
Abstract
Background
Elevated urine Mg excretion and its correlation with histological damage in tubulo-interstitial nephropathy (TIN) were reported. Here we investigated the clinical significance of the fractional excretion of Mg (FEMg) for the prediction of TIN.
Methods
We enrolled and assessed 94 adult patients with various renal diseases diagnosed principally by renal biopsy.
Results
Our stratified analysis based on the value of the conventional TIN parameter N-acetylglucosaminidase (NAG) excretion showed that the high-NAG index group (more than median value of NAG-to-Cr ratio, n = 47) demonstrated significantly high FEMg values (p = 0.017). A univariate analysis revealed a significant correlation between the FEMg and the NAG index (R = 0.60) but not for other parameters. A multivariate regression analysis confirmed the significance of the FEMg as an effective predictor of the NAG index. The FEMg showed a significant correlation with the estimated glomerular filtration rate (eGFR) in the patients with eGFR ≤ 30 mL/min. The correlation of FEMg with the NAG index was not observed in the primary glomerulonephritis patients but was apparent in the patients with hypertensive nephrosclerosis or interstitial nephritis.
Conclusion
Our findings may indicate that the combination of the FEMg and the NAG index can provide a specific, sensitive assessment for TIN in patients without renal insufficiency.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Tubulo-interstitial nephropathy (TIN) has been recognized as a significant determinant of disease severity or prognosis in various kidney diseases, as have glomerular disorders [1, 2]. In primary glomerulonephritis and in glomerular injury-predominant disorders such as diabetic nephropathy, it would be reasonable to assess the disease activity or prognosis by examining urine abnormalities such as proteinuria or hematuria or by investigating changes in the serum Cr level or GFR, because impaired filtration efficacy caused by structural damage in the glomeruli often develops in such glomerular injury-predominant disorders. However, in TIN, the lack of an elevation of serum Cr does not straightforwardly indicate less severity of interstitial damage, because the glomerular injury would be secondary in the interstitial-predominant disorders [3]. In TIN, the absence of apparent urine abnormalities and the lesser elevation of Cr compared to the severity of interstitial impairment are not rare. Although TIN is frequently a secondary disorder following glomerular injury, glomerular injury and TIN often exist independently until severe renal impairment develops [3], and it is generally known that the severity of interstitial impairment shows a more evident correlation with the renal prognosis than does the glomerular injury [4]. The accurate diagnosis and the assessment of the disease severity of TIN often depend on a histopathological approach, but there is a clinical limitation due to the inability to obtain a kidney biopsy in many cases. Therefore, clinical parameters that are sensitive and specific to TIN are required for the management of patients.
Both N-acetylglucosaminidase (NAG) and β2-microglobulin (β2MG)—which is more commonly used instead of α1-microglobulin in Japan—are regularly used as clinical indexes for the assessment of TIN. β2MG, one of the components of major histocompatibility complex, is ubiquitously distributed on the surface of nucleated cells. Excreted β2MG from the cell surface is completely filtered through the glomerulus, and is mostly reabsorbed from the proximal tubule. Consequently, dysfunction of the proximal tubules associated with TIN would lead to an increase in the β2MG excretion. However, the β2MG excretion would also depend on the glomerular filtration and should be affected by a glomerular injury, indicating that an elevation of the β2MG excretion is not particularly specific to TIN [5]. NAG is a lysosomal enzyme distributed exclusively in the proximal tubules and prostate, and the increased NAG excretion is generally believed to indicate organic damage of the proximal tubules. However, NAG excretion is also known to be enhanced in cases of glomerulonephritis [6].
The fractional excretion of magnesium (FEMg) has been adopted to evaluate TIN, and it was found that FEMg directly correlates with the degree of histological damage of the interstitium [7–10]. A variety of disorders related to the structure and function of the tubular epithelium can affect magnesium reabsorption and lead to a further loss of magnesium into the urine. Therefore, an elevation of the FEMg beyond the normal range might indicate the existence of a tubular disorder or a disorder affecting tubular function, such as TIN. Indeed, hypermagnesiuria was revealed in a patient with Sjogren syndrome and another patient with leptospirosis and interstitial fibrosis [11, 12]. In those reports, the underlying mechanism was presumed to be related to the tubular dysfunction associated with TIN.
