
Abstract
Background
Tolvaptan is an effective treatment for polycystic kidney disease (PKD), but also causes unfortunate polyuria. Hydrochlorothiazide (HCTZ) has been shown to reduce urine volume in nephrogenic diabetes insipidus, raising the possibility that HCTZ could also be effective in reducing tolvaptan-induced polyuria. In this study, we examined the combined administration of HCTZ and tolvaptan.
Methods
Male PCK rats were divided into four groups of normal chow (Cont), normal chow plus tolvaptan, gavage HCTZ treatment, and tolvaptan + HCTZ. Biochemical examinations of the plasma and urine were performed as well as histological and molecular (mRNA and protein expression) analyses.
Results
Groups treated with tolvaptan had significantly higher 24 h urine excretion, which was significantly reduced in the tolvaptan + HCTZ group after 2 weeks. Cyst size, pERK protein expression, and Cyclin D1 mRNA expression were all significantly reduced in both the tolvaptan and tolvaptan + HCTZ groups, indicating that HCTZ did not affect the beneficial functions of tolvaptan. Notably, aquaporin 2 redistribution from the apical to intracellular domains was observed in tolvaptan-treated rats and was partially reversed in the tolvaptan + HCTZ group. The renal glomerular filtration rate was reduced in the tolvaptan + HCTZ group. Significantly lowered mRNA expression of neuronal nitric oxide synthase, prostaglandin E synthase 2 and renin were also found in the medulla, but not in the cortex.
Conclusion
HCTZ reduces tolvaptan-induced polyuria without altering its beneficial effects on PKD. This novel therapeutic combination could potentially lead to better PKD treatments and improved quality of life for the affected patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
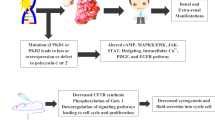
Polycystic kidney disease (PKD) is the most common genetic renal disorder, affecting 12.5 million people worldwide [1]. Structurally, PKD is characterized by altered renal tubules that develop multiple cysts within the kidney, crushing adjacent normal tubules and eventually rendering them non-functional. Autosomal dominant PKD (ADPKD) is the leading genetic cause of end-stage renal disease (ESRD) [2], accounting for about 5–10% of all ESRD patients requiring renal replacement therapy in Europe and the USA [3, 4]. Thus, continued research to understand disease pathogenesis is essential.
The PCK rat strain is an established model of PKD and is characterized by progressive cystogenesis, impairment of renal function, intrarenal accumulation of cAMP, abnormal activation of adenylyl cyclase, and ERK signaling [5]. It resembles many clinical and morphological aspects of human ADPKD, although the pattern of inheritance is autosomal recessive [5]. The establishment of this strain has greatly enhanced our understanding of PKD, and has enabled various treatments to be analyzed in vivo.
Tolvaptan, a vasopressin V2 receptor antagonist, is frequently used in ADPKD patients, and has renoprotective effects by reducing the increase in kidney volume [6]. However, this treatment also causes polyuria, which can be severe and, in some cases, result in a urine output up to 8–10 L per day [7]. This aquaretic effect cannot be ignored and has a profoundly negative impact on the quality of life for the patient. Indeed, patients are usually required to void more frequently, resulting in increased pressure in the upper urinary tract as well as an increased risk of ureter dilatation, hydronephrosis, and ultimately renal function loss. This rapid decline from polyuria to renal function loss is well-documented in patients with diabetes insipidus and psychogenic polydipsia [8,9,10,11]. Thus, the side effects of tolvaptan limit its utility, and the development of other treatment options is required.
Hydrochlorothiazide (HCTZ) is the mainstay drug prescribed for diabetes insipidus and is effective in reducing polyuria and increasing urine osmolality in both central and nephrogenic diabetes insipidus [12,13,14]. Polyuria following tolvaptan treatment in PKD follows the same mechanism as that described for nephrogenic diabetes insipidus, whereby the V2 receptor no longer responds to circulating vasopressin. However, the effectiveness of HCTZ in reducing tolvaptan-induced polyuria during PKD treatment has not been evaluated.
In this study, we investigated the effects of combination treatment using HCTZ and tolvaptan on PCK rats. We also sought to elucidate any HCTZ-mediated changes in the therapeutic effect of tolvaptan, and to identify its antidiuretic mechanism. To our knowledge, this is the first time evaluating HCTZ and tolvaptan as a combination therapy for PKD.
