
Abstract
Background
Hypoalbuminemia caused by peritoneal dialysate protein loss, frequently occurs in patients on peritoneal dialysis (PD) and is associated with an increased risk of death. We investigate whether PD dialysis exchange volume (PD volume) could be reduced with tolvaptan (TVP) through increased urine volume (UV).
Methods
The study included 11 stable patients with oliguria undergoing PD. The following parameters were examined—diuretic response and the effect of TVP on peritoneal ultrafiltration (UF), body weight, serum albumin, sodium, arm muscle area (AMA), PD volume, dialysis efficiency calculator (K t/V), and urine and serum osmolarity (OSM).
Results
The average UV increased from 428 ± 178 to 906 ± 285 mL (p = 0.018 by paired t test). Average weekly PD volume decreased from 28,836 ± 5,699 to 23,872 ± 3,569 mL (p = 0.04 by paired t test). Average UF increased from 283 ± 147 to 575 ± 135 mL (p = 0.019 by paired t test). On the other hand, there was no significant difference in the average dialysate K t/V before and after TVP treatment. Serum sodium, AMA, and serum albumin levels were not statistically different before and after TVP treatment. The urine and serum OSM ratio of effective cases before TVP treatment was higher than that of ineffective cases (p = 0.024 by unpaired t test).
Conclusion
Our results indicate that TVP is useful for patients on continuous ambulatory PD who have oliguria and high urine osmolarity. Furthermore, we can reduce PD volume to maintain their nutritional status.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The use of peritoneal dialysis (PD) has become widespread since the introduction of continuous ambulatory PD (CAPD) over 25 years ago. During this period, many advances have been made and PD is an alternative to hemodialysis (HD), with excellent comparable survival, lower cost, and improved quality of life [1]. Hypoalbuminemia resulting from dialysate protein loss is, however, frequently observed in patients on PD and associated with an increased risk of death [2]. Nevertheless, we usually have to increase the dialysate volume for patients with reduced urine volume (UV), even if they already exhibit hypoalbuminemia.
Tolvaptan (TVP) (SAMSCA; Otsuka Pharmaceutical Co., Ltd), a selective vasopressin V2 receptor antagonist, has recently been available for patients with volume overload in heart failure (HF) when adequate response is not obtained with other diuretics. Recent clinical studies in Japan have demonstrated that short-term TVP treatment increased UV, decreased body weight (BW), and improved signs of fluid overload in patients with HF and excess fluid retention despite receiving loop and/or thiazide diuretics [3–5].
The unique mechanism of TVP action selectively blocks the binding of vasopressin to the V2 receptors (V2Rs) in the collecting duct of the kidney. If the V2Rs are left unblocked, the binding of vasopressin with these receptors can cause water retention resulting in hyponatremia. By inhibiting the effects of vasopressin at the V2R, TVP increases the excretion of free water, whereas the excretion of sodium and other electrolytes is not directly affected [6, 7].
Here, we examined whether PD volume could be reduced by increasing UV with TVP.
Method
Protocol
All patients underwent blood and urine tests including neurohumoral assessment, chest X-ray, and echocardiography before TVP therapy. TVP was administered at a low dose of 7.5 mg once daily after breakfast for 2–4 consecutive days. If oliguria persisted we increased the dose to 15 mg daily for >1 month between October 2011 and May 2012 at the Koyukai Memorial Hospital. Background diuretics and other cardiac medications were maintained and water intake was not restricted during the treatment period. Vital signs and UV were measured at baseline and every 8 h on the first day, and every 24 h subsequently. BW was measured every day after urination and before breakfast to the nearest 0.1 kg. A 24-h fluid intake measurement was recorded on the day before and following each treatment day. Blood and urine samples were collected at baseline and every 4 h during the first 8 h after administration of TVP, and every 24 h subsequently. All patients underwent repeated neurohumoral assessment and chest X-ray analysis once a month.
Parameter and laboratory data analysis
BW, UV, PD volume, ultrafiltration (UF), dialysis efficiency calculator (K t/V), arm muscle area (AMA), and serum concentrations of sodium, potassium, albumin, and urine concentrations of sodium (uNa), potassium (uK), and sodium concentration in PD drainage fluid (PD-Na) were studied immediately before initiation and immediately after one month of TVP treatment in all patients.
Urine and serum osmolarity (us OSM) ratio
We calculated the us OSM ratio as follows:
The us OSM ratio was calculated for each individual patient before TVP treatment and 1 month after TVP treatment. The unit of osmolarity is mOsm/kg.
Statistical analysis
Statistical analysis was performed using JMP for Windows software (SAS Institute Inc, Chicago, IL, USA) and Prism 6 for Macintosh software. Results are expressed as mean ± standard error of the mean. The statistical difference was determined by a 2-sided paired or unpaired Student’s t test. Differences with p value of <0.05 were considered significant.