These clinical observations and study findings strongly suggest that TIN provokes urinary magnesium wasting due to tubular dysfunction, and the findings might also indicate that the evaluation of magnesium excretion would be beneficial as an independent clinical parameter to estimate the presence and severity of TIN. Despite the clinical significance of hypermagnesiuria in patients with TIN, previous studies and reports simply show the correlation between urine magnesium excretion and the presence or histological severity of TIN; they did not describe any assessment of the correlations between urine magnesium excretion and conventional clinical indexes such as NAG or β2MG.
Here we studied the evaluation of FEMg as an alternative approach to estimate the presence of TIN by focusing on its correlations with the urine excretions of NAG in patients with a variety of renal disorders who were diagnosed mainly by renal biopsy. Based on our findings, we propose that FEMg shows high sensitivity for the assessment of TIN similar to NAG excretion, and higher specificity for TIN than NAG excretion. Therefore, we suggest that the combination of NAG and FEMg measurements might provide a more sensitive and specific assessment of TIN.
Materials and methods
Study subjects
This study was performed in accord with the principles of the Declaration of Helsinki. We enrolled male and female adult (15- to 80-year-old) patients at the outpatient unit of our hospital between June 2001 and May 2012 who were diagnosed mostly with histologically confirmed renal diseases, and who provided their agreement to the use of their laboratory data. Some patients were diagnosed based on their clinical history of long-term hypertension in combination with the findings of eye ground, blood and urine tests. Patients were excluded from this study if they exhibited renal failure [estimated glomerular filtration rate (eGFR) ≤15 mL/min], heart failure (New York Heart Association functional class III or IV for dyspnea at exertion), or severe liver dysfunction. The aim of this study, both advantages and disadvantages for the participants, and the details of analysis were explained to each patient, and informed consent was obtained. The investigational protocol was approved by the Ethics Committee for Human Studies at Saitama Medical University on June 1, 2012.
Diuretics were not administered to these patients during the testing or within 24 h prior to testing. Briefly, after a regular supper, no additional food except ad lib drinking water was allowed. Blood and urine were analyzed by the laboratory unit of our hospital. The FEMg was calculated using the following formula:
where, U represents the urine concentration and P represents the plasma concentration.
Study protocol
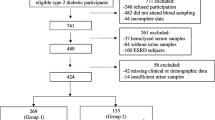
We enrolled 94 patients who satisfied the inclusion and exclusion criteria and consented to participate in this study. We obtained blood and urine samples without any changes in the patients’ therapy, including medication protocols. The diagnosis of hypertension was performed following the 2009 Japanese Society of Hypertension Guidelines (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg) [13]. The criteria for diabetes and dyslipidemia were the use of antihyperglycemic medications or fasting blood glucose >125 mg/dL, and the use of lipid-lowering medications or total cholesterol ≥220 mg/dL and/or high-density lipoprotein-cholesterol ≤40 mg/dL and/or triglyceride ≥150 mg/dL.
Statistical analysis
Most of the biochemical parameters are expressed as means ± standard deviations. The protein-to-creatinine ratio, the urine NAG-to-creatinine and the urine β2MG-to-Cr ratios (NAG and β2MG indexes) did not have a parametric distribution; and therefore, they are expressed as median and 1st- and 3rd-quartile values. We determined the significance of differences in continuous variables with a parametric distribution by a two-tailed unpaired t-test for two groups’ comparison if an analysis of variance (ANOVA) demonstrated an equal distribution and by Welch’s t-test if the ANOVA demonstrated a nonequal distribution. The significance of paired and unpaired variables with a nonparametric distribution was evaluated using Wilcoxon’s signed-rank test and the Mann–Whitney U test, respectively. All statistical analyses were undertaken using a microcomputer-assisted program with SPSS (version 20.0) for Windows XP (IBM, Armonk, NY). A p value <0.05 was considered significant.