Materials and methods
Animal experiments
PCK rats start cystic formation in kidneys as early as 1–3 weeks of age [5], and most studies using this model performed them around 10 weeks old as an adult model. However, to study early cyst formation, male PCK rats (n = 42; Charles River Laboratories) aged 5–7 weeks old were used in this study. They were divided into four groups and monitored for the entire 8-week experimental period (Fig. 1). Untreated PCK rats served as the Cont group, which were fed a standard protein diet (n = 10); the Tol group had tolvaptan incorporated into their normal rat chow at 0.05% (Otsuka Pharmaceutical, Tokyo, Japan) (n = 10); the HCTZ group was treated with HCTZ (80 mg/kg/day; Sigma-Aldrich, St. Louis, MO, USA) through gavage, starting from the second week (n = 10); and the Tol + HCTZ group were treated with both tolvaptan and HCTZ (n = 12). Rats were allowed food (treated and untreated) and tap water ad libitum and kept at a constant temperature and humidity in a 12:12 h dark–light cycle.

Experimental design. PCK rats were divided into four groups: Cont group, untreated PCK rats (n = 10); Tol group, which had tolvaptan incorporated into their normal rat chow at 0.05% (n = 10); HCTZ group, which was treated with hydrochlorothiazide (80 mg/kg/day) through gavage starting from the second week (n = 10); and the Tol + HCTZ group, which was treated with both tolvaptan and HCTZ as described (n = 12)
Tolvaptan incorporated into the chow was a gift from Otsuka Pharmaceutical. The tolvaptan concentration, 0.05%, in this study was half, when compared to previous report that demonstrated the protective effect of tolvaptan on polycystic kidney disease development in the PCK rat [15]. A preliminary study was performed to test a dose–response of HCTZ. The low dose (10 mg/kg/day by gavage) was calculated from human dose [16] and dose conversion equation between animals and human [17]. The high dose (80 mg/kg/day by gavage) was determined by the previous report [18]. Since the efficiency of the low dose for urine reduction was weak (less than 10% reduction) and not statistically significant, we decided to use high dose in this study.
During the follow-up period, 24 h urine collection in metabolic cages was performed every week to evaluate urinary output and excretion composition. Tail-cuff blood pressure was also obtained every week, because HCTZ is representative of anti-hypertensive diuretics. At the end of the observation period, rats were sacrificed by guillotine, and blood was obtained from the exposed carotid artery. Both kidneys were weighed and immediately sliced. The samples for histological analysis were fixed with 10% formalin (Mildform, Wako Pure Chemical Industries, Osaka, Japan) and embedded in paraffin. The samples for gene expression analysis were dissected to isolate the cortex and outer medulla, snap frozen in liquid nitrogen, and stored at − 80 °C. Biochemical examinations of the plasma and urine were performed by Nagahama Life Science Laboratory (Nagahama, Japan).
Quantitative real-time PCR
Total RNA was extracted using Trizol (Invitrogen, Carlsbad, CA) and treated with DNase I (Invitrogen). cDNAs were generated using SuperScript III First-strand Synthesis SuperMix (Life Technologies, Carlsbad, CA, USA). Quantitative real-time PCR (qRT-PCR) was performed with 5 ng of cDNA, using SYBR Premix Ex Taq II reagent (TaKaRa, Shiga, Japan) and a CFX96 Real-Time PCR Detection System (Bio-Rad Laboratories, Hercules, CA, USA). Gene-specific primers for aquaporin (Aqp2), cyclin D1 (Ccnd1), microsomal prostaglandin E synthase 2 (Ptges2), neuronal nitric oxide synthase (Nos1), renin (Ren), and ribosomal protein large protein 2 (Rplp2) were purchased from TaKaRa. mRNA expression was normalized to that of Rplp2. All qRT-PCR were run with melting curve analysis to check non-specific amplification of PCR products and primer dimers.
Immunostaining analysis
Paraffin-embedded kidneys were sliced (2.0 µm thick) for immunohistochemical and Masson’s trichrome staining. The sections were deparaffinized with xylene and dehydrated with ethanol. Antigens were retrieved by microwaving for 5 min in 10 mM citrate buffer (pH 6.0). After blocking with Protein Block Serum-Free reagent (X0909, Dako, Glostrup, Denmark), the sections were incubated in primary antibody overnight at 4 °C. Anti-phosphorylated extracellular signal-regulated kinase (pERK)1/2 (1:300, M8159, Sigma-Aldrich), anti-kidney injury molecule (Kim)1 (1:1250, AF3689, R&D Systems Minneapolis, MN), and anti-Aqp2 (1:3000, A7310, Sigma-Aldrich) were used as primary antibodies. After washing with phosphate-buffered saline (PBS) containing 0.03% tween-20, sections were reacted with Histofine Simple Stain MAX PO (Nichirei, Tokyo, Japan) or fluorescent labeled secondary antibodies (Alexa Fluor 488 and Alexa Fluor 555, 1:1000, Molecular probes, Eugene, OR) for 30 min at 37 °C. Immunostaining was visualized with 3,3′-diaminobenzidine (DAB, Dojindo, Kumamoto, Japan) and counterstained with hematoxylin. A light microscope (DMi8; Leica, Wetzlar, Germany) was used to photograph and digitalize the slides. Nuclei were stained with Hoechst 33342 (Molecular probes) and observed by a TCS-SP8 confocal microscope (Leica).
