
Abstract
Among 55–64 year olds, poor health is a reason for leaving the labour market early within the framework of schemes such as not only Early Retirement for Certain Employees (or Early Retirement for Asbestos Workers), but also by absence from the workforce (sick pay and disability pensions, respectively). It is interesting to single out the controlling factors for participation in or absence from the labour market after 50 and the link between poor health and employment status. The prevalence of functional limitations in everyday activities leads to a more pronounced exclusion of those over 50 years old from the labour market. Some of those aged between 55 and 59 on disability benefits become unemployed and do not look for work; in other words, they are potentially exempted from job-seeking. This would confirm the hypothesis that some of those exempted from job-seeking are in poor health.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In France, public mechanisms for early retirement, which were originally intended to encourage the employment of younger people, but also to manage redundancies in businesses with economic problems, are gradually being replaced by new mechanisms, such as early retirement for some employees faced with hard working conditions (night work, for example), early retirement for asbestos workersFootnote 1 and particularly job-seeking exemptions up to July 2008. Acquiring a disability pension is another means of early retirement from the labour market, an approach used in Scandinavian countries where increasing recourse to disability pensions is possible in a generously funded health insurance system [14]. Many empirical studies have shown that poor health status affects the behaviour of older people who retire early from the labour market [13, 23]. Early retirement for health reasons can limit the efficacy of measures to postpone the retirement age by encouraging older people to work. Hence, an understanding of the relationship between health and employment status is essential.
We also consider the approaches used by unhealthy people in order to retire early. More precisely, what role could job-seeking exemptions play in managing health-related incapacity to work? What retirement mechanisms exist in France, and which of these are devoted to compensating for unhealthy conditions?
Thus, the task here is to study retirement behaviour in unhealthy people in the population aged 50–59, particularly for those who can use non-health-related mechanisms such as job-seeking exemptions. Before describing the empirical study, we present a brief overview of current approaches to early retirement in France. This is followed by a short review of the literature on the relationship between health and employment statuses. We present three analyses:
-
The first aims to validate the healthy worker effect’s assumption in the labour market by testing the relationship between poor health and premature exit from the labour market at the end of working life.
-
Then, in the non-working population, it is instructive to look at the relationship between health and non-working statuses (with and without recognition of handicap) on one hand and between health and unemployment statuses on the other. These two analyses aim to examine those situations in which non-working and unhealthy people use health-related mechanisms (recipients of disability pensions) and those in which they use others (job-seeking exemptions, early retirement, women at home, etc.).
The French context and overview of current approaches to leaving the labour market
The French pension system is complex, with equality in the length of the required contribution period for private sector employees and civil servants (in 2008), but at the same time a great variety of rules governing access to pensions, and no private pension insurance. These are the specific features of the French system. The legal age of retirement for employees is still very low (the same for men and women, namely 60 years), and the pension system is a pay-as-you-go only. Moreover, the employment rate for 55–64 year olds was 40.7% in 2005, one of the lowest in Europe (OECD, 2006). Length of employment is being squeezed from two sides: age of entrance in the labour market is rising (23 years old) and, at 59, the average age at cessation of employment is decreasing (differing from the average age of 62 when rights are accrued). Thus, the French labour market essentially concerns the 25–55-year-old population, and a new phase of transition (non-working, preretirement, unemployment, etc.) appears between employment and retirement, classic periods in the life cycle.
French employees have several options when leaving the labour market: early retirement, disability pensions and job-seeking exemptions for different circumstances. State early retirement pensions have decreased since 1998. Following Law 2003-775 of 21 August 2003 on retirement reform, state mechanisms for early retirement have gradually decreased, and taxation of those retiring early from the private sector has steadily increased (from 12% in 2003 to 22% in 2008). This gradual reduction in those taking “classic” early retirement has favoured those measures that aimed to compensate for occupational health risks (CATS and CAATA: see footnote no. 1). Hence, at the end of 2005, the only classic early retirement schemes financed concern only 55,000 recipients compared to more than 70,000 persons in health schemes [25]. Together with this change in early retirement, job-seeking exemptions became the most common means of early retirement from the labour market in France. This mechanism, created in 1986, was initially designed to help people more than 55 for whom it was difficult to find work. It is now used by all persons aged at least 57 and a half, or those over 55 provided that they have at least 160 trimesters of contributions to basic compulsory old age insurance schemes (or equivalent periods) or are covered by another specific scheme. Job-seeking exemptions increased by about 50% between 1996 and 2006 and stood at 383,000 in December 2007. However the number of recipients has fallen since December 2006 (peaking at over 416,000).