Results
Patients
This study comprised 11 eligible participants (7 male, 4 female) undergoing PD treatment who had received TVP 7.5–15 mg/day for >1 month between October 2011 and May 2012 at the Department of Immunology and Nephrology of Koyukai Memorial Hospital. The median age of the patients was 78 years (range 52–91 years) (Table 1). In this study, eight of the patients chose automated PD (APD) and the remaining patients chose CAPD. All patients used both 1.5 % glucose dialysate and icodextrin dialysate. Five of the patients had diabetes mellitus (DM) and the remaining patients had nephrosclerosis (NS) as the primary disease. The median levels of sodium, potassium, N-terminal prohormone of brain natriuretic peptide (NT-pro BNP), creatinine clearance rate (CCr), and albumin were 138 mEq/L (range 127–146 mEq/L), 3.86 mEq/L (range 3.2–4.9 mEq/L), 9,615 pg/mL (range 927–40,536 pg/mL), 9.3 mL/min (range 1.2–13.4 mL/min), and 2.4 g/dL (range 1.5–3.4 g/dL), respectively. Furthermore, the median UV was 428 mL/day (range 8–1,417 mL/day) and median total volume of PD dialysate was 28,836 mL (range 6,000–42,000 mL/week). All patients were also medicated with furosemide and three of them were receiving spironolactone as combination diuretics. However, we did not change any drug throughout the study. The study was carried out according to the principles of the Declaration of Helsinki and was approved by the local ethics committee.
Changes in BW, serum sodium, serum potassium, serum albumin, and AMA during TVP treatment
BW decreased from 49.7 ± 8.1 kg to 47.3 ± 5.8 kg after 1 month of TVP treatment, although the difference between pre- and post-treatment BW did not reach statistical significance. Serum sodium, serum potassium, serum albumin, and AMA were not statistically different before and after the initiation of TVP treatment (Fig. 1).

Comparison of BW, Na, K, AMA, and albumin (Alb) before and after initiation of treatment with TVP, BW body weight, Na sodium, K potassium, AMA arm muscle area, Alb albumin
Changes in UV, PD volume, UF, and dialysis K t/V during TVP treatment
The average UV increased from 428 ± 178 to 906 ± 285 mL (p = 0.018 by paired t test). The average weekly PD volume decreased from 28,836 ± 5,699 mL to 23,872 ± 3,569 mL (p = 0.04 by paired t test). The average UF increased from 283 ± 147 to 575 ± 135 mL (p = 0.019 by paired t test). However, there was no significant difference in average dialysate K t/V before and after initiation of TVP treatment (Fig. 2).

Comparison of UV, PD volume, UF, and K t/V values obtained before and after treatment with TVP. UV urine volume, UF ultrafiltration
Changes in uNa and uK, and PD-Na during TVP treatment
uNa decreased from 72.1 ± 26.1 to 47.8 ± 17.7 mEq/L after TVP treatment, although the difference between pre- and post-treatment uNa did not reach statistical significance. uK and PD-Na were not statistically different before and after the initiation of TVP treatment (Fig. 3).

Comparison of uNa, uK, and PD-Na obtained before and after treatment with TVP. uNa urine sodium, uK urine potassium, PD-Na PD sodium
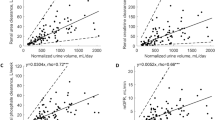
Relationship between UV and us OSM ratio
Figure 4 shows that the us OSM ratio before TVP treatment significantly correlated with delta UV after treatment (p = 0.0037, r = 0.6043).

Correlation between delta UV and us OSM ratio
Investigation of us OSM ratio
Treatment with TVP was either effective (effective cases) or ineffective (ineffective cases). We defined effective cases as those showing an increase in UV of >400 mL based on mean UV of patients or 2-fold increase in UV compared with UV before TVP treatment. The us OSM ratios of effective cases before TVP treatment were higher than those of ineffective cases (p = 0.024 by unpaired t test). The ratios of effective cases decreased from 15.2 ± 10.3 to −6.0 ± 10.6 after TVP treatment (p = 0.024 by paired t test). There was no statistical difference between ratios before and after the initiation of TVP treatment in ineffective cases (Fig. 5).

