review of physical health see [2]). However, there are good arguments in both directions of influence. According to the causation thesis (1), unemployment causes people to become mentally and physically ill [3, 4]. According to the selection hypothesis (2), people with mental or physical health restrictions are at higher risk of losing their jobs (this selection effect is often referred to as reverse causality) and (3) will remain unemployed longer. There also might be confounding effects (4). Particularly, those with a poor education experience a higher risk of both unemployment and becoming ill. Probably, all of these mechanisms might be at work simultaneously. However, the major goals of this paper are to disentangle the mechanism based on causation from the others and to provide evidence of whether there is a causal effect of unemployment on mental and physical health.
Many empirical studies have attempted to disentangle these four mechanisms with observational data. One central aspect of these attempts is the comparison of intra-individual observations of health over time. Was there a deterioration of health before or after the transition to unemployment? However, even when exploring the temporal order of measurement in a panel, there is still the possibility that both health deterioration and transition to unemployment occur between the same two measurement points. Even very sophisticated approaches cannot completely dismiss selection: we cannot assess the true succession of health deterioration and job loss between two measurement points [5, 6]. As the current physical health status can be viewed as the cumulative result of health-related behaviour over the life course, a causal effect of unemployment on health might need a long time to gain momentum and might not be detected shortly after a transition to unemployment.
In this paper, I propose a method to isolate a causal effect of unemployment on physical and mental health focussing on how unemployment affects mental and physical health over time. Mere selection of the unhealthy into unemployment should imply more or less time-constant effects of unemployment on physical and mental health. In contrast, I suggest that the effect of unemployment on physical and mental health can be interpreted as a causal effect if health deterioration gains additional momentum with a longer duration of unemployment (“Background and hypotheses”). I will analyse indicators for mental and physical health from the German Socio-economic Panel (GSOEP) between 2002 and 2014 with a fixed-effects approach controlling for age and period (“Data and methods”) and present the results from testing my hypotheses concerning the time-dependent effect of unemployment on physical and mental health (“Results”). Adding substantially to the literature, the paper will conclude that there is a cumulative, and therefore, probably causal effect of unemployment duration on physical health, especially for those who face unemployment late in their working life. In contrast, most of the association of unemployment and poor mental health might be attributable to the selection of those with emotional problems into unemployment (“Discussion”).
Background and hypotheses
Social mechanisms
There are at least four potential social mechanisms behind the association of unemployment with physical and mental health.
Causation thesis
According to the causation hypothesis, unemployment causes people to become mentally or physically ill. In this view, the negative association of unemployment with mental health stems from manifest and latent deprivation [3, 4]. Manifest deprivation refers to income reduction as a major consequence of unemployment. The unemployed are forced to adjust their standard of living [7] and spend their savings. They lose both agency over their lives and the ability to plan for the future. These financial troubles cause distress. Moreover, if financial restrictions force individuals to relocate, existing social ties with family and friends may be disrupted [6: 129] and hence, social resources might vanish. In addition to this manifest deprivation, individuals suffer from latent deprivation [3]. For many individuals, employment plays an important social role and affects their self-conception, social identity and self-esteem. In addition, the workplace provides an important opportunity structure for social contacts. Thus, losing a job means losing all these sources of social and emotional support. Finally, in many cases, unemployed people may feel stigmatized [8]. Some aspects of latent deprivation, like the loss of the professional role or stigmatization may affect mental health more or less immediately or even in anticipation of a job loss [9]. However, most aspects of manifest and latent deprivation caused by unemployment might affect mental health later, because there are still some financial and social resources that help to buffer the negative impact. In particular, the German unemployment insurance pays 60% of the last net income for a period ranging from 6 to 24 months depending on the time having been employed and on age. And social contacts might not end abruptly but tend to fade out slowly. In the long run, however, individuals might adapt to deprivation, and mental health might recover in spite of continuing unemployment. In summary, unemployment might have a u-shaped effect on mental health. It leads to manifest and latent deprivation, affecting mental health not directly after a job loss, but within some months; however, adaption to the situation and hence recovery in spite of continuing unemployment appear to be possible.
Manifest and latent deprivation might affect not only mental but also physical health. Economic deprivation may force individuals to invest less in the maintenance of their physical health. They may stop expensive exercising (e.g., they cannot afford the monthly fee for their sports club), they will not be able to afford to buy healthy but more expensive food, and they will not invest in medical therapies that are not covered by their health insurance.Footnote 1 Moreover, manifest and latent deprivation and the resulting distress in the long run may both directly and indirectly, influence an individual’s physical status. For example, distress and depression lead to unhealthy patterns of behaviour such as smoking [13, but see 14], drinking, and reducing social and physical activity. Moreover, there is evidence that distress increases the risk of cardiovascular diseases [15, 16] and that the severely mentally ill are at higher risk of illnesses such as obesity, metabolic syndrome, diabetes mellitus and cardiovascular diseases, primarily mediated by an unhealthy lifestyle [17, 18].
In contrast to the more short-term and intermediate impacts of unemployment on mental health, the effects of manifest and latent deprivation on physical health are mediated by unhealthy patterns of behaviour only in the very long run and the effects might accumulate over time [19: 779]. Moreover, the effects of manifest deprivation will strengthen with enduring unemployment because the financial benefits from unemployment insurance expire after some time (see above). Therefore, the negative impact of unemployment on physical health will gain momentum only for long-enduring unemployment.
Selection of the unhealthy into unemployment (reverse causation)
Employees with poor health conditions might face a higher risk of being selected into unemployment [20,21,22,23,24,25,26]. Mental problems or physical restrictions might reduce an employee’s job performance or reliability, increase his/her days of absence and hence the probability of job loss [1, 27, 28: 268].
Selection of the healthy into re-employment
Third, once they are unemployed, ill persons will have a decreased chance of re-employment [1, 29,30,31,32,33, but see 34,35,36].
Confounding effect (indirect selection)
Fourth, both the risk of a poor health status and a high unemployment risk are correlated with other observable or unobservable characteristics. For example, the less-educated and those with a neurotic personality might be at a higher risk of both falling ill and losing a job [37,38,39].
The major goal of this paper is to disentangle the mechanism based on causation from the others.