Results
Clinical profile of enrolled patients
Table 1 provides the clinical profile of the 94 enrolled patients. The mean age of the enrolled patients was 52 years, but the ages of the individual patients were widely distributed, from 16 to 80 years. All cases of primary glomerulonephritis were histologically diagnosed by renal biopsy and included ten cases of IgA nephropathy, eight cases of focal segmental glomerulosclerosis, seven cases of membranous nephropathy, and nine cases of post-minimal change nephrotic syndrome.
The clinical category of nephrosclerosis included ten cases of histologically diagnosed hypertensive nephrosclerosis. The remaining 11 cases were diagnosed based on the clinical features of a hypertension history for ≥10 years, eye ground findings compatible with hypertensive fine arteriole sclerosis (≥H2S2 of Scheie’s classification), and elevated serum creatinine or the presence of proteinuria. All cases of TIN were histologically diagnosed as TIN-predominant renal disorder, including four cases of acute TIN.
Stratified analysis by the NAG index
First of all, to identify the clinical parameters which showed difference according to the estimated severity of the interstitial injury, multiple parameters were stratified by the median value of the NAG index. As demonstrated in Table 2, the stratified analysis revealed that in the high-NAG index group, parameters that generally indicate renal dysfunction (including serum creatinine, eGFR, serum uric acid and the urine protein-to-Cr ratio) showed significantly high values. The β2MG index values did not differ significantly between the high-and low-NAG index patient groups (n = 47 each). The serum concentrations of sodium and magnesium were not significantly different between the two groups, whereas the FEMg was significantly high in the high-NAG index group (p = 0.017). The serum potassium level and the fractional excretion of sodium (FENa) were also significantly high in the high-NAG index group as a result of renal dysfunction.
Correlation analysis of FEMg with NAG index and β2MG Index
We next studied the correlation between FEMg and the NAG index by performing a univariate analysis focusing on the parameters that showed a significant difference in the stratified analysis. As shown in Table 3, FEMg showed a significant correlation with the NAG index, whereas all other parameters did not show a significant correlation. Our subsequent multivariate analysis revealed that FEMg was the only significant predictor for the NAG index among all the parameters that showed a significant difference in the stratified analysis.
For a comparative assessment, we also performed a univariate analysis between FEMg and the β2MG index (Table 3). Unlike the analysis with the NAG index, multiple parameters showed a significant correlation. Similarly, the multivariate analysis revealed multiple parameters as predictive factors for the β2MG index, suggesting that the β2MG index was principally affected by the reduced GFR or the diminished number of functional nephrons, and consequently, indicating that the specificity of the β2MG index for TIN would be inferior to that of the NAG index.
Assessment of the effect of the eGFR on the significance of FEMg
The correlation between the FEMg and the eGFR was also studied to examine the influence of the GFR on the FEMg (Fig. 1). The FEMg showed a significant negative correlation with the eGFR (Fig. 1a), indicating that the FEMg was markedly influenced by the eGFR in addition to the TIN. However, when the patients for the analysis were limited to those who showed an eGFR ≥ 30 mL/min, the significant correlation disappeared (Fig. 1b). In contrast, the correlation between the FEMg and the NAG index was still preserved in the same limited set of patients (Fig. 1c).

The correlation of the FEMg with the eGFR and with the NAG-to-Cr ratio in patients with different glomerular filtration rates. The individual correlations between the FEMg and the eGFR of all cases (a), those with eGFR values ≥30 mL/min (b), and the NAG-to-Cr ratio in patients showing eGFR ≥ 30 mL/min (c). Regression lines show a significant correlation
Significance of the FEMg in various disease settings
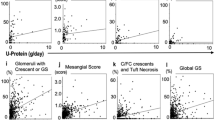
For the assessment of the clinical benefit of FEMg measurement, we sampled the cases of the patients with the diagnoses of primary glomerulonephritis, TIN, and nephrosclerosis, which are disease settings showing a glomerular injury-dominant impairment, an interstitial injury-dominant impairment, and injury of both glomeruli and interstitium, respectively, and we assessed the cases by a univariate analysis. When the NAG index was used as a response variable and the FEMg and eGFR were used as predictor variables, there was no significant correlation in the primary glomerulonephritis group (Table 4; Fig. 2a), indicating that urine NAG excretion is independent of both the FEMg and eGFR in this disease criterion. However, in the nephrosclerosis group, the NAG index showed significant correlations with both the FEMg and eGFR (Table 4; Fig. 2b). Interestingly, the NAG index in the TIN group showed a significant correlation only with the FEMg, not with the eGFR (Table 4; Fig. 2c), suggesting that the severity of TIN would not directly affect the reduction of GFR.