Which mechanisms for early retirement are aimed at unhealthy people, amongst the range of those available? Persons with a permanent disability, for reasons of health or a handicap, receive either a replacement income in proportion to their final salary (disability pensions) or a minimum social benefit (Handicapped Adult Benefit). Disability pensions are more often awarded for age-related health problems. In France, disability pensions (in the public and private sector) are the principle mechanism for early retirement for health reasons. These pensions are awarded where there is a reduction in earning capacity of at least two-thirds as assessed by a doctor appointed by the Primary Sickness Insurance Scheme. At the end of 2004, 750,000 persons aged over 50 had received either a disability pension or Handicapped Adult Benefit [5]. Among these recipients, at least 650,000 persons are almost certainly not working (apart from those with category 1 pensions for persons deemed capable of paid employment). If we compare recipients of disability pensions in Germany, Sweden, the UK and France, the number of disability pension claimants is lower in France for all ages. For example, between the age of 55 and 59, 6% of men receive disability pensions in France, compared to 10% in Germany, 15% in the UK and more than 20% in Sweden. This relatively low recourse of disability pensions in France could be due to the existence of better financial benefits available from other mechanisms. The replacement rate offered by disability pensions (less than 50% in the absence of supplementary insurance) is often below the replacement rate offered to workers retiring at term (between 65 and 75%). An unhealthy employee may also benefit from a better replacement rate in early retirement, or after redundancy, than from a disability pension. An occupational doctor can award pensions for inability to work after verifying that the employee is not fit for the nature of job. This applied to about 60,000 persons in 2005 and may result in redundancy where reclassification is not possible [2].
Finally, the introduction in July 2004 of the “lengthy careers” mechanism makes it possible for persons to retire before 60 if they started work before the age of 17 and contributed during five trimesters before their 16th birthday (for retirement at 56, 57 or 58) or their 17th birthday for those retiring at 59. This early retirement mechanism may compensate, indirectly, for the arduousness of the work in these categories of under-skilled workers who enter the labour market very young.
The relationship between health and occupational statuses: an overview from the literature
In France the decision to cease professional activity mainly depends at the macroeconomic level on institutional rules governing access to retirement and at the microeconomic level on the financial constraints, which involve the capacity to take a reduction in pension that until 2003 was substantial for the private sector in the base scheme. So institutional and financial constraints often mean that those with low incomes have to wait until the legal retirement age before acquiring their retirement benefits [6].
Nevertheless, according to the literature, health status appears to be one of the most important determinants of labour market participation by older workers [23]. The relationship between health and employment is theoretically clear [30], but is the result of a double causality that is empirically ambiguous [13]. Many empirical studies have shown the healthy worker effect. Hence, bad health status results in early retirement from the labour market [9, 10, 16, 19]. In addition, the effect of the arduousness of work on health status shows that work can also affect health status, which complicates the simultaneous study of health and labour market participation [11, 21]. Thirty-six percent of employees aged between 50 and 59 reporting a condition that limits their work ability state that their health problems result from their working environment [12]. Furthermore, according to the results of the SUMER survey (DARES, 2006), 28% of persons over 50 have joint or postural problems. This second connection, which we do not address in this paper, has also been studied empirically, given that working conditions may affect health status [22, 29].
Rust et al. [28] have shown that many unhealthy workers stop working at 62 (the age at which they can claim their pension entitlement in the USA), while healthy workers retire later at around 65 years of age. In general, workers in the poorer socioeconomic classes, that is, the unhealthier ones, retire soonest (Burtless and Moffit 1984). In France, studies of the ESTEV survey cohorts have shown that poor health status greatly increases the risk of exclusion from employment [15, 17]. In addition, we have shown, on the basis of a complementary survey of the INSEE (National Institute of Statistics and Economic Studies) employment survey of 1996, that poor health results in early departure from employment, after taking financial and family constraints into account [3]. The healthy worker effect appears to be in line with the workers’ wishes, given that they hope to retire early if they suffer from health problems [27]. Furthermore, even if the role of health status seems to be the most important at the end of working life, this relationship is observed from the beginning of working life [31].