Previous research
Longitudinal analyses have often been used to compare employed and not employed individuals [40] and more specifically, individuals who lose their jobs between two points in time compared with those who remain employed (see [1] for a meta-analysis). With the use of fixed-effects panel analyses [5], scholars neutralized unobserved heterogeneity in time-constant traits and, therefore, the confounding effects (especially with respect to qualification and personality). However, the central problem in conventional fixed-effects models is that they cannot eliminate selection based on short-term health shocks, i.e., a sudden deterioration of health between two waves that rapidly leads to a job loss.
One sophisticated method to eliminate unobserved heterogeneity and (long term) selection has been proposed by Gebel and Voßemer [6]. Using a propensity score-matching approach, they construct a treatment group of those who face the transition from employment to unemployment between two waves. This group is compared with a control group of “statistical twins” who are similar with respect to all control variables applied in the propensity score-matching procedure but without the treatment. By comparing the change in the health variable over time between both groups, they apply a difference-in-differences estimation. They find a negative effect of a transition into unemployment on mental health, but no effect on physical health. However, the difference-in-differences approach can either be applied in less complex fixed-effects models that control age and period effects [41: 966]. But even the more complex propensity score-matching approach cannot eliminate selection based on short-term health shocks.
To cope with this problem, and to eliminate selection of ill persons into unemployment in their analytical models, many researchers have relied on observing unemployment caused exclusively by factory closure, because many other reasons for unemployment might be endogenous. For example, an employee might be dismissed due to restricted productivity resulting from mental or physical health problems. These scholars argue that for factory closures, it seems unlikely that job loss has been caused by poor mental or physical health or any other individual characteristic [1, 5: 277]. Applying fixed-effects models to the German Socio-Economic Panel (GSOEP), Schmitz [5] finds no effects of job loss due to factory closure on health satisfaction, hospital visits, and mental health; there were only effects of job loss for other reasons. In his view, these effects are likely to result from health selection into unemployment. Therefore, and in accordance with earlier research [42,43,44,45,46,47], he concludes that the poor health status of the unemployed results from selection into unemployment. But other studies—even using the same data—find negative mental health impacts of unemployment due to plant closure on the dismissed and even on their spouses [48].Footnote 2 Nevertheless, we cannot conclude that the health deterioration of those who lose their jobs for reasons other than factory closure is completely the result of selection.
Several other approaches have been suggested to disentangle effects of causation and selection (reverse causation), in particular fixed-effects models with a lagged-dependent variable or structural equation models with cross-lagged effects.
Though all these approaches may be adequate in principle, the central shortcoming of all applications in prior research is that only two succeeding observation points in time are compared. However, the effect of unemployment on health might be very different based on the time people are exposed to the negative consequences of unemployment.
Hypotheses and methodological approach
As the examples from previous research show, even very sophisticated approaches cannot completely eliminate selection because we will never know the true sequence of two events between two measurement points. From this perspective, a deterioration of mental or physical health in the same time span as—or even prior to—the transition to unemployment might be the result of selection. Therefore, a potential causal effect is only detected when health deteriorates after the period that includes the transition to unemployment.
In contrast to prior research, I propose to disentangle the causal effect from the selection effect by focusing on the duration of unemployment. I suggest analysing hypotheses concerning how mental and physical health will develop in time after a job loss. As health selection into unemployment is the result of the health status before a job loss, it will produce a more or less time-constant association thereafter. In contrast, as discussed above, unemployment causes deprivation and changes in health behaviour that might affect physical health only in the long run and the effects might accumulate over time [19: 779]. Hence, I hypothesize (1) that the longer the exposure to unemployment, the stronger the negative effect of unemployment on physical health.
However, two theoretical scenarios with potential deviations from this reasoning should be discussed: First, when a health deterioration is being anticipated either by the employer or the employee and leads to a dismissal or a resignation, physical health might deteriorate after the transition to unemployment due to selection effects. But the anticipated health deterioration should happen more or less shortly after the transition to unemployment and not in the long run. The reason is that an employee will normally quit his/her job only if (s)he is incapacitated. Why should (s)he quit earlier and loose his/her entitlement for unemployment or incapacity benefits—even though (s)he is aware of a future decline in health? Why should an employer dismiss a productive employee now when his/her productivity is satisfying but might shrink in 3 or 4 years? How should the employer even know about it? Second, when a sudden, but progressive physical illness forces the employee first to quit or to be dismissed and then makes health deteriorate even further after the transition to unemployment, this should be also attributed to selection and not to causation but might be congruent with the temporal pattern of hypothesis (1). However, in the German social system, a heavy-progressive physical illnessFootnote 3 normally will not lead to unemployment but to a drop-out from the labour force, because people with a severe, long-enduring, and progressive illness normally do not search for a new job and they will not receive unemployment benefits but incapacity benefits from their health insurance. In total, both theoretical cases of a health deterioration while in unemployment but congruent with selection instead of causation either suggest additional health deterioration in the periods shortly after unemployment, whereas the general hypothesis congruent with causation is linked with long-enduring unemployment, or they are infrequent due to institutional regulations in the social system.
I further suggest that the impact of unemployment and its duration on physical health will vary based on the age at transition. Human physics becomes increasingly vulnerable over the life course, and the chances for a (complete) recovery after a physical deterioration are lower for older people (“Homeostenosis” [51: 982]). Hence, I hypothesize (2) that the older an individual is at job loss, the more rapidly the negative effect of unemployment on physical health will gain momentum.
With respect to the causal effect of unemployment on mental health, I argued that it will affect mental health only after some months after job loss, because people still may benefit from financial and social resources that will fade out slowly. In the long run, people might adapt to the situation and hence recover. Therefore, I hypothesize (3) that a job loss will have a u-shaped effect on mental health.
There are competing arguments about how age at job loss might interact with a causal effect of unemployment on mental health. One argument is that an older unemployed worker might find it more difficult to locate a new job, face a higher risk of social isolation and generally is at a higher risk to have suffered from mental disorders earlier in life than a younger worker. Hence, within the general u-shaped effect, a stronger deterioration of mental health could be assumed for those who experience a transition to unemployment late in their life course (hypothesis 4a). Conversely, continuing unemployment with no defined end point is likely to have more severe consequences for individuals’ life chances, such as developing a career, finding a partner, building a home and raising children, when they are still young and have not yet attained these life goals. Therefore, a long period of unemployment might affect mental health more severely during the early life course. In contrast, older unemployed might have already reached these goals. Moreover, younger individuals are more likely than older individuals to have family responsibilities (overview by [1: 266, 52]) and hence, manifest deprivation will lead to additional distress. Thus, I also hypothesize (4b) that—within the general u-shaped effect of unemployment duration on mental health (hypothesis 3), the younger the individual at transition to unemployment, the faster the negative effect of unemployment on mental health will gain momentum.