Correlations of the FEMg and the NAG-to-Cr ratio in patients diagnosed with biopsy-proven glomerulonephritis (a, n = 38), hypertensive nephrosclerosis (b, n = 21), and tubulointerstitial damage-predominant renal disorder confirmed by renal biopsy (c, n = 22). Regression lines show the significant correlations
Discussion
The results of the present study showed a significant correlation between the FEMg and the NAG index, indicating the potential practicality of the FEMg for the assessment of TIN. Our present findings also revealed that the FEMg would be more selective for distinguishing TIN from glomerular injury-predominant disorders compared to the NAG index. Additionally, the significant positive correlation with the NAG index in the TIN-predominant disease group suggested the conceivable significance of FEMg as a possible predictor of the severity of TIN. Consequently, the combination of FEMg and the NAG index would enable clinicians to evaluate patients with TIN more thoroughly in cases showing an eGFR of 30 mL/min or more.
A positive correlation between urine magnesium excretion and the degree of histological impairment of the interstitium has been demonstrated in multiple studies [8, 10]. However, the correlation between FEMg and conventional parameters, and the specificity of FEMg to TIN-predominant disorders have never been studied yet in those previous studies [8, 10]. The kidney plays a central role in the maintenance of magnesium metabolism in the body by reabsorbing the majority of filtered magnesium into the tubules [14]. The most susceptible tubule subsegments for the magnesium reabsorption are proximal tubules, the thick ascending limb of Henle (TAL), and distal convoluted tubules, which are responsible for reabsorbing 10–30, 40–70 and 5–10 % of the filtered magnesium, respectively [14]. Therefore, elevated urine magnesium excretion showing an inhibition of tubular magnesium reabsorption could be caused by disorders of the various tubular segments. This might be a critical point and an advantage of the FEMg as a parameter of TIN in the various parts of the kidney, unlike the urine NAG excretion, which would be affected primarily by an injury to the proximal tubules or glomeruli.
Conventionally, the NAG and β2MG indexes have been widely used in clinical assessments of the presence and severity of TIN in Japan. The urine excretion of NAG in particular is known to show higher values according to the severity of TIN, and its specificity is considered to be higher than that of β2MG [15, 16]. Likewise, it was reported that the FEMg is useful as a noninvasive parameter for estimating the severity of TIN and also for the indications for a renal biopsy [10]. However, the correlation between the parameters of the FEMg and the NAG index had not been studied yet, to our knowledge. The significant correlation between the NAG index and the FEMg shown in the present study contributes to the clinical usefulness of the FEMg as a parameter of TIN.
The primary cause of the increased NAG excretion is considered to be an organic disorder of proximal tubule epithelial cells, which contain a large amount of NAG. However, NAG excretion is also affected by a glomerular injury. It is known that urine NAG excretion is enhanced concomitantly with a glomerular injury such as primary glomerulonephritis [6], suggesting that the FEMg could be a more selective parameter for the diagnosis of TIN. In addition, fractional excretion of other ions, FENa or FEK, did not show significant correlation with the NAG index (data not shown). Multiplicity of tubular reabsorption of sodium or potassium might be involved in this dissociation, and the remaining number of functional nephrons might affect FENa or FEK rather than the severity of TIN.