Semi-quantitative histological analysis
Whole slide digital images (20 × magnification) of Masson’s trichrome or pERK stained sections including the entire cortex, medulla, and papilla were acquired using a scanner (BZ-9000 All-in-one Fluorescence Microscope, Keyence). A color threshold was applied at a level that separated the cysts from non-cystic tissue to calculate cyst volume. All histomorphometric analyses were performed blindly, without knowledge of group assignment. The cyst index was calculated as the total cystic area/total tissue area × 100 (%) [19, 20]. As the cysts usually take up most of the area of the renal medulla in the PCK rat model, we divided the total cystic area by the area of the medulla excluding the cysts, in accordance with previous studies [21].
The fluorescence intensities of Aqp2 in the kidneys were quantified using Image J software, according to the previous report [22].
Statistical analysis
Data are presented as means ± standard error of the means (SEM). Analysis of variance (ANOVA), followed by Tukey’s HSD (honest significant difference) test was used for comparison between the groups. A p value less than 0.05 was considered significant.
Results
HCTZ added to tolvaptan-induced changes in urinary output and blood pressure
Urine volume was significantly increased in rats treated with tolvaptan, but reduced in the Tol + HCTZ group after 2 weeks of HCTZ administration (Cont 13.3 ± 1.2 mL, HCTZ 14.5 ± 1.8 mL, Tol 37.1 ± 3.2 mL, Tol + HCTZ 26.3 ± 2.8 mL, p = 0.023 between Tol and Tol + HCTZ groups at week 3, Fig. 2a). After 8 weeks of treatment, urine output was 16.5 ± 0.8 mL in the Cont group, 18.6 ± 1.4 mL in the HCTZ group, 47.4 ± 2.7 mL in the Tol group, and 32.2 ± 3.0 mL in the combination group (p < 0.0001 by ANOVA, Fig. 2b). As shown in Table 1, HCTZ also significantly lowered urinary calcium excretion in both the HCTZ (0.8 ± 0.3 mg/dL) and Tol + HCTZ (0.8 ± 0.3 mg/dL) groups compared to the Cont (1.4 ± 0.5 mg/dL) and Tol (2.0 ± 0.2 mg/dL) groups. Treatment also increased plasma renin activity (PRA) in the Tol + HCTZ group (4.4 ± 2.7 ng/mL/h) compared to that of both the Cont (3.5 ± 1.6 ng/mL/h, p = 0.046) and Tol groups (1.7 ± 0.7 ng/mL/h, p = 0.005).

Hydrochlorothiazide was effective in reducing tolvaptan-induced polyuria. PCK rats were divided into four groups: control (Cont), tolvaptan-treated (Tol), hydrochlorothiazide-treated (HCTZ), and Tol + HCTZ combination treatment. a The 24 h urine volume change through the 8-week experimental period for each group. Values are mean ± SEM. *p < 0.05, compared to the Cont group. †p < 0.05, compared to the HCTZ group. ‡p < 0.05, compared to the Tol group. b Comparison of the 24 h urine volume between the groups at week 8, prior to sacrifice. Values are mean ± SEM. *p < 0.05, compared to the Cont group. †p < 0.05, compared to the HCTZ group. ‡p < 0.05, compared to the Tol group. All statistical analyses were performed with the Tukey–Kramer HSD test
Blood pressure was not changed by tolvaptan treatment during the experiment, which is consistent with tolvaptan administration studies on PCK rats [15, 23]. HCTZ administration was not also affected on blood pressure. After 8 weeks of treatment, blood pressure was 108.8 ± 2.5 mmHg in the Cont group, 101.3 ± 3.8 mmHg in the HCTZ group, 98.8 ± 2.5 mmHg in the Tol group, and 109.0 ± 3.8 mmHg in the Tol + HCTZ group (p = 0.07 by ANOVA, Table 1).