When we find these types of time paths that are congruent with causal effects of unemployment on physical or on mental health, but not with effects of selection of the less healthy into unemployment, causal effects are isolated.
Data and methods
Data and analysed sample
To analyse the derived hypotheses with the goal of isolating a potential causal effect, I conduct a panel analysis of the GSOEP between 2002 and 2014. Because the mental and physical health variables are available bi-annually, I constructed a seven waves panel (2002, 2004, 2006, 2008, 2010, 2012, and 2014). As usual for fixed effects-models, I only include all individuals who were employedFootnote 4 at one observation during the panel and subsequently remained in employment or experienced a transition into unemployment (at least one additional month in unemployment during the panel).Footnote 5 People who switch between employment and unemployment at a high frequency might nevertheless cumulate health risks over the various periods of unemployment. Therefore, I also included observations with re-employment after an unemployment period; hence, another period of unemployment may be observed for these individuals.Footnote 6 Note that for most respondents, I will use less than seven observations. All observations preceding the first period of employment, all observations after retirement or leaving the labour force for other reasons, observations with item non-response and all participants with only one observation in the panel have been deleted (see Table 1). In addition, there have been several refreshing samples added since 2002. For individuals in these samples, there are naturally fewer observations than for those from the sample that began in 2002.
After restricting the sample in this way, I will analyse 74,572 bi-annual observations from 17,274 individuals. In 5446 observations (representing 2984 individuals), there has been a period of unemployment (Table 1).
Health indicators
Since 2002, the GSOEP has provided the Mental Component Summary (MCS) scale as an indicator of mental health and the Physical Component Summary (PCS) scale for physical health every 2 years. The indicators are based on the items of the SF12v2, a short version of the internationally approved and reliable SF36v2-Index [54].Footnote 7 The SF12v2 items are based on self-reports concerning various dimensions of mental and physical health, such as general health, physical and social functioning, mental health, bodily pain, physical and emotional restriction on social role accomplishment, vitality and health-related restrictions on social contacts.Footnote 8 The items explicitly refer to the 4 weeks prior to the interview. In line with the WHO-definition of health, MCS and PCS are not disease-specific measures focusing on a particular condition or disease, but generic measures of mental and physical health [48: 548]. The PCS and MCS provide a fine-grained, reliable and valid representation of mental and physical health status [54, 56, 57]. The weights of the items in the two indices were calculated by exploratory factor analysis and the indices were transformed into norm-based scores with a mean of 50 and a standard deviation of 10 in 2004 [55]. In the analysed sample, the mental health scale has a mean of 50.4 and ranges between 3.1 (min) and 79.4 (max) and the physical health scale has a mean of 51.2 with a somewhat lower range between 9.2 (min) and 76.4 (max). See Table 2 for further details.
Measuring unemployment
To account for periods of unemployment shorter than 24 months, I measure transition into unemployment with a variable provided by the GSOEP that uses the monthly calendar spells of employment. The variable provides the cumulated duration of unemployment at every interview (in months). Hence, when there is an increase between two waves, there must have been at least one (additional) month in unemployment in the preceding 24 months. If so, a dummy variable (unemployed at least once during the preceding 24 months, ue) is set to one. In addition, I use the cumulative duration of unemployment (on a monthly basis) at each measurement point to estimate the cumulative effect of the duration of unemployment on health (ued). As a baseline, when a person is employed at a time point of the panel, both the dummy and the duration variable are set to zero. When a person had (additional) months in unemployment within the preceding 24 months, the dummy variable is set to one and the duration variable represents the cumulative duration of unemployment until the particular time point (in years of unemployment, derived from the monthly calendar data). This allows for several periods of unemployment during the panel and for an adequate measurement of the supposed cumulative effect of unemployment on health over time.
To employ an additional control for potential long-term health selection into unemployment, I use a dummy variable that is set to one exclusively for those observations that precede a new period of unemployment (uep, see “Research design” and “Appendix” for an illustration of how ue, ued, and uep are coded).
Sample description
As Table 2 shows, in observations of individuals with at least one transition into unemployment, people on average have poorer physical and mental health, are younger and have a lower household income. Only 20.6% have an Abitur (i.e., a high-school degree, allowing them to attend institutions of tertiary education), compared to 34.0% among those who did not experience any unemployment during the panel. Among the unemployed, there are more singles, slightly more females and some more people living with children. Table 2 also informs about the distribution of unemployment duration among those with at least one transition into unemployment. Even for very long durations of 9–12 years there are 56 observations.
Research design
Neither conventional OLS regression nor pooled OLS regression (POLS) with several measures for each individual can distinguish a causal effect of unemployment on mental or physical health from health selection into unemployment. These approaches essentially rely on the differences in the conditional mean of the dependent variable between individuals with different traits, controlling for other variables.
In a fixed-effects model, the intra-individual mean is subtracted from every measurement of all variables. Hence, a fixed-effects model exclusively focuses on the covariation of variables over several observations within individuals. It does not compare groups of individuals (between-comparison), but it does compare individuals with themselves at several measurement points (within-comparison). Since there is no intra-individual variation in time-constant traits, we thus implicitly control for any unobserved heterogeneity in those traits and eliminate the corresponding confounding effects [41, 58,59,60].
Within the fixed-effects model, the effect estimator of unemployment provides the average change in health of all individuals after a transition from employment to unemployment. However, we do not exactly know what has occurred in the 24 months between the two observations. Perhaps the individual has lost the job before his/her health deteriorated (causation), but it could have been the opposite and the individual suffered from a deterioration of health and thereafter lost his/her job as a consequence. Both paths would lead to a negative sign of the fixed effect of unemployment on health. Hence, the fixed effect of unemployment is suspected to be a mere consequence of a ‘short-term’ selection.