Comparison of us OSM ratio before and after initiation of treatment with TVP
Discussion
The nutritional and hydration status of patients on CAPD are the most essential aspects of their management because they influence survival [8, 9]. The survival of patients on CAPD was particularly related to serum albumin [9]. The loss of proteins into dialysate is considered a major limitation of maintenance PD. During maintenance PD, protein loss was 12.9 g/10 h of dialysis, albumin loss was 8.5 g/10 h, and immunoglobulin G loss was 1.3 g/10 h [10] The mean peritoneal protein loss was 5.8 ± 2.1 g/day (range 1.9–12.2 g/day) and protein clearance was 0.092 ± 0.041 L/24 h. Serum albumin was the unique parameter among biochemical and anthropometric measurements reflecting nutritional status, correlating with peritoneal protein loss. Peritoneal protein clearance was also not significantly correlated with measurements of visceral protein or somatic nutritional status, except serum albumin [11]. Hakemi et al. [12] showed that older patients on CAPD and patients with low serum albumin are at a high risk of mortality. Patients on CAPD, especially older patients, should have to reduce CAPD volume as much as possible to prevent protein loss. For this purpose, we usually use loop diuretics, thiazide, or spironolactone to increase UV; however, the adverse effects of these drugs limit their use. In particular, the use of high-dose loop diuretics is independently associated with increased mortality [13, 14]. Furthermore, furosemide produces natriuresis, leading to decreased serum sodium levels and activation of the renin−angiotensin−aldosterone system [15].
The neurohormone arginine vasopressin plays a significant role in the regulation of volume homeostasis, which is mediated by V2Rs in the collecting tubules of the kidney. TVP, a highly selective nonpeptide V2R antagonist, has demonstrated an improvement in volume status, osmotic balance, and hemodynamic profile [16]. TVP increases free water excretion and serum sodium levels while maintaining serum potassium levels. It has not been shown to decrease renal function or the glomerular filtration rate and is well tolerated. In HF, arginine vasopressin worsens HF by causing vasoconstriction of arteries and veins, potentially contributing to remodeling of the left ventricle and causing fluid retention and worsening of hyponatremia [17]. Plasma renin activity increases when furosemide or hydrochlorothiazide (HCTZ) is administered alone, but is unchanged after TVP treatment alone. TVP does not significantly affect the natriuretic activity of furosemide or HCTZ. Furosemide and HCTZ do not significantly affect the aquaretic activity of TVP [18].
On the basis of these data, we used TVP for patients with oliguria on CAPD to not only increase UV but also to reduce dialysis exchange volume.
As shown in Fig. 2, the average UV increased from 428 ± 178 to 906 ± 285 mL (p = 0.018 by paired t test) and average weekly PD volume decreased from 28,836 ± 5,699 to 23,872 ± 3,569 mL (p = 0.04 by paired t test) after TVP treatment without concomitant change in dialysate K t/V. In terms of PD menu, we did not change the combination of dialysates through this study even though total PD volume was decreased.
These results indicated that TVP was effective for fluid removal and inhibited dialysis exchange volume.
Many patients undergoing CAPD receive antihypertensive agents, including calcium antagonists. As compared with other drugs, azelnidipine increases drain volume by 13 % [19]. Atrial natriuretic peptide may decrease peritoneal fluid absorption, resulting in a significant increase in peritoneal fluid removal and small solute clearances [20]. In our trial, TVP also increased average UF significantly (Fig. 2). On the other hand, we measured uNa, uK, and PD-Na to evaluate if these parameters could help in understanding the mechanism. However, we do not insist on anything in terms of mechanism with these parameters because there was no difference between before and after TVP treatment (Fig. 3).
Arginine vasopressin exerted a local anti-inflammatory effect on the lung through the V2R in a sepsis model [21]. V2R is expressed only in principal cells of the renal collecting duct system, but not on the vascular endothelium or in vascular smooth muscle [22].
TVP treatment can be effective or ineffective, but it is important to determine its effectiveness in advance. We therefore propose measurement of the us OSM ratio before starting TVP treatment. This ratio, calculated as shown above, reflects the concept that patients in whom TVP treatment is effective should have higher urine OSM than serum OSM, despite congestion with high vasopressin levels. A decrease of >26 % in urine OSM from a baseline of >352 mOsm/L for the first 4–6 h predicts responders to TVP [23]. Differences between urine and serum OSM need to be compensated with serum OSM to exclude confounding of the metrics by dehydration. As shown in Fig. 4, there is correlation between UV and us OSM ratio. Based on a mean UV of 428 mL (Table 1), we determined >400 mL of UV as an effective case. Figure 5 shows that TVP-responsive patients had high us OSM ratios compared with nonresponders, and the ratio decreased after TVP treatment, indicating that free water clearance should be increased with TVP. This also means the ratio is useful for determination of efficiency in advance. We re-evaluated each patient to try to identify other factors affecting response to TVP therapy; however, we could not find any factors other than us OSM ratio for predicting response to TVP in advance.
Our results indicate that TVP is useful for patients with oliguria and high urine OSM undergoing CAPD. Furthermore, we can reduce PD volume to maintain their nutritional status.