Cyst development and cell proliferation
Consistently with previous research [20, 24], tolvaptan attenuated PKD progression and improved renal function (Table 1). The cyst index in PCK rats was decreased in both the Tol and Tol + HCTZ groups (Fig. 3a, b). pERK expression was mainly observed in the medulla, with levels in both the Tol and Tol + HCTZ groups significantly lower compared to that of the Cont group (Fig. 3c, d). Notably, with regard to both cyst size and pERK expression, no significant differences were found between the Tol group and Tol + HCTZ group (Fig. 3b, d). Positive areas of Kim-1, a tubular damage marker, were appeared in pERK positive tubules (Fig. 3e).

Cyst development and cell proliferation in tolvaptan- and hydrochlorothiazide-treated PCK rats. Animals were divided into four groups: control (Cont), tolvaptan-treated (Tol), hydrochlorothiazide-treated (HCTZ), and Tol + HCTZ combination treatment. a Representative Masson’s Trichrome stained equatorial kidney sections of all experimental groups. b Cyst index comparison between sections from each experimental group. Values are mean ± SEM. *p < 0.05, compared to the Cont group. †p < 0.05, compared to the HCTZ group. c Phosphorylated extracellular signal-regulated kinase (pERK; red) and DAPI (blue)-stained kidney sections (scale bars = 100 µm). d Index comparison of pERK positive areas between groups showing HCTZ does not affect the cyst reducing effects of tolvaptan. Values are mean ± SEM. *p < 0.05, compared to the Cont group. †p < 0.05, compared to the HCTZ group. e Colocalize of kidney injury molecule-1 (KIM-1) and pERK appears in the tubular epithelial cells that are transforming or about to transform into cystic cells (scale bars = 100 µm). f Comparison of cyclin D1 (Ccnd1) mRNA expression in the medulla, where most of the cysts are located. Values are mean ± SEM. *p < 0.05, compared to the Cont group. All statistical analyses were performed with the Tukey–Kramer HSD test
We then proceeded to examine the effects of HCTZ on cell proliferation and the pERK/Ccnd1 pathway during tolvaptan treatment on a molecular level. As shown in Fig. 3f by qRT-PCR experiment, Ccnd1 mRNA expression was significantly lower in the medulla of both the Tol and Tol + HCTZ groups compared to that of the Cont group. No significant differences were found between the Tol and Tol + HCTZ group.
Aqp2 regulation
Tolvaptan has been shown to be involved in the regulation of Aqp2 in the collecting ducts [22, 25, 26]. Aqp2 might also contribute to the antidiuretic mechanism of HCTZ. Therefore, we investigated the impact of HCTZ on the expression and subcellular localization of Aqp2 [22, 27, 28]. It appears that Aqp2 expression was significantly reduced in the cortex in the Tol and Tol + HCTZ groups compared to that observed in the Cont group (Fig. 4a); however, there were no significant differences between the Cont and HCTZ groups or between the Tol and Tol + HCTZ groups. Redistribution of Aqp2 from the apical domain to the intracellular domain was observed in the Tol group compared to the Cont group. Notably, this redistribution was reversed in the Tol + HCTZ group (Fig. 4c–e).

Effects of tolvaptan and hydrochlorothiazide on aquaporin (Aqp) 2 expression in the kidneys of PCK rats. Animals were divided into four groups: control (Cont), tolvaptan-treated (Tol), hydrochlorothiazide-treated (HCTZ), and Tol + HCTZ combination treatment. mRNA expression of Aqp2 in the cortex (a) and medulla (b) in each treatment group. Values are mean ± SEM. *p < 0.05, compared to the Cont group with the Tukey–Kramer HSD test. c Representative images of kidney sections immunohistochemically stained for Aqp2 (scale bars = 100 µm). d Enlarged views of the black box areas showing the redistribution of Aqp2 from the apical domain to the intracellular domains (indicated with dashed arrows), which was partially reversed in the Tol + HCTZ group (indicated with solid arrows) (scale bars = 50 µm). e Immunofluorescence staining of Aqp2. The relative intensities of Aqp2 staining from basolateral to apical membrane (along dashed arrow) are shown (scale bars = 25 µm)
Treatment-induced changes in glomerular filtration rate and tubuloglomerular feedback
Despite the significant improvement in renal function, a negative effect on the glomerular filtration rate (GFR) was observed in the Tol + HCTZ group (Table 1). To investigate how molecules related to tubuloglomerular feedback (TGF) was affected, we analyzed Nos1, Ren and Ptges2 mRNA expression in the kidney (Fig. 5). The results showed a significant reduction in Nos1 and Ptges2 expression in the medulla in the Tol + HCTZ group (Fig. 5b, f). Ren mRNA expression was also lower in this group compared to that observed in the HCTZ group (Fig. 5d). These changes appear to occur solely in the medulla, and not in the cortex.