The effect of such a ‘short-term’ selection between two waves of the panel should be more or less time-constant during unemployment. In contrast, causal effects of unemployment on mental or physical health should gain momentum only after a transition to and during a period of unemployment. Therefore, if we attempt to isolate a causal effect of unemployment on health, we should demonstrate that the effect of unemployment on health does not primarily depend on the employment status, but that it develops according to the time paths as hypothesized above.
The applied estimation model is given in Eq. (1):
where y denotes the physical or mental health status according to the pcs and mcs scales. ue is a dummy that is set to one if there were any period of unemployment at least once during the preceding 24 months. ued denotes the cumulative duration of unemployment (measured on a monthly basis, but in years). When ue = 0, ued is set to zero either. When ue = 1, ued represents the cumulative duration of unemployment while in the panel. To allow for non-linear effects of duration of unemployment, for some analyses, unemployment duration is classified in 2-year periods. uep is a dummy variable that is set to one exclusively for those observations in employment that precede a new period of unemployment. X is a vector of additional time-varying covariates, in particular age and period dummies. And ε denotes an intra-individual error term.
Table 5 in the "Appendix" illustrates the coding of ue, uep, and uep for four typical cases.
Note that a fixed effects-estimator of unemployment on health is based exclusively on those respondents who have experienced a transition to unemployment (average treatment effect on the treated, ATET). Hence, we have no information about how the health of those without a transition would develop if they had experienced a transition. Nevertheless, ue provides information about the intra-individual time-constant health deterioration caused by a transition into unemployment [41: 966].
A negative sign of ued indicates increasing health deterioration with every additional year of unemployment, pointing to a causation effect. Both ue and ued are estimated net of age, period, all time-constant confounders and the other time-varying covariates controlled for in vector X. Hence, the effects of unemployment ue and its duration ued are not mere effects of ageing, but indicate a deterioration of health in addition to the age effect.
Finally, the effect estimator of uep indicates whether health is better or worse in periods with employment immediately preceding a transition to unemployment compared to ‘normal’ observations in employment of the same individuals. A negative sign in this variable is either a clue for a long-term selection of the unhealthy into unemployment or for a decline in particular of mental health due to an anticipation of being dismissed within the next 24 months.
It may be argued that a negative time trend in the physical health of the unemployed could be the result of selective re-employment. As the period of unemployment continues, the healthier unemployed might locate a new job and leave behind those in poorer health. According to this argument, individuals who remain unemployed are compared with those who secure a new job (between-comparison). However, in the fixed-effects approach in Eq. (1), all differences between individuals are neutralized. The FE estimator of unemployment duration (ued) indicates the health change within individuals with every additional year of unemployment compared to the situation prior to the job loss. Hence, the suspected effect of a health-selection into re-employment on the estimator of unemployment duration is eliminated by removing all between-variance.
Because an FE model only controls for time-constant unobserved heterogeneity, the presented models will additionally control for mobility in education, and living with a partner and children, summarized in vector X.
Results
Unemployment and physical health
What are the effects of unemployment and its duration on physical health controlling for age and other covariates? Table 3 presents in model I the results of a pooled ordinary least square regression (POLS). This model does not control for unobserved heterogeneity. Controlling for age, education, and household constellation, the physical health component scale (PCS) is approximately 2.0 points lower for those who experienced at least one period of unemployment in the 24 months preceding the measurement. This effect contains both differences within and between individuals. Therefore, we do not know whether the transition to unemployment has contributed to poorer health (causal effect) or whether those with a poorer health status had a higher risk of job loss (selection). The corresponding fixed-effects model (FE, Model II), additionally controlling for period effects, provides a considerably lower within-individual difference of approximately − 0.30. Hence, a considerable amount of the health difference in the POLS of Model I is driven by a long-term health selection into unemployment or by time-constant confounders. Within the same individual, during periods of unemployment, physical health on average is 0.30 scale points lower than in periods of employment, controlling for age and period. However, we do not know what exactly has occurred between the two intra-individual measurements. Did individuals first face unemployment and then become ill (causation) or vice versa (short-term selection)? Hence, the effect might still be attributable to selection.
Therefore, in Model III, I add the dummy for the observation preceding the transition to unemployment (uep) and the duration of unemployment (ued). uep shows a small negative effect, indicating that individuals who will experience a job loss in the next period were slightly worse off before the transition. However, the estimator is only slightly significant at the 10% level.Footnote 9ue becomes insignificant and positive, whereas the duration of unemployment (ued) now has a strong negative effect. With every additional 12 months of unemployment, physical health deterioration is 0.42 scale points worse compared to the situation prior to the transition. Hence, supporting hypothesis 1, there is a cumulative effect of unemployment duration on physical health. Since I have controlled for age, we can say that enduring unemployment accelerates natural health deterioration. In contrast, a short-term selection with a deterioration of physical health and a subsequent transition to unemployment within 24 months should lead to a time-constant effect of unemployment and is not congruent with the discovered pattern of cumulative health deterioration of unemployment. Therefore, I conclude that there are strong clues for a causal effect.Footnote 10
In Models IV, V, and VI, I add interactions of age at transition and unemployment (ue) and of age at transition and duration of unemployment (ued) to test hypothesis 2. Models IV and V show that we find significant effects for both interactions. When including both interaction effects simultaneously, only the interaction of age at transition and ued remains significant (Model VI).
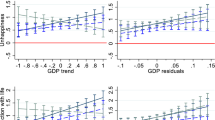
Therefore, I will use Model V for further interpretation. Because of its complexity, I will discuss a conditional effects plot based on the findings in Model V. Figure 1 presents the isolated effect of health deterioration attributable to unemployment based on time since transition to unemployment, net the natural health deterioration caused by ageing and the other covariates. In accordance with hypothesis 2, it shows that the deterioration of physical health gains more momentum over time for individuals who lost their jobs at older ages. For those who lost their jobs at age 55, the unemployment effect after 12 years (at age 67) is approximately 8 points—in addition to natural ageing. For them, one additional year of unemployment deteriorates health by (0.12 − 0.02 × (55 − 18)) = − 0.62 points—in addition to natural ageing (− 0.37 points on the pcs).Footnote 11 In contrast, those who became unemployed at age 25 face no deterioration of physical health. Therefore, I find support for hypothesis 2. The deterioration of physical health gains momentum during unemployment and is faster for those who face unemployment later in their life courses.