Various sources of biases may affect the quality of measurement of this double causality between health and employment statuses: a reporting bias related to how information is collected, a bias in the measurement of health status and an incentive and justification bias.
First of all, a reporting bias is inherent in this exercise. Individual declarations, which are available from most health surveys, are dependent on social characteristics and even on individual health status, which can result in sociocultural and endogenous bias [1, 8]. Hence, some authors combine objective measures (such as mortality) with subjective measures of health status. The difficulty in measuring the “real” health status of individuals results in a second form of bias. Added to the difficulty of measuring real morbidity is that of the relevance of the indicator chosen to measure the specific link between health and employment statuses. The most natural indicator to measure this would appear to be disability, often presented in surveys in terms of activity limitations. But this indicator addresses only one aspect of health status, such that several indicators of health should be used to measure their impact on employment and to take into account the multidimensional nature of health status [24].
Furthermore, studying people aged over 50 complicates the analysis because older persons are subject to severe barriers in the labour market and can leave employment to take advantage of the system of early retirement and disability pensions with more advantageous replacement rates than in retirement. This can be termed an incentive bias, which is not necessarily related to health status. These barriers also underline the problem of the “employability” of older persons. Lastly, there may be a justification bias whereby people explain their departure from the labour market in terms of a health problem rather than redundancy, which may overestimate the correlation between health and work.
In an attempt to correct the sources of bias described above, Bound et al. [8] and then Campolieti [10] considered activity limitations as a latent variable, dependent on a group of individual factors and on health status. Based on this model, Barnay and Debrand [4] have shown that reporting an activity limitation leads to a more significant reduction in employment among persons aged 50–64 in Europe (based on SHARE data) after controlling for endogenous bias and the measurement of health, because activity limitations are taken into account directly (by accounting for the variables of age, marital status, country of residence, educational qualifications and other tools for measuring health status, as well as medical conditions and body mass index).
The links between health status and unemployment are also complex, with a similar problem of double causality affecting the relationship. Khlat et al. [20] carried out a literature review of the health–unemployment link, showing in particular the direct effect of health on unemployment and the causal effect of unemployment on health. Sarel-Cubizolles et al. [17] have shown, based on data from the ESTEV survey (the Health, Work and Ageing Survey), that degradation in health status (such as blood pressure, restricted physical mobility, etc.) can increase the risk of losing one’s job [15]. Elsewhere, Mesrine [26] has shown that the annual risk of death for an unemployed male is three times higher than that of an employed male of the same age.
Measuring the relationship between health and employment statuses between the age of 50 and 59
Data
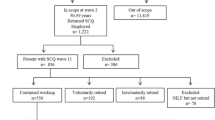
The decennial health survey (EDS) was established by INSEE in 1960 and since then has been repeated every 10 years (1969–1970, 1980–1981, 1991–1992, 2002–2003). The objectives of the EDS are to measure the health status of ordinary households, to estimate the annual use of medical and preventive care, and to investigate the association of health and use of medical care with individual and household characteristics. This survey, carried out for a representative sample of ordinary households, selected at random from census data, enables the use of medical care and the health status of individuals to be identified and measured for a period of 2 months. This study relates to people aged between 50 and 59, namely 7.4 million individuals. We have reconstructed, or at least approximated, the administrative categories described above, particularly for recipients of disability pensions (non-working people reporting official recognition of a handicap) and those with job-seeking exemptions (unemployed people not seeking work). We looked specifically at the categories of working, non-working and unemployment. In addition, the health data used relate particularly to perceived health, activity limitations during the previous 6 months and the prevalence of chronic illness (see Box 1).
Methodology
We worked with two types of logistic regression. The first investigated the relationship between health and working status in order to validate the healthy worker effect (binomial logit). The second aimed to analyse the correlation between health and non-working status (multinomial logit) in order to show that some unhealthy people use mechanisms at the end of their working life that do not involve compensation for poor health status.
We may expect that an unhealthy worker makes several choices rather than a single decision. For example, an advisory doctor determines whether a disability pension will be awarded, and early retirement from a business is determined by professional logic. The retiring employee has several possibilities, particularly after the age of 55.