Analysis of TGF-related mRNA expressions. PCK rats were divided into four groups: control (Cont), tolvaptan-treated (Tol), hydrochlorothiazide-treated (HCTZ), and Tol + HCTZ combination treatment. a, b Comparison of nitric oxide synthase 1 (Nos1) expression in the kidney, a critical factor involved with the modulation of TGF responsiveness, showing that HCTZ administration had an impact on TGF. c, d Comparison of renin (Ren) expression in the kidney. e, f Comparison of microsomal prostaglandin E synthase 2 (Ptges2) expression in the kidney. Values are mean ± SEM. *p < 0.05, compared to the Cont group. †p < 0.05, compared to that of the HCTZ group. All statistical analyses were performed with the Tukey–Kramer HSD test
Discussion
The beneficial effects of tolvaptan in ADPKD are accompanied by the development of polyuria. HCTZ is often prescribed to reduce polyuria in diabetes insipidus. However, HCTZ and tolvaptan combination treatment has never been investigated in PKD. We investigated the efficacy of HCTZ in reducing polyuria during tolvaptan treatment in a PKD rat model. Our results showed for the first time that HCTZ significantly reduced urine volume in PCK rats, without affecting the beneficial effects of tolvaptan. Vasopressin V2 receptors and downstream cAMP signaling play an important role in PKD pathogenesis [29]. Indeed, changes in this pathway along with increased ERK activity and cell proliferation [30, 31], which lead to renal injury and interstitial fibrosis, are likely essential factors in cyst growth and expansion. Consistent with these PKD characteristics, Kim-1 and pERK co-localization in PCK rats was primarily observed in the medulla, especially in tubular epithelial cells that are transforming or about to transform into cystic cells. pERK activity and cyst size were also significantly lower in both the Tol and Tol + HCTZ groups, indicating that HCTZ did not affect the tolvaptan-mediated effects on cyst size reduction and pERK activity.
Furthermore, Ccnd1, a protein in the downstream of pERK pathway, is also a major regulator of cell-cycle progression [32, 33], and inappropriate proliferation and differentiation of renal tubular epithelial cells have been shown to lead to PKD cystogenesis [34]. Our results showed that both the Tol and Tol + HCTZ groups had significantly lower Ccnd1 expression in the kidney, further confirming that HCTZ treatment did not interfere with the prohibitive effects of tolvaptan on cyst formation.
HCTZ is a thiazide previously shown to be effective in reducing polyuria in both central and nephrogenic diabetes insipidus [12,13,14]. Despite having been used clinically for over 50 years [12, 13], the precise mechanism of this paradoxical antidiuretic effect of HCTZ, and other thiazides, is still unclear. It is generally believed that the thiazide-induced decrease in renal sodium uptake occurs through the inhibition of the sodium chloride cotransporter (NCC) in the renal distal convoluted tubule. This inhibition would temporarily induce a hypovolemic state, leading to a decreased GFR and increased renin–aldosterone–angiotensin system (RAAS) activation. Consequently, these changes result in a compensatory increase in proximal tubule sodium and water reabsorption, causing the observed antidiuretic effects. However, this does not appear to be the full mechanism. Experiments on lithium-induced nephrogenic diabetes insipidus rats showed that HCTZ could also partially increase Aqp2 abundance in the kidney, while Cesar et al. [27] showed that HCTZ increases water reabsorption in isolated rat inner medullary collecting ducts by increasing osmotic and diffusional water permeability, suggesting that thiazides may directly act on the vasopressin–AQP2 axis of principal cells [28]. More recently, experiments on NCC knockout mice with HCTZ suggested the possibility that the paradoxical antidiuretic effect might partially come from its inhibitive effects on carbonic anhydrase in the proximal tubule causing a decreased sodium–hydrogen antiporter (NHE) activity and increased fluid delivery to macula densa, creating a TGF response-mediated GFR reduction [35].
We thus examined the Aqp2 expression levels in the kidneys of Tol- and HCTZ-treated PCK rats. In this analysis, we found a significant decrease in Aqp2 mRNA expression in the renal cortex in groups treated with tolvaptan compared to groups without tolvaptan, consistent with other similar acute and chronic studies on rats treated with vasopressin antagonists [36, 37]. However, no significant differences in Aqp2 mRNA expression in the medulla between the groups were observed between the different treatment groups. This is most likely due to the inappropriate proliferation and differentiation of the renal tubular epithelial cells that were undergoing in the medulla during cyst formation. It has also been previously demonstrated that Aqp2 expression in cysts is significantly lower compared to that of non-cystic tubules [38]. Thus, when cysts formation is attenuated in the medulla, the normal cells expressing Aqp2 mask the lower expression of Aqp2 caused by tolvaptan treatment. Furthermore, we also observed a redistribution of Aqp2 from the apical domain to the intracellular domains in both the cortical and medullary collecting ducts, a phenomenon which was partially reversed following HCTZ treatment, possibly contributing to its antidiuretic effect.