Unemployment and mental health
In Table 4, I present similar models as in Table 3 for the effects of unemployment on mental health. Again, the POLS in Model I shows a lower value of the mental health scale for those who were unemployed at least once in the 24 months preceding the observation (between- and within-differences). The fixed-effects estimator ue in Model II is considerably lower because the between-differences have been removed. Hence, there are considerable effects of a long-term selection of the unhealthy into unemployment. Since I hypothesized a u-shaped effect of unemployment duration on mental health, I use dummies for unemployment duration classified in 2-years intervals in Model III. However, none of them shows a significant difference to ued < 1 year (p < 0.05), whereas both the dummy for being unemployed in the last 24 months and the dummy indicating the observation preceding the job loss show a highly significant strong negative effect. Model IV comes to similar conclusions assuming a linear effect of ued. Hence, these findings do not support hypothesis 3. Instead, compared to observations during employment of the same individuals, mental health is worse in all observations during unemployment at a similar level. Hence, the results are congruent with both causation and with a short-term selection, and it remains unclear whether unemployment causes a deterioration of mental health or whether those with a deterioration of mental health in the preceding 24 months are selected into unemployment. Compared to other observations during employment, mental health is worse in observations immediately preceding a period of unemployment (uep). This effect indicates either a long-term selection into unemployment after a deterioration of mental health or a long-term anticipation of being layed-off causing a poorer mental health.
In Models V, VI, and VII, I test for interaction of age at transition and unemployment (V), age at transition and duration of unemployment (VI), and both (VII). The interaction terms are significant only in Model VII. For ease of interpretation, I use another conditional effects plot of the effect of unemployment on mental health by duration of unemployment and age at transition net the age and period effects. Based on Model VII, Fig. 2 shows that for those who experience the transition to unemployment early in their life course (at ages 25 and 30), there actually is a (small) negative linear effect of unemployment duration. Slightly pointing at a causal effect, for the 25- and 30 year olds, mental health deteriorates after the transition to unemployment, and the difference in the observations of unemployment and employment of the same individual increases as unemployment endures. Hence, hypothesis 3 finds (weak) support with respect to these younger age groups. This finding also weakly supports hypothesis 4b that the younger the unemployed, the faster the negative effect of unemployment on mental health. When a job loss occurs later in the life course (especially at ages 50 and 55), mental health does not deteriorate compared to the situation before the transition to unemployment. Instead, the older unemployed rapidly recover from their poorer mental health in the observation preceding the period of unemployment (uep) and immediately after the job loss (ue). Hence, I do not find support for hypothesis 4a that a stronger deterioration of mental health is more likely for those who experience unemployment later in their life course.

Robustness checks
I performed several robustness checks. In preliminary analyses, I used dummies to model the effect of unemployment duration on physical health either; the linear model is adequate at least during the first 9 years of unemployment. Deviations from the linear model at longer durations were moderate. Nevertheless, I restricted the analysis to a duration of unemployment of only 9 years in another robustness check. The findings are qualitatively similar to those reported, but contrasts for age at transition to unemployment are slightly smaller.
For the presented results, I allowed for more than one spell of unemployment while in the panel. The results are qualitatively the same when cutting observations after the first spell of unemployment per respondent. There is one exception: When allowing only one spell of unemployment, physical health deteriorates significantly even at the observation preceding the unemployment spell (uep), indicating a selection effect in addition to the strong clues for a causal effect. Maybe some (small) part of the deterioration of physical health after a transition to unemployment is due to a process of health deterioration that has started even in the period before the transition and might be attributable to selection.
Furthermore, two items of the SF12v2 are formulated in terms of work requirements. Respondents were asked during the last 4 weeks how often they felt that they achieved less than they wanted to at work or in everyday activities because of physical health problems and mental/emotional problems, respectively. In a similar manner, respondents were asked whether they felt limited either at work or in everyday activities. Since the PCS and MCS, therefore, might be sensitive to whether one is employed, I additionally controlled for the corresponding subscales concerning the physical and emotional restriction on social role accomplishment. The findings show no qualitative differences to those presented above. With respect to physical health, the contrasts with respect to unemployment duration and age at transition to unemployment in Fig. 1 are smaller. With respect to mental health in Fig. 2, the contrasts are larger.
To test for ceiling and level effects, I controlled for the interaction of the experience of unemployment accumulated at the start of the panel with (1) unemployment in the preceding 24 months, (2) duration of unemployment, and (3) the indicator for the observation preceding a new unemployment period. There were no qualitative differences in these results.
Discussion
This paper sought to disentangle the causal effects of unemployment on physical and mental health from selection and confounding effects. In contrast to previous studies, I formulate hypotheses concerning the influence of unemployment’s duration on health. The central findings are (1) that there is a considerable long-term selection of the physically unhealthy into unemployment, (2) that physical health does not additionally deteriorate directly in the period of job loss, but (3) that health deterioration (in addition to natural deterioration caused by ageing) gains momentum during unemployment, and (4) that the size of this effect depends on age. The older individuals are at transition to unemployment, the more vulnerable their physical health and the more rapidly it declines. The found negative time trend in physical health cannot be the result of a selection of healthier individuals into re-employment because the fixed-effects approach eliminates all inter-individual differences and exclusively compares observations over time within individuals. Hence, the results point at a causal effect of unemployment on physical health because I have found a time path that is congruent with a theoretical argument pointing to causation. Nevertheless, this conclusion might be limited because the found time trend might be congruent with a selection due to anticipating future deterioration of physical health. Both employers and employees might anticipate a pending decline in physical health of the employee and may decide to dismiss or resign, respectively. And the conclusion may be limited because some part of the deterioration of physical health after a transition to unemployment might be due to a process of health deterioration that has started even in the period before the transition and might be attributable to selection. However, as discussed above, these scenarios might be infrequent or they suggest a substantial additional health deterioration in the periods shortly after unemployment, whereas the general result is that the cumulative deterioration of physical health is linked with long-enduring unemployment.