Using a simple logit binomial model, we begin by explaining the probability of working between 50 and 59 (Table 2) and the probability of non-working with no officially declared recognised handicap between 50 and 59 (Table 4), all other things being equal.
The probability of working will depend on the explanatory variables and on self-reported health status indicators (activity limitations, perceived health, chronic illness, abnormal body mass index and feelings of depression), age (which links to eligibility for particular mechanisms), marital status (living with a partner or not), age at the end of education but also on the career path (career interruptions for unemployment or ill health reasons, changes of occupation for health reasons) and the type of work done or having been done, in order to account for the characteristics of the working environment.
Next, among the non-working population we analyse the correlations between health and non-working statuses for people aged 50–59 using a non-ordered multinomial model (Table 6).
The dependent variable can have various statuses, which are constructed from survey answers:
-
Unemployed not seeking work (reference situation allowing approaching the administrative category of job-seeking exemptions).
-
Unemployed seeking work.
-
Non-working with declared official recognition of handicap. (This category captures a large part of the bonds between poor health and non-working statuses; then we decide to take off the regression.)
-
Non-working without declared official recognition of handicap.
-
Retired or early retired.
Results
Descriptive statistics
Self-reported health varies widely by employment status. In the 50–59-year-old population, about 11% of workers report activity limitations compared to 17% in the population aged 50–59 years. In the non-working population, people with a recognised handicap report the poorest health status, whichever health indicator is used, followed by non-worked people with no recognised handicap, in each case for men. Big differences in reported health for non-worked men and women result from career paths, choices and particular behaviours. Furthermore, whether or not an unemployed person is looking for work is also very discriminating, with unemployed workers looking for work always reporting better health than those who are not seeking work (Table 1).
The relationship between poor health and employment statuses
The analysis “all other things being equal” confirms the negative correlation between reported health status and labour market participation (Table 2). The stratification proposed by type depends on three models. Neverthess, except for model C, it is not possible to study causality. Model A aims to estimate the working probability with the introduction of four tools for measuring health status: perceived health status, chronic illnesses, abnormal BMI and activity limitation.Footnote 2 The presence of different health status variables allows limiting self-reporting biases. Model B only considers activity limitation, which in fact is the only variable with which the link between health and physical aptitude for work can be measured. Finally, the third (C) introduces information concerning the nature of the professional career (career breaks) into model B. Thanks to this information, this model enables us to assess a possible causal link between professional career interruptions (in particular those for health reasons) and current employment status—because it is possible to establish a chronology of events, the selection effect of health on the labour market can be studied. Information about professional careers in fact selects a population that has already worked, which is not the case for the whole sample and for women in particular. The associated coefficients are at risk of selection bias, which is why, for model C only, individuals who have never worked are excluded from the analysis.
By its nature, health status does not affect the employment rate in men and women in the same way. For men, poor perceived health and activity limitation will each have their own negative effect on the probability of working. However, in women, the prevalence of chronic illness, activity limitation and an abnormal BMI will considerably reduce their presence in the labour market. The relative probability of working decreases very significantly, by 68% for men and by 51% for women, after controlling for perceived health, chronic illness and BMI. When only activity limitations are introduced to measure health status (model B), this probability decreases by 74% for men and by 59% for women compared to men (or women) who do not declare any activity limitations. This difference between models A and B results from the importance of the pure effect of activity limitations on the link between health and employment, compared to other health variables. Results show that the correlation between health status indicators is not so high and corresponds to different aspects to health. The change in health status measured using the other indicators does not highlight this health–employment correlation, or at least very little, and is less significant. However, it results from different health characteristics depending on the type.
Career interruptions that the surveys explain in terms of health problems result in a reduced probability of working between 50 and 59 of 41% at the 0.1% threshold (model C). The preponderance of professional characteristics in the male model confirms an earlier study [5]. These results also seem to show that health-related events during professional life affect departure from the labour market and socioeconomic status [18]. However, a man who reports having changed jobs for health reasons is 63% more likely to be employed at the end of his working life than a man who does not report this. Although the level of significance is not high, we may nonetheless assume that changing professional activity due to health problems has a protective effect for male older workers in the labour force. In this case, adapting jobs or even changing work during working life would appear to be one approach to integrating and keeping sick or handicapped people in the labour market (in Centres for Assistance at Work, in Protected Workshops or in Centres for the Distribution of Home Working, for example).