To examine how molecules related to the TGF under HCTZ administration was affected, we tested the expression of Ptges2 and Nos1. Predominantly expressed in macula densa cells [39], Nos1 is critical in the TGF response and renin signaling cascade [39, 40], while Ptges2 and the synthesis and release of prostaglandin E2 are critical downstream elements of macula densa-mediated signaling of renin release [41, 42]. Although expression of Nos1 and Ptges2 mRNA in the medulla were lowered in both Tol + HCTZ group and Tol group, no significant difference in the expression in the cortex were found, in either case, no significant differences between the Tol group and Tol + HCTZ group was found (Fig. 5). Thus, it is unlikely that nitric oxide and prostaglandin E2, mediators of TGF, are responsible for the reduction of polyuria with HCTZ.
More studies on the intricate changes inside renal medulla involving Nos1 and Ptges2 following tolvaptan treatment might need to be conducted as in our current study. We did not identify any significant differences between the Tol and Tol + HCTZ group in this regard. We thus tried NHE3 immunostaining to determine the effect of tubular sodium handling on HCTZ treatment. However, no clear differences among the groups were observed in this study (data not shown). Although Tol + HCTZ group in the current study showed a lowered creatinine clearance, with the above results and an elevated PRA (Table 1) in consideration, the paradoxical antidiuretic effect of HCTZ in the Tol + HCTZ group might have more to do with an activated RAAS, allegedly a compensatory response [43, 44] following HCTZ administration. This would consequently result in an elevated angiotensin II level that acts on the sodium–hydrogen exchanger in the proximal tubules, causing more sodium reabsorption [45].
Conclusion
In this study, we demonstrated the effectiveness of combining HCTZ and tolvaptan treatment as a treatment for PKD in PCK rats. Our results indicate that there were no adverse HCTZ-mediated effects on tolvaptan function during treatment. To our knowledge, this is the first time HCTZ and tolvaptan have been investigated as a combination therapy for PKD. While further investigation is required to clarify the renoprotective effects of combination therapy in human ADPKD patients, this animal study highlights a novel treatment option to minimize the negative effects of tolvaptan. Although caution should be taken with regards to the negative impact on renal clearance, we believe this new therapeutic combination could potentially lead to better PKD treatments and improved quality of life for the affected patients.
References
Chapman AB, Devuyst O, Eckardt KU, et al. Autosomal-dominant polycystic kidney disease (ADPKD): executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2015;88(1):17–27.
Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic kidney disease. Lancet. 2007;369(9569):1287–301.
Martínez V, Comas J, Arcos E, et al. Renal replacement therapy in ADPKD patients: a 25-year survey based on the Catalan registry. BMC Nephrol. 2013;14:186.
Collins AJ, Foley RN, Herzog C, et al. US renal data system 2012 annual data report. Am J Kidney Dis. 2013;61(1 Suppl 1):A7 (e1–476).
Lager DJ, Qian Q, Bengal RJ, Ishibashi M, Torres VE. The pck rat: a new model that resembles human autosomal dominant polycystic kidney and liver disease. Kidney Int. 2001;59(1):126–36.
Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367(25):2407–18.
Casteleijn NF, Messchendorp AL, Bae KT, et al. Polyuria due to vasopressin V2 receptor antagonism is not associated with increased ureter diameter in ADPKD patients. Clin Exp Nephrol. 2017;21(3):375–82.
Hora M, Reischig T, Hes O, Ferda J, Klecka J. Urological complications of congenital nephrogenic diabetes insipidus—long-term follow-up of one patient. Int Urol Nephrol. 2006;38(3–4):531–2.
Higuchi A, Kawamura T, Nakai H, Hasegawa Y. Infrequent voiding in nephrogenic diabetes insipidus as a cause of renal failure. Pediatr Int. 2002;44(5):540–2.
Maroz N, Maroz U, Iqbal S, Aiyer R, Kambhampati G, Ejaz AA. Nonobstructive hydronephrosis due to social polydipsia: a case report. J Med Case Rep. 2012;6:376.
Singh H, Linas SL. Compulsive water drinking in the setting of anticholinergic drug use: an unrecognized cause of chronic renal failure. Am J Kidney Dis. 1995;26(4):586–9.