In contrast, (5) findings imply that the poorer mental health of the unemployed seems primarily attributable to long- and short-term selection (reverse causality)—or to anticipation effects. Mental health reduces even at the observation preceding the period of unemployment. (6) Only for those who face unemployment early in their life course, mental health additionally worsens during unemployment, only slightly pointing to a causal effect. In contrast, older age groups can even experience a mental recovery while unemployed. Perhaps older unemployed are better able to adapt to the situation than younger unemployed. In addition, at older ages, employment might be a stronger source of distress, and being unemployed is a chance to recover in a manner similar to that which has been shown for retirement [61]. However, the finding that mental health is even worse in the observation preceding a job loss—although it is a clue for selection of those with a mental breakdown into unemployment—might result from the anticipation of a job loss and might hence be due to causation. In addition, the mental health measure might be more volatile over time than physical health. Hence, within the 24 months between observations, many ups and downs may be undetected that may be attributable to losing or finding a (new) job and hence, causation. In total, the findings on mental health are much more ambiguous than those on physical health.
In summary, I found that—in addition to a selection of the unhealthy into unemployment–unemployment causes an acceleration of physical health deterioration and this acceleration is stronger the older individuals are at the time of transition to unemployment. In contrast, the poorer mental health of the unemployed is probably a result of selection of those with poor mental health into unemployment. The only exceptions with weak clues for a causal effect are those who experience long-lasting unemployment early in life and those who anticipate losing their jobs.
Using the same data as I did, Schmitz [5] found no effect of unemployment caused by plant closure on health satisfaction and mental health. Gebel and Voßemer [6] found that unemployment affects individuals’ mental but not their physical health. However, both Schmitz, Gebel and Voßemer restricted their analysis to the two points in time preceding and following the transition to unemployment. Actually, their results are consistent with my findings: At the time of job loss, mental health is (slightly) worse than before, and I do not find any short-term effects on physical health. However, the general conclusion in the prior studies is that there are no clues for causal effects of unemployment on physical health. In contrast, I theoretically argue that the negative effect of unemployment on mental and physical health apparently requires additional time to accumulate with enduring unemployment, and I find empirical evidence that there is such an accumulation effect with respect to physical health. This accumulation effect can be interpreted as a strong clue for a causal effect.
As already discussed, the conclusions above may be limited in some cases due to the possibility of anticipation effects or due to a process of health deterioration that has started even in the period before the transition to unemployment. Moreover, the time-constant effect of unemployment on mental health is only suspect to be due to short-term selection. Hence, we simply do not know whether the found time-constant fixed effect of unemployment on mental health is due to causation or due to selection.
The following questions remain open for further research: Will physical health recover after finding a new job? The association of unemployment with mental and physical health might depend on other economic and social resources, such as household income, education or social embeddedness. Do these resources moderate a health selection into unemployment and prevent workers from losing their jobs because of poor mental or physical health? Or do these resources moderate a causal effect and assist in maintaining good health even during unemployment?
Appendix: Illustration of coding of the variables uep, ue, and ued
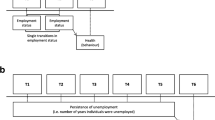
Table 5 illustrates the coding of the variables uep, ue, and ued. To keep it simple, all respondents in the example were observed at seven time-points. Case 1 shows a respondent employee who stays employed throughout the panel. ued, ue, and ued rest at zero throughout the panel. Case 2 represents a respondent who loses his job 6 months before the 2006 interview with no re-employment during the rest of the panel. Hence, uep marks the observation preceding the unemployment period in 2004 with the value one; ue marks every observation from 2006 until 2014 with one; and ued changes to 0.5 years at the 2006 observation, because the individual already experienced 6 months of unemployment then. At every further point of observation, ued increases by another two years. Case 3 shows what happens if the individual finds a new job between the 2008 and the 2010 interview: All three variables change to zero again. And case 4 illustrates multiple transitions to unemployment. Note that ued cumulates over the multiple periods of unemployment. In 2010, it would have been four years (another 1.5 years of unemployment before re-employment) but is set to zero while employed. The second unemployment period starts one month before the 2012 interview; hence 1/12 of a year (0.083) is added to ued.
Notes
In contrast to other countries, in Germany, the unemployed are not dropped from public health insurance. However, in recent decades, the catalogue of public health insurance benefits has been restricted to the basics [10]. Therefore, many people have to purchase additional insurance policies [11, 12] or pay for some therapies themselves.
Some shortcomings of this approach have been discussed in the literature: Factory closures are very infrequent events, a job loss caused by a plant closure may have different mental consequences than losing a job due to an individual’s performance [49: 362], and those who lost their jobs due to a plant closure constitute a very selected group [49: 362, 46: 1397, 50].
If the progressive illness has not yet a heavy impact on work performance, the discussed first scenario for an anticipated decline in health holds.
Persons on parental leave or in military service are treated as being employed because these people later may be at risk of unemployment during the panel.
Note that in some cases, within the 24 months between two waves employment might not be directly followed by unemployment but by some months of inactivity before starting a new job search.
As is discussed in Sect. “Robustness checks”, the results of the analysis stay qualitatively unchanged, when the analysis is restricted to only one period of unemployment per respondent.
For the application in the GSOEP, the SF12v2 has been slightly modified (see [55] for details).
See [48: Appendix A2 on page 556] for an English documentation of the questionnaire.
Please note that when allowing only one spell of unemployment, physical health deteriorates significantly at the observation preceding the unemployment spell, indicating a selection effect. See Sect. “Robustness checks” for a discussion.
See “Hypotheses and methodological approach” and “Discussion” for limitations to this conclusion.
The discussed effects rely on a sufficient number of cases, even at high durations of unemployment. As documented in Table 2, there are 56 observations with an unemployment duration between 9 and 12 years. And, as documented in Sect. “Robustness checks”, there are highly significant and strong effects for high unemployment durations when using a dummy-system.