The other socioeconomic variables have a predictable impact on employment. Employment between 50 and 59 years old is strongly influenced by age-related measures and principally those giving access to early retirement mechanisms. Hence, the relative probability of working decreases significantly from 55 years of age. At 55, compared to a 50 year old, this decreases by 45% for men and by 55% for women, all other things being equal.
Level of qualifications, measured here with the variable age at completion of education, also has an impact on working, particularly for women who leave education below 15 years of age (70% less than for women who finish their studies after the age of 20). However, the level of education has less effect on the employment of women over 50 because other events intervene during their professional lives.
The effect of marital status on participation in the labour market is different for men and women. It seems to have a protective effect in men living with a partner, because the probability of working for a single man is between 35 and 40% less than for a married man, all other things being equal. In contrast, women who live alone are undoubtedly more likely to participate in the labour market for financial reasons. (A single woman is 70–75% more likely to work compared to a married woman.)
Finally, I introduce a variable of occupational sectors to compare employment behaviours in the private sector, for civil servants and self-employed. At the end of a professional career, we know that professional constraints and conditions of retirement are not similar for these different categories. Differences between occupational sectors mean that we can approximate the effect of “labour demand”, with self-employed workers stopping work later, no doubt because of their less generous retirement system and job specificities. However, there is no significant difference between private sector employees and civil servants (except for Model C for men). Health status at the time of the survey as well as health-related events during the professional career seem to have some effect on the employment rate for 50–59 year olds for men in particular, although the effects appears to be relatively independent (the coefficient associated with activity limitations does not vary significantly whether or not career events are taken into account). These initial results confirm the very strong relationship between deteriorating health status and departure from the labour market.
As we have seen, unhealthy people can retire early from the labour market using disability pensions (in the category non-working with recognised handicap) and possibly also using the job-seeking exemption mechanism (which is partly in the category unemployed not seeking work). So now it will be instructive to look in more detail at reported health status among the non-working population in particular.
The relationship between poor health and non-working statuses
We may study the causal link between health and non-working statuses amongst persons who have worked directly using the decennial health survey. Non-working status refers to different situations for men and women: people looking after the home and those with disability pensions in particular. Amongst persons aged between 50 and 59 who report they look after the home, 99% are women. Non-working is caused by a health problem for 41% of the non-working population (90% for men and 27% for women). Non-working for health reasons is, as we would expect, very strongly related to recognition of a handicap. Health reasons do not explain why women older than 50 become non-workers (only 9% explain it with health reasons). Even among women looking after the home with an officially recognised handicap or disability, only 42% explain their non-working state by health reasons.
In contrast, health status is strongly correlated with non-working with recognised handicap status for men and women (respectively 99 and 94%). They are all classed as “other non-working”, i.e., they could potentially benefit from disability pensions. Even among “other non-working” men without a recognised handicap, 82% report a link between non-working and health statuses (Table 3).
If the relationship between poor health status and non-working with declared official recognition of a handicap is obvious, it is nevertheless interesting to look at the link between health status and non-working without declared official recognition of a handicap for the population that has left employment. To test this relationship, we use a simple (binomial) logistic regression based on models B and C (Table 4). The male model lacks statistical power (3% of the sample of men), and de facto very few variables emerge from the analysis.
However, reporting of activity limitations appears to be very closely related to this status because the relative risk of non-working without a recognised handicap is almost three times higher where activity limitations are reported. In order to control for a possible effect of other health problems in reporting activity limitations, we carry out two other regressions (only the coefficient associated with activity limitations is presented), one controlling for general health variables (perceived health and the prevalence of chronic illness) and the other for variables likely to be associated more specifically with social exclusion (BMI and depression). These complementary analyses show that it is not activity limitations that explain the link between health and occupational status for men, but the indicator of perceived health. A non-working man declaring poor health is in fact four times more likely to be non-working without a recognised handicap. Hence, this status is not explicitly related to a declared handicap, but rather to men’s general perception of their health status, excluding depression (which does not emerge from the analysis).