Crawford JD, Kennedy GC, Hill LE. Clinical results of treatment of diabetes insipidus with drugs of the chlorothiazide series. N Engl J Med. 1960;262:737–43.
Al nofal A, Lteif A. Thiazide diuretics in the management of young children with central diabetes insipidus. J Pediatr. 2015;167(3):658–61.
Forrest JN, Cohen AD, Torretti J, Himmelhoch JM, Epstein FH. On the mechanism of lithium-induced diabetes insipidus in man and the rat. J Clin Investig. 1974;53(4):1115–23.
Wang X, Gattone V II, Harris PC, Torres VE. Effectiveness of vasopressin V2 receptor antagonists OPC-31260 and OPC-41061 on polycystic kidney disease development in the PCK rat. J Am Soc Nephrol. 2005;16(4):846–51.
Salvetti A, Ghiadoni L. Thiazide diuretics in the treatment of hypertension: an update. J Am Soc Nephrol. 2006;17(4 Suppl 2):25–9.
Nair AB, Jacob S. A simple practice guide for dose conversion between animals and human. J Basic Clin Pharm. 2016;7(2):27–31.
Reungjui S, Roncal CA, Mu W, Srinivas TR, Sirivongs D, Johnson RJ, Nakagawa T. Thiazide diuretics exacerbate fructose-induced metabolic syndrome. J Am Soc Nephrol. 2007;18(10):2724–31.
Yamamoto J, Nishio S, Hattanda F, et al. Branched-chain amino acids enhance cyst development in autosomal dominant polycystic kidney disease. Kidney Int. 2017;92(2):377–87.
Gattone VH, Wang X, Harris PC, Torres VE. Inhibition of renal cystic disease development and progression by a vasopressin V2 receptor antagonist. Nat Med. 2003;9(10):1323–6.
Seo MY, Yang J, Lee JY, et al. Renal Klotho expression in patients with acute kidney injury is associated with the severity of the injury. Korean J Intern Med. 2015;30(4):489–95.
Ando F, Sohara E, Morimoto T, Yui N, Nomura N, Kikuchi E, Takahashi D, Mori T, Vandewalle A, Rai T, Sasaki S, Kondo Y, Uchida S. Wnt5a induces renal AQP2 expression by activating calcineurin signalling pathway. Nat Commun. 2016;7:13636.
Hopp K, Wang X, Ye H, Irazabal MV, Harris PC, Torres VE. Effects of hydration in rats and mice with polycystic kidney disease. Am J Physiol Ren Physiol. 2015;308(3):F261–6.
Sabbatini M, Russo L, Cappellaio F, et al. Effects of combined administration of rapamycin, tolvaptan, and AEZ-131 on the progression of polycystic disease in PCK rats. Am J Physiol Ren Physiol. 2014;306(10):F1243–50.
Ando F, Sohara E, Morimoto T, et al. Wnt5a induces renal AQP2 expression by activating calcineurin signalling pathway. Nat Commun. 2016;7:13636.
Whiting JL, Ogier L, Forbush KA, et al. AKAP220 manages apical actin networks that coordinate aquaporin-2 location and renal water reabsorption. Proc Natl Acad Sci USA. 2016;113(30):E4328–37.
César KR, Magaldi AJ. Thiazide induces water absorption in the inner medullary collecting duct of normal and Brattleboro rats. Am J Physiol. 1999;277(5 Pt 2):F756–60.
Earley LE, Orloff J. The Mechanism of antidiuresis associated with the administration of hydrochlorothiazide to patients with vasopressin-resistant diabetes insipidus. J Clin Investig. 1962;41(11):1988–97.
Torres VE, Harris PC. Strategies targeting cAMP signaling in the treatment of polycystic kidney disease. J Am Soc Nephrol. 2014;25(1):18–32.
Cohen JD, Tham KY, Mastrandrea NJ, Gallegos AC, Monks TJ, Lau SS. cAMP-dependent cytosolic mislocalization of p27(kip)-cyclin D1 during quinol-thioether-induced tuberous sclerosis renal cell carcinoma. Toxicol Sci. 2011;122(2):361–71.
Cohen JD, Gard JM, Nagle RB, Dietrich JD, Monks TJ, Lau SS. ERK crosstalks with 4EBP1 to activate cyclin D1 translation during quinol-thioether-induced tuberous sclerosis renal cell carcinoma. Toxicol Sci. 2011;124(1):75–87.
Sherr CJ. Cancer cell cycles. Science. 1996;274(5293):1672–7.
Zhao J, Li L, Wei S, et al. Clinicopathological and prognostic role of cyclin D1 in esophageal squamous cell carcinoma: a meta-analysis. Dis Esophagus. 2012;25(6):520–6.