To examine the specificity of the FEMg for TIN, we assessed the correlation between the FEMg and the NAG indexes in three subgroups of patients whose rates of glomerular and interstitial damage differed. The results showed that the correlation between the FEMg and the NAG index was significant in groups with TIN and nephrosclerosis but not with primary glomerulonephritis, suggesting that the elevated NAG excretion in the patients lacking the significant correlation is caused principally by the glomerular injury, and demonstrating that the FEMg would be more selective for TIN compared to the NAG index.
In this study, the FEMg showed an inverse correlation with the eGFR, conceivably suggesting that the FEMg is strongly affected by the decrease in the number of functional nephrons rather than the interstitial impairment. However, our findings revealed that the correlation was not significant when the analyzed subjects were limited to the patients with an eGFR ≥ 30 mL/min, although the correlation between the FEMg and the NAG indexes was still significant in these patients. This result indicates that the FEMg was affected by the interstitial damage more apparently than the decrease in GFR in the patients whose glomerular filtration is moderately preserved, and that the FEMg as a clinical parameter for TIN should be applied to patients showing eGFR ≥ 30 mL/min.
The mechanism underlying the correlation between magnesium excretion and TIN have not been well studied or elucidated. Some examples of drug-induced hypermagnesiuric hypomagnesemia associated with interstitial impairment, such as by gentamicin [17], FK506 [18], and carboplatin [19], have been reported. Interestingly, Deekajorndech et al. [10] demonstrated that the estimated blood flow of peritubular capillaries (PTCs) and magnesium excretion show an inverse correlation, suggesting that ischemia or oxidative stress may be highly involved in the increase in the FEMg.
The normal range of the FEMg is generally considered to be less than 2.2 % [10]. Considering that in the present study the upper limit of the confidence interval of the FEMg values in the low-NAG index group was 6.4 %, an approximately 6 % FEMg may be a reliable standard as a cut-off value for accepting the presence of TIN if patients show an eGFR ≥ 30 mL/min. Shah et al. [20] reported that the fractional excretion of ionized magnesium above 4 % in subjects with normal kidney function generally indicates renal magnesium wasting. The ionized ratio of serum magnesium would be approximately 70 %, resulting in a 5.7 % FEMg when the value of 4.0 % FEMg is converted to the value using total (not ionized) magnesium, which is almost consistent with the cut-off value of FEMg in the present study. We believe that a FEMg value of more than 6.0 % would provide a more accurate and noninvasive assessment of TIN in combination with an abnormally elevated NAG index.
There is a limitation in this study. Dietary magnesium intake in individual subject was not considered in the analysis. Because the variation of daily magnesium intake must somewhat influence FEMg, obtained results might be partly affected.
In conclusion, an increase in the FEMg might be of use as a clinical parameter for the assessment of TIN. Particularly, high values of both FEMg and the NAG index would strongly suggest the presence of a TIN-predominant renal disorder, and a dissociation of these two parameters may be a reliable sign of a glomerular injury-predominant disorder.
References
Mackensen-Haen S, Bader R, Grund KE, Bohle A. Correlations between renal cortical interstitial fibrosis, atrophy of the proximal tubules and impairment of the glomerular filtration rate. Clin Nephrol. 1981;15:167–71.
Nath KA. Tubulointerstitial changes as a major determinant in the progression of renal damage. Am J Kidney Dis. 1992;20:1–17.
Rodriguez-Iturbe B, Johnson RJ, Herrera-Acosta J. Tubulointerstitial damage and progression of renal failure. Kidney Int Suppl. 2005;99:S82–6.
Gilbert RE, Cooper ME. The tubulointerstitium in progressive diabetic kidney disease: more than an aftermath of glomerular injury? Kidney Int. 1999;56:1627–37.
Donadio C. Serum and urinary markers of early impairment of GFR in chronic kidney disease patients: diagnostic accuracy of urinary beta-trace protein. Am J Physiol Renal Physiol. 2010;299:F1407–23.
Morii T, Fujita H, Narita T, Koshimura J, Shimotomai T, Fujishima H, Yoshioka N, Imai H, Kakei M, Ito S. Increased urinary excretion of monocyte chemoattractant protein-1 in proteinuric renal diseases. Ren Fail. 2003;25:439–44.