On the contrary, in the female population, there is an opposite correlation between health and non-working statuses, with relatively fewer women reporting activity limitations than for the other categories. In contrast, this status is strongly linked to the level of education, the relative risk of non-working with no recognised handicap being two times greater when the age on leaving education is below 15 years compared to women who complete their studies after age 20. Marital status is completely determinant, with married or widowed women more often non-working for non-health reasons compared to single women. If we look at events during the professional career, we see different career paths for men and women no longer working after age 50. For men, periods of unemployment during the professional career seem to lead to non-working with no recognised handicap after 50, while women who have experienced career interruptions following unemployment or illness periods are significantly less likely to become non-workers with no recognised handicap. The latter again underlines the disconnection between poor health and non-working statuses with no recognised handicap in the female population.
Poor health and approaches to leaving employment
Non-working as a means of leaving employment for persons in poor health appears to be logical, particularly for persons whose handicap is officially recognised. What role could unemployment mechanisms play for these people? Given the difficulty in measuring the number of people with job-seeking exemptions (see Box 2), we concentrate our analysis on the 50–59-year-old non-working population, because those over 55 years old are eligible for job seeking exemptions under certain conditions, and those over 57 years old are in all cases.
One quarter of non-working 55–59 year olds who have worked report activity limitations, with this proportion increasing from 13.2% for retired and early retired to 70.9% for non-workers with a recognised handicap. In addition, unemployed persons not seeking work report twice as many activity limitations as those who are seeking work (see Table 5).
To understand the relationship between different types of work available to persons over 55 and health status, we have used a multinomial model to look at unemployed persons not seeking work (see Table 6).
The multinomial model is one of discrete choice between a given number of ways of leaving employment under the hypothesis that they are mutually exclusive. To simplify the analysis and in view of the small sample sizes, the dependent variable is constructed using a non-ordered polytomic approach with four modalities: unemployed seeking work, unemployed not seeking work, non-working with no recognised handicap and a final group of retired and early retired. The last category groups people in different situations, but the small sample size rules out a more detailed analysis and makes it necessary to retain this category.
Persons who report activity limitations are less likely to have another employment status after 55 and more likely to have job-seeking exemptions even after controlling for perceived health and chronic illness.
All other things being equal, an unemployed person who reports an activity limitation is 66% less likely to be seeking work (column 1). Furthermore, a person with poor functional health is more likely to leave the labour market using the job-seeking exemption system than the preretirement and early retirement system [associated risk of 70% (column 3)]. Early retirement results from collective redundancy; a priori it is less likely to select individuals based on their health status. On the contrary, an individual suffering from a health problem will have more reason to obtain an individual redundancy that could later lead to a job-seeking exemption.
The choice between non-working without a recognised handicap and job-seeking exemptions is less clear (column 2). If education level and career path are explicitly accounted for, the statistically shown differences between unemployed persons not seeking work and non-working persons with no recognised handicap disappear. The early exclusion from the labour market of a population with a low education level explains the emergence of a group of non-working persons in poor health at the end of working life who do not benefit from any mechanisms. These are essentially men because the non-working female population with no recognised handicap is in relatively good health.
The difference between sexes perhaps explains the non-significance of activity limitation in this regression.
Career breaks for health reasons however capture all the health information. This finding is not straightforward to interpret: a career break for health reasons would be more likely to lead to job-seeking exemptions than a non-working situation, without recognition of a handicap after controlling for activity limitations. The activity limitation variable perhaps represents a fairly severe handicap: people who face less severe health problems during their professional career may be more inclined to apply for job-seeking exemptions in order to obtain a better replacement rate, knowing that they are ineligible for a disability pension.
Within this population, the fact that we technically needed to group together men and women to carry out this analysis hides some big differences, as the coefficient associated with this variable suggests, and which indicates the need for further analysis.
The increase with age in the numbers of persons with job-seeking exemptions emerges clearly if we test for the probability of being non-working with no recognised handicap and early retired or retired. Given the specificity of this mechanism, civil servants and self-employed persons use it very little, hence the importance of the odds ratios associated in particular with civil servant status.
The population studied here is no longer working between the age of 55 and 59, but has worked in the past. Hence, this population has already been selected: it is a population with poorer health status and is less educated than the employed population of the same age. Where there have been career breaks for health reasons, this is very likely to result in unemployment without seeking work between the age of 55 and 59, rather than non-working with no recognised handicap, which is not the case for career breaks due to unemployment.