Happé H, Peters DJ. Translational research in ADPKD: lessons from animal models. Nat Rev Nephrol. 2014;10(10):587–601.
Sinke AP, Kortenoeven ML, De Groot T, et al. Hydrochlorothiazide attenuates lithium-induced nephrogenic diabetes insipidus independently of the sodium-chloride cotransporter. Am J Physiol Ren Physiol. 2014;306(5):F525–33.
Christensen BM, Marples D, Jensen UB, et al. Acute effects of vasopressin V2-receptor antagonist on kidney AQP2 expression and subcellular distribution. Am J Physiol. 1998;275(2 Pt 2):F285–97.
Xu DL, Martin PY, Ohara M, et al. Upregulation of aquaporin-2 water channel expression in chronic heart failure rat. J Clin Investig. 1997;99(7):1500–5.
Pavlov TS, Levchenko V, Ilatovskaya DV, Palygin O, Staruschenko A. Impaired epithelial Na+ channel activity contributes to cystogenesis and development of autosomal recessive polycystic kidney disease in PCK rats. Pediatr Res. 2015;77(1–1):64–9.
Wilcox CS, Welch WJ, Murad F, et al. Nitric oxide synthase in macula densa regulates glomerular capillary pressure. Proc Natl Acad Sci USA. 1992;89(24):11993–7.
Juncos LA, Garvin J, Carretero OA, Ito S. Flow modulates myogenic responses in isolated microperfused rabbit afferent arterioles via endothelium-derived nitric oxide. J Clin Investig. 1995;95(6):2741–8.
Lorenz JN, Weihprecht H, Schnermann J, Skøtt O, Briggs JP. Renin release from isolated juxtaglomerular apparatus depends on macula densa chloride transport. Am J Physiol. 1991;260(4 Pt 2):F486–93.
Peti-peterdi J, Komlosi P, Fuson AL, et al. Luminal NaCl delivery regulates basolateral PGE2 release from macula densa cells. J Clin Investig. 2003;112(1):76–82.
Ernsberger P, Koletsky RJ. Metabolic effects of antihypertensive agents: role of sympathoadrenal and renin-angiotensin systems. Naunyn Schmiedebergs Arch Pharmacol. 2006;373(4):245–58.
Jessup JA, Brosnihan KB, Gallagher PE, Chappell MC, Ferrario CM. Differential effect of low dose thiazides on the renin angiotensin system in genetically hypertensive and normotensive rats. J Am Soc Hypertens. 2008;2(2):106–15.
Geibel J, Giebisch G, Boron WF. Angiotensin II stimulates both Na(+)-H+ exchange and Na+/HCO3 − cotransport in the rabbit proximal tubule. Proc Natl Acad Sci USA. 1990;87(20):7917–20.
Acknowledgements
The authors are grateful to the Biomedical Research Unit of Tohoku University Hospital and the Institute for Animal Experimentation Tohoku University Graduate School of Medicine as well as the Center of Research Instruments, Institute of Development, Aging and Cancer (IDAC), Tohoku University for the use of their equipment. We thank Ms. Yayoi Aoyama for technical assistance. This study was supported in part by Grants for Scientific Research (Japan Society for the Promotion of Science; 23659438, 25860156, 26670424, 15K18694, 15H04834, and 16H05312) from the Ministry of Education, Culture, Sports, Science and Technology of Japan (MEXT).
Author information
Authors and Affiliations
Contributions
AW, TH, and TM designed the study and wrote the initial draft of the manuscript. TM and SI supervised the project. AW, YO, and CT performed the animal experiments. AW, TH, CT, ES, IO-Y, SK, and YM contributed to the analysis and interpretation of data. All authors critically reviewed the manuscript and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
T.M. and S.I. are consultants for a clinical trial being conducted by Otsuka Pharmaceutical. T.M. has also received honoraria for lectures and research funding from Otsuka Pharmaceutical. The Division of Integrative Renal Replacement Therapy is financially supported by Terumo, JMS, Kyowa Hakko Kirin, and Otsuka Pharmaceutical.
Ethical approval
All procedures performed in studies involving animals were in accordance with the ethical standards of the institution or practice at which the studies were conducted (IRB approval number: 2015MdA-085 and 2016MdA-177).
About this article

Cite this article
Wang, A., Hirose, T., Ohsaki, Y. et al. Hydrochlorothiazide ameliorates polyuria caused by tolvaptan treatment of polycystic kidney disease in PCK rats. Clin Exp Nephrol 23, 455–464 (2019). https://doi.org/10.1007/s10157-018-1669-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-018-1669-9