References
Paul, K.I., Moser, K.: Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 74(3), 264–282 (2009). https://doi.org/10.1016/j.jvb.2009.01.001
Wanberg, C.R.: The individual experience of unemployment. Annu. Rev. Psychol. 63, 369–396 (2012). https://doi.org/10.1146/annurev-psych-120710-100500
Jahoda, M.: Employment and Unemployment. Cambridge University Press, Cambridge (1982)
Jahoda, M.: Unemployed men at work. In: Fryer, D., Ullah, P. (eds.) Unemployed People. Social and Psychological Perspectives, pp. 1–73. Open University Press, Milton Keynes (1987)
Schmitz, H.: Why are the unemployed in worse health? Labour Econ. 18(1), 71–78 (2011). https://doi.org/10.1016/j.labeco.2010.08.005
Gebel, M., Voßemer, J.: The impact of employment transitions on health in Germany. A difference-in-differences propensity score matching approach. Soc. Sci. Med. 108, 128–136 (2014). https://doi.org/10.1016/j.socscimed.2014.02.039
Korpi, T.: Accumulating disadvantage. Longitudinal analyses of unemployment and physical health in representative samples of the Swedish population. Eur. Sociol. Rev. 17(3), 255–273 (2001). https://doi.org/10.1093/esr/17.3.255
Young, C.: Losing a job: the nonpecuniary cost of unemployment in the United States. Soc. Forces 91(2), 609–634 (2012). https://doi.org/10.1093/sf/sos071
Ferrie, J.E., Shipley, M.J., Marmot, M.G., Stansfeld, S., Davey Smith G: Health effects of anticipation of job change and non-employment: longitudinal data from the Whitehall II study. BMJ 311, 1264–1269 (1995)
Lisac, M., Reimers, L., Henke, K.-D., Schlette, S.: Access and choice—competition under the roof of solidarity in German health care: an analysis of health policy reforms since 2004. Health Econ. Policy Law 5(1), 31–52 (2010). https://doi.org/10.1017/S1744133109990144
Zok, K.: Bonusprogramme und Zusatzversicherungen in der GKV. WIdOmonitor 2(1), 1–7 (2005)
Zok, K.: Interesse an privaten Zusatzversicherungen. WIdOmonitor 6(2), 1–8 (2009)
Marcus, J.: Does job loss make you smoke and gain weight? Economica 81, 626–648 (2014)
Schunck, R., Rogge, B.G.: No causal effect of unemployment on smoking? A German panel study. Int. J. Public Health 57(6), 867–874 (2012)
Low, C.A., Thurston, R.C., Matthews, K.A.: Psychosocial factors in the development of heart disease in women: current research and future directions. Psychosom. Med. 72(9), 842–854 (2010). https://doi.org/10.1097/PSY.0b013e3181f6934f
Steptoe, A., Kivimäki, M.: Stress and cardiovascular disease: an update on current knowledge. Annu. Rev. Public Health 34, 337–354 (2013). https://doi.org/10.1146/annurev-publhealth-031912-114452
De Hert, M., Correll, C.U., Bobes, J., Cetkovich-Bakmas, M., Cohen, D., Asai, I., Detraux, J., Gautam, S., Möller, H.-J., Ndetei, D.M., Newcomer, J.W., Uwakwe, R.L.S.: Physical illness in patients with severe mental disorders. World Psychiatry. 10(1), 52–77 (2011). https://doi.org/10.1002/j.2051-5545.2011.tb00014.x
Collins, E., Tranter, S., Irvine, F.: The physical health of the seriously mentally ill: an overview of the literature. J. Psychiatr. Ment. Health Nurs. 19(7), 638–646 (2012). https://doi.org/10.1111/j.1365-2850.2011.01831.x
Kuh, D., Ben-Shlomo, Y., Lynch, J., Hallqvist, J., Power, C.: Life course epidemiology. J. Epidemiol. Commun. Health 57, 778–783 (2003)
Christensen, U., Kriegbaum, M., Hougaard, C.O., Mortensen, O.S., Diderichsen, F.: Contextual factors and social consequences of incident disease. Eur. J. Public Health. 18(5), 454–459 (2008). https://doi.org/10.1093/eurpub/ckn049
Varekamp, I., van Dijk, F.J.H.: Workplace problems and solutions for employees with chronic diseases. Occup. Med. 60(4), 287–293 (2010). https://doi.org/10.1093/occmed/kqq078
García-Gómez, P., Jones, A.M., Rice, N.: Health effects on labour market exits and entries. Labour Econ. 17(1), 62–76 (2010). https://doi.org/10.1016/j.labeco.2009.04.004
Riphahn, R.T.: Income and employment effects of health shocks. A test case for the German welfare state. J. Popul. Econ. 12(3), 363–389 (1999). https://doi.org/10.1007/s001480050104
Lindholm, C., Burström, B., Diderichsen, F.: Does chronic illness cause adverse social and economic consequences among Swedes? Scand. J. Public Health. 29(1), 63–70 (2001). https://doi.org/10.1080/14034940151107064
Weber, A., Hörmann, G., Heipertz, W.: Arbeitslosigkeit und Gesundheit aus sozialmedizinischer Sicht. Deutsches Ärzteblatt 104(43), 2957–2962 (2007)
Chandola, T., Bartley, M., Sacker, A., Jenkinson, C., Marmot, M.: Health selection in the Whitehall II study. UK. Soc. Sci. Med. 56(10), 2059–2072 (2003). https://doi.org/10.1016/S0277-9536(02)00201-0
Matsekaasa, A.: Unemployment and health. J Commun. Appl. Soc. Psychol. 6(3), 189–205 (1996). https://doi.org/10.1002/(SICI)1099-1298(199608)6:3<189::AID-CASP366>3.0.CO;2-O
Varekamp, I., van Dijk, F.J.H., Kroll, L.E.: Workers with a chronic disease and work disability. Problems and solutions. Bundesgesundheitsblatt Gesundh. Gesundh. 56(3), 406–414 (2013). https://doi.org/10.1007/s00103-012-1621-1
Cardano, M., Costa, G., Demaria, M.: Social mobility and health in the Turin longitudinal study. Soc. Sci. Med. 58(8), 1563–1574 (2004). https://doi.org/10.1016/S0277-9536(03)00354-X
Stewart, J.M.: The impact of health status on the duration of unemployment spells and the implications for studies of the impact of unemployment on health status. J Health Econ. 20(5), 781–796 (2001). https://doi.org/10.1016/S0167-6296(01)00087-X