Discussion and conclusion
In France, the decreasing age of retirement, the persistence of early retirement and of job-seeking exemptions until July 2008 would all appear to enable employees with poor health to leave the labour market early. In the Scandinavian countries, such as Sweden, it is essentially generous disability mechanisms that meet this need. The increasing number of job-seeking exemptions in France prompted us to ask what role they could play in early departure from the labour market for persons in poor health, those generations born between 1932 and 1936 for the most part having had access to job-seeking exemptions before retiring [7].
It is important to note that the survey data used do not include all job-seeking exemption data, for which 400,000 persons were eligible at the time of the survey. The survey data are subject to reporting bias but are also incomplete—the survey is of households, and hospitals and institutions are not included. It is also the case that possession of a job-seeking exemption does not necessarily mean the recipient is not seeking work. On the other hand, it is likely that people with a job-seeking exemption are not likely to be looking for work, particularly those above the age of 57.
Another source of bias concerns reported health status, which we have tried to account for with various regressions and with different health variables. Despite this bias, the results suggest a relationship between departure from the labour market and poor health, even if we cannot prove a causal link.
Functional limitation of daily activities is more likely to result in exclusion of over 50 year olds from the labour market. Men reporting poor health are less inclined to work in contrast to women with a chronic illness or an abnormal BMI, who are subject to early exclusion from the labour market. Research on recruitment discrimination could no doubt throw light on these questions.
The relationship between health and non-working statuses is quite different for those with or without a recognised handicap. Official recognition of disability affects a population much less able to work. The reasons linked to a non-working state given by women looking after the home seem to be less closely related to health status than for men.
These results seem to indicate that a proportion of 55–59 year olds with disabilities are unemployed and not seeking work, and may therefore have job-seeking exemptions. This would appear to support the hypothesis that a proportion of people with job-seeking exemptions are unhealthy.
Unemployment benefits decrease with the suppression of job-seeking exemptions. Some unhealthy people aged between 55 and 59 will receive a disability pension. This raises the issue of the role of different branches of social security in protecting health risks at the end of working life. This possible substitution between disability and unemployment mechanisms, which is taking place in some other countries when one of the two mechanisms is considered less beneficial, partly reduces the effectiveness of policies to delay retirement age. On the other hand, abolishing job-seeking exemptions might mean that people whose state of health does not warrant a disability pension shift to other mechanisms involving daily allowances or that the population of sick people who are not covered at the end of their working lives simply adds to the non-working population with no recognised handicap.
Hence, we need to deal with the problem of disability at the end of people’s working lives, but we must also assess the trade off that people make between disposable income, given lower benefits, and health status, which people need to be able to measure. The type of health problem (occupational or otherwise), the age at which it appears, and also the employer’s situation when the health problem arises will all affect the mechanisms available and hence the replacement rate that is proposed.
Notes
Two modes exist (CATS and CAATA in French). The first one allows employees who are 55 or older and are having difficulties adapting to new technologies or who during their professional career had to do hard work to stop their professional activity before 60 years. The second one allows asbestos workers to stop working at 57 years.
Given the very specific nature of depression, it has not been included here.
References
Anderson, K.H., Burkhauser, R.V.: The importance of the measure of health in empirical estimates of the labour supply of older men. Econ. Lett. 16, 375–380 (1984)
Bardot, F., Touranchet, A.: Partir plus tôt: le dilemme pour les médecins du travail. Retraite et Société, 49, 62–77 (2006)