References
Chaudhary K, Sangha H, Khanna R. Peritoneal dialysis first: rationale. Clin J Am Soc Nephrol. 2011;6:447–56.
Tjiong HL, Swart R, van den Berg JW, Fieren MW. Amino Acid-based peritoneal dialysis solutions for malnutrition: new perspectives. Perit Dial Int. 2009;29:384–93.
Matsuzaki M, Hori M, Izumi T, Fukunami M. Efficacy and safety of tolvaptan in heart failure patients with volume overload despite the standard treatment with conventional diuretics: a phase III, randomized, double-blind, placebo-controlled study (QUEST study). Cardiovasc Drugs Ther. 2011;25(Suppl 1):S33–45.
Matsue Y, Suzuki M, Seya M, et al. Tolvaptan reduces the risk of worsening renal function in patients with acute decompensated heart failure in high-risk population. J Cardiol. 2013;61:169–74.
Watanabe K, Dohi K, Sugimoto T, et al. Short-term effects of low-dose tolvaptan on hemodynamic parameters in patients with chronic heart failure. J Cardiol. 2012;60:462–9.
Josiassen RC, Curtis J, Filmyer DM, et al. Tolvaptan: a new tool for the effective treatment of hyponatremia in psychotic disorders. Expert Opin Pharmacother. 2010;11:637–48.
Aperis G, Alivanis P. Tolvaptan: a new therapeutic agent. Rev Recent Clin Trials. 2011;6:177–88.
Jones CH, Wells L, Stoves J, et al. Can a reduction in extracellular fluid volume result in increased serum albumin in peritoneal dialysis patients? Am J Kidney Dis. 2002;39:872–5.
Struijk DG, Krediet RT, Koomen GC, et al. The effect of serum albumin at the start of continuous ambulatory peritoneal dialysis treatment on patient survival. Perit Dial Int. 1994;14:121–6.
Blumenkrantz MJ, Gahl GM, Kopple JD, et al. Protein losses during peritoneal dialysis. Kidney Int. 1981;19:593–602.
Ates K, Oztemel A, Nergizoglu G, et al. Peritoneal protein losses do not have a significant impact on nutritional status in CAPD patients. Perit Dial Int. 2001;21:519–22.
Hakemi MS, Golbabaei M, Nassiri A, et al. Predictors of patient survival in continuous ambulatory peritoneal dialysis: 10-year experience in 2 major centers in Tehran. Iran J Kidney Dis. 2010;4:44–9.
Testani JM, Cappola TP, Brensinger CM, et al. Interaction between loop diuretic-associated mortality and blood urea nitrogen concentration in chronic heart failure. J Am Coll Cardiol. 2011;58:375–82.
Nunez J, Nunez E, Minana G et al. Differential mortality association of loop diuretic dosage according to blood urea nitrogen and carbohydrate antigen 125 following a hospitalization for acute heart failure. Eur J Heart Fail. 2012;14(9):974–84.
Hirano T, Yamamura Y, Nakamura S, et al. Effects of the V(2)-receptor antagonist OPC-41061 and the loop diuretic furosemide alone and in combination in rats. J Pharmacol Exp Ther. 2000;292:288–94.
Schrier RW, Gross P, Gheorghiade M, et al. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N Engl J Med. 2006;355:2099–112.
Schweiger TA, Zdanowicz MM. Vasopressin-receptor antagonists in heart failure. Am J Health Syst Pharm. 2008;65:807–17.
Shoaf SE, Bramer SL, Bricmont P, Zimmer CA. Pharmacokinetic and pharmacodynamic interaction between tolvaptan, a non-peptide AVP antagonist, and furosemide or hydrochlorothiazide. J Cardiovasc Pharmacol. 2007;50:213–22.
Suzuki H, Inoue T, Kobayashi K, et al. The newly developed calcium antagonist, azelnidipine, increases drain volume in continuous ambulatory peritoneal dialysis patients. Adv Perit Dial. 2006;22:18–23.
Wang T, Cheng HH, Heimburger O, et al. Intraperitoneal atrial natriuretic peptide increases peritoneal fluid and solute removal. Kidney Int. 2001;60:513–9.
Boyd JH, Holmes CL, Wang Y, et al. Vasopressin decreases sepsis-induced pulmonary inflammation through the V2R. Resuscitation. 2008;79:325–31.
Decaux G, Soupart A, Vassart G. Non-peptide arginine-vasopressin antagonists: the vaptans. Lancet. 2008;371:1624–32.
Imamura T, Kinugawa K, Shiga T, et al. Novel criteria of urine osmolality effectively predict response to tolvaptan in decompensated heart failure patients–association between non-responders and chronic kidney disease. Circ J. 2013;77:397–404.
Acknowledgments
We are