Braden GL, Germain MJ, Fitzgibbons JP. Impaired potassium and magnesium homeostasis in acute tubulo-interstitial nephritis. Nephron. 1985;41:273–8.
Futrakul P, Yenrudi S, Futrakul N, Sensirivatana R, Kingwatanakul P, Jungthirapanich J, Cherdkiadtikul T, Laohapaibul A, Watana D, Singkhwa V, Futrakul S, Pongsin P. Tubular function and tubulointerstitial disease. Am J Kidney Dis. 1999;33:886–91.
Miura K, Nakatani T, Asai T, Yamanaka S, Tamada S, Tashiro K, Kim S, Okamura M, Iwao H. Role of hypomagnesemia in chronic cyclosporine nephropathy. Transplantation. 2002;73:340–7.
Deekajorndech T. A biomarker for detecting early tubulointerstitial disease and ischemia in glomerulonephropathy. Ren Fail. 2007;29:1013–7.
Khositseth S, Sudjaritjan N, Tananchai P, Ong-ajyuth S, Sitprija V, Thongboonkerd V. Renal magnesium wasting and tubular dysfunction in leptospirosis. Nephrol Dial Transplant. 2008;23:952–8.
Kim YK, Song HC, Kim WY, Yoon HE, Choi YJ, Ki CS, Park CW, Yang CW, Kim J, Kim YS, Choi EJ, Bang BK. Acquired Gitelman syndrome in a patient with primary Sjogren syndrome. Am J Kidney Dis. 2008;52:1163–7.
Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mitsuyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshima H, Umemura S, Ishimitsu T, Rakugi H. The Japanese Society of Hypertension Guidelines for the management of hypertension (JSH 2009). Hypertens Res. 2009;32:3–107.
Glaudemans B, Knoers NV, Hoenderop JG, Bindels RJ. New molecular players facilitating Mg(2+) reabsorption in the distal convoluted tubule. Kidney Int. 2010;77:17–22.
Abraham P, Indirani K, Sugumar E. Effect of cyclophosphamide treatment on selected lysosomal enzymes in the kidney of rats. Exp Toxicol Pathol. 2007;59:143–9.
Morii T, Fujita H, Narita T, Shimotomai T, Fujishima H, Yoshioka N, Imai H, Kakei M, Ito S. Association of monocyte chemoattractant protein-1 with renal tubular damage in diabetic nephropathy. J Diabetes Complicat. 2003;17:11–5.
Foster JE, Harpur ES, Garland HO. An investigation of the acute effect of gentamicin on the renal handling of electrolytes in the rat. J Pharmacol Exp Ther. 1992;261:38–43.
Nijenhuis T, Hoenderop JG, Bindels RJ. Downregulation of Ca(2+) and Mg(2+) transport proteins in the kidney explains tacrolimus (FK506)-induced hypercalciuria and hypomagnesemia. J Am Soc Nephrol. 2004;15:549–57.
Ettinger LJ, Gaynon PS, Krailo MD, Ru N, Baum ES, Siegel SE, Hammond GD. A phase II study of carboplatin in children with recurrent or progressive solid tumors. A report from the Childrens Cancer Group. Cancer. 1994;73:1297–301.
Shah GM, Kirschenbaum MA. Renal magnesium wasting associated with therapeutic agents. Miner Electrolyte Metab. 1991;17:58–64.
Acknowledgments
This work was supported by the Financial Supporting Project for young investigators at Saitama Medical Center, Saitama Medical University (#24-C-1-C08), and was also supported, in part, by research grants from the Research Foundation for Community Medicine, Utsunomiya, Tochigi, Japan. We gratefully acknowledge Mr. T. Ozawa for his technical assistance.
Conflict of interest
The authors state that they have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Noiri, C., Shimizu, T., Takayanagi, K. et al. Clinical significance of fractional magnesium excretion (FEMg) as a predictor of interstitial nephropathy and its correlation with conventional parameters. Clin Exp Nephrol 19, 1071–1078 (2015). https://doi.org/10.1007/s10157-015-1099-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-015-1099-x