Barnay, T.: Santé déclarée et cessation d’activité. Revue Française d’Économie 20(2), 73–106 (2005)
Barnay, T., Debrand, T.: Effects of health on the labour force participation of older persons in Europe, Issues in health economics IRDES no. 109 (2006)
Barnay, T., Jeger, F.: Quels dispositifs de cessation d’activité pour les personnes en mauvaise santé? Irdes, Questions d’Économie de la Santé, no. 108 (2006)
Blanchet, D., Mahieu, R.: Une analyse microéconométrique des comportements de retrait d’activité, pp. 9–31. Revue d’Économie politique. Numéro hors-série, Épargne et Retraite (2000)
Bommier, A., Magnac, T., Roger, M.: Le marché du travail à l’approche de la retraite: évolutions en France entre 1982 and 1999. Revue Française d’Économie 18(1), 23–82 (2003)
Bound, J.: Self-reported versus objective measures of health in retirement models. J. Hum. Res. 26, 106–138 (1991)
Bound, J., Schoenbaum, M., Stinebrickner, T.-R., Waidmann, T.: The dynamic effects of health on the labor force transitions of older workers. Labour Econ. 6(2), 179–202 (1999)
Campolieti, M.: Disability and the labor force participation of older men in Canada. Labour Econ. 6, 405–432 (2002)
Volkoff, S., Molinié, S., Jolivet, A.: Efficaces à tout âge, Dossier no. 16, Centre d’Études sur l’Emploi, PUF, p. 126 (2000)
Coutrot, T., Waltisperger, D.: L’emploi des seniors souvent fragilisé par des problèmes de santé, Premières informations et premières synthèses, no. 08.1, p. 4 (2005)
Currie, J., Madrian, B.C.: Health, health insurance and the labor market. In: Ashenfelter, O., Card, D. (eds.) Handbook of Labor Economics, pp. 3309–3416. North Holland, Amsterdam (1999)
Dahl, S.-A.N., Oivind, A., Vaage, K.: Work or retirement? Exit routes for Norwegian elderly. Appl. Econ. 32(14), 1865–1876 (2000)
Deriennic, F., Saurel-Cubizolles, M.J., Monfort, C.: Santé, conditions de travail et cessation d’activité des salariés âgés, Travail et Emploi, no. 96 (2003)
Dwyer, D.S., Mitchell, O.S.: Health problems as determinants of retirement: are self-rated measures endogenous? J. Health Econ. 18(2), 173–193 (1999)
Saurel-Cubizolles, M.J. et al.: État de santé perçu et perte d’emploi. In: Cassou, B. (ed.) Travail-Santé-Vieillissement: Relation et Évolution, Edition Octares (2001)
Jusot, F., Khlat, M., Rochereau, T., Sermet, S.: Une mauvaise santé augmente fortement les risques de perte d’emploi, Données Sociales–La Société française, pp. 533–542. Paris, Insee (2006)
Kerkhofs, M., Lindeboom, M., Theeuwes, J.: Retirement, financial incentives and health. Labour Econ. 6, 203–227 (1999)
Khlat, M., Sermet, C.: La santé des chômeurs en France: revue de la littérature. Revue d’Épidémiologie et de Santé publique 52(3), 465–474 (2004)
Lasfargues, G.: Départs en retraite et travaux pénibles. L’usage des connaissances scientifiques sur le travail et ses risques à long terme pour la santé, Rapport de recherches, no. 19, Centre d’études de l’emploi, p. 39 (2005)
Leung, S.F., Wong, C.T.: Health status and labor supply: interrelationship and determinants, mimeo. Honk-Kong University, Honk-Kong (2002)
Lindeboom, M.: Health and work of older workers. In: Jones, A.M. (ed.) Elgar Companion to Health Economics. Edward Elgar, Cheltenham (2006)
Loprest, P., Kalman, R., Sandell, S.H.: Gender, disabilities, and employment in the health and retirement study. J. Hum. Res. 30(5), S293–S318 (1995)
Merlier, R.: Les dispositifs de préretraites publiques en 2005: poursuite du repli, Premières informations premières synthèses, Dares, no. 52-1, décembre, p. 7 (2006)
Mesrine, A.: La surmortalité des chômeurs: un effet catalyseur du chômage? Économie et statistique, Insee, no. 334, pp. 33–48 (2000)
Rapoport, B.: Âge de départ souhaité, âge de départ prévu et liberté de choix en matière d’âge de départ à la retraite, Drees, Dossiers Solidarité et Santé, Perspectives et comportements en matière de retraite, no. 3, pp. 31–50 (2006)
Rust, J., Phelan, C.: How social security and medicare affect retirement behavior in a world of incomplete markets. Econometrica 65(4), 781–831 (1997)
Stern, S.: Measuring the effects of disability on labor force participation. J. Hum. Res. 24, 361–395 (1989)
Strauss, J., Thomas, D.: Health, nutrition and economic development. J. Econ. Lit. 35, 766–817 (1998)
Tessier, P., Wolff, F.C.: Offre de travail et santé en France, Économie et Prévision, no. 168, pp. 17–41 (2005)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Barnay, T. In which ways do unhealthy people older than 50 exit the labour market in France?. Eur J Health Econ 11, 127–140 (2010). https://doi.org/10.1007/s10198-009-0155-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10198-009-0155-4