Wynne, R., McAnney, D.: Employment and Disability. European Foundation for the Improvement of Living and Working Conditions, Dublin (2004)
OECD: Employment Outlook 2003. OECD, Paris (2003)
Vinokur, A.D., Schul, Y.: The web of coping resources and pathways to reemployment following a job loss. J. Occup. Health Psychol. 7(1), 68–83 (2002). https://doi.org/10.1037/1076-8998.7.1.68
Crossley, C.D., Stanton, J.M.: Negative affect and job search. J. Vocat. Behav. 66(3), 549–560 (2005). https://doi.org/10.1016/j.jvb.2004.05.002
Wanberg, C.R., Zhu, J., Van Hooft, E.A.J.: The job search grind: perceived progress, self-reactions, and self-regulation of search effort. Acad. Manag. J. 53(4), 788–807 (2010)
Ginexi, E.M., Howe, G.W., Caplan, R.D.: Depression and control beliefs in relation to reemployment: what are the directions of effect? J. Occup. Health Psychol. 5(3), 323–336 (2000). https://doi.org/10.1037/1076-8998.5.3.323
Möller, J., Schmillen, A.: Verteilung von Arbeitslosigkeit im Erwerbsleben, vol. 24. Kurzberichte des Instituts für Arbeitsmarkt- und Berufsforschung, pp. 1–8 (2008)
Weber, B., Weber, E.: Qualifikation und Arbeitsmarkt: Bildung ist der beste Schutz vor Arbeitslosigkeit, vol. 4. Kurzberichte des Instituts für Arbeitsmarkt- und Berufsforschung, pp. 1–8 (2013)
Bartley, M., Ferrie, J., Montgomery, S.M.: Living in a high-unemployment economy. In: Marmot, M., Wilkinson, R.G. (eds.) Social Determinants of Health, pp. 81–104. Oxford University Press, Oxford (1999)
Ross, C.E., Mirowsky, J.: Does employment affect health? J. Health Soc. Behav. 36(3), 230–243 (1995)
Brüderl, J.: Kausalanalyse mit Paneldaten. In: Wolf, C., Best, H. (eds.) Handbuch der Sozialwissenschaftlichen Datenanalyse, pp. 963–994. VS Verlag für Sozialwissenschaften, Springer Fachmedien, Wiesbaden (2010)
Browning, M., Dano, A.M., Heinesen, E.: Job displacement and stress-related health outcomes. Health Econ. 15(10), 1061–1075 (2006). https://doi.org/10.1002/hec.1101
Salm, M.: Does job loss cause ill health? Health Econ. 18(9), 1075–1089 (2009). https://doi.org/10.1002/hec.1537
Kuhn, A., Lalive, R., Zweimüller, J.: The public health costs of job loss. J Health Econ. 28(6), 1099–1115 (2009). https://doi.org/10.1016/j.jhealeco.2009.09.004
Sullivan, D., von Wachter, T.: Job displacement and mortality: an analysis using administrative data. Q. J. Econ. 124(3), 1265–1306 (2009). https://doi.org/10.1162/qjec.2009.124.3.1265
Eliason, M., Storrie, D.: Does job loss shorten life? J Human Resour 44(2), 277–302 (2009)
Böckerman, P., Ilmakunnas, P.: Unemployment and self-assessed health: evidence from panel data. Health Econ. 18(2), 161–179 (2009). https://doi.org/10.1002/hec.1361
Marcus, J.: The effect of unemployment on the mental health of spouses—evidence from plant closures in Germany. J Health Econ 32, 546–558 (2013)
Brand, J.E.: The far-reaching impact of job loss and unemployment. Ann. Rev. Sociol. 41, 359–375 (2015). https://doi.org/10.1146/annurev-soc-071913-043237
Schwerdt, G.: Labor turnover before plant closure: “leaving the sinking ship” vs. “captain throwing ballast overboard”. Labour Econ. 18(1), 93–101 (2011). https://doi.org/10.1016/j.labeco.2010.08.003
Ben-Shlomo, Y., Cooper, R., Kuh, D.: The last two decades of life course epidemiology, and its relevance for research on ageing. Int. J. Epidemiol. 45(4), 973–988 (2016). https://doi.org/10.1093/ije/dyw096
Jackson, P.R., Warr, P.B.: Unemployment and psychological ill-health. Psychol. Med. 14(3), 605 (1984). https://doi.org/10.1017/S003329170001521X
World Health Organisation (2018). http://www.who.int/features/factfiles/mental_health/en/. Accessed 30 Apr 2018
Ware, J.E., Dewey, J.E., Kosinski, M.: How to Score Version 2 of the SF-36 Health Survey. QualityMetric, Lincoln (2001)
Andersen, H.H., Mühlbacher, A., Nübling, M., Schupp, J., Wagner, G.G.: Computation of standard values for physical and mental health scale scores using the SOEP version of SF-12v2. Schmollers Jahrbuch 127(1), 171–182 (2007)
Gill, S.C., Butterworth, P., Rodgers, B., Mackinnon, A.: Validity of the mental health component scale of the 12-item Short-Form Health Survey (MCS-12) as measure of common mental disorders in the general population. Psychiatry Res. 152(1), 63–71 (2007)
Salyers, M.P., Bosworth, H.B., Swanson, J.W., Lamb, J., Osher, F.C.: Reliability and validity of the SF-12 health survey among people with severe mental illness. Med. Care 38(11), 1141–1150 (2000)
Allison, P.D.: Using panel data to estimate the effects of events. Sociol. Methods Res. 23, 174–199 (1994)
Angrist, J.D., Pischke, J.-S.: Mostly Harmless Econometrics. Princeton University Press, Princeton (2009)
Halaby, C.N.: Panel models in sociological research: theory into practice. Ann. Rev. Sociol. 30(1), 507–544 (2004). https://doi.org/10.1146/annurev.soc.30.012703.110629 doi
van den Bogaard, L., Henkens, K., Kalmijn, M.: Retirement as a relief? The role of physical job demands and psychological job stress for effects of retirement on self-rated health. Eur. Sociol. Rev. 32(2), 295–306 (2016). https://doi.org/10.1093/esr/jcv135
Acknowledgements
I would like to thank Nico Seifert, the Thomas Klein working group at the Max Weber Institute in Heidelberg and participants in several presentations for their useful comments on earlier versions of this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Stauder, J. Unemployment, unemployment duration, and health: selection or causation?. Eur J Health Econ 20, 59–73 (2019). https://doi.org/10.1007/s10198-018-0982-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-018-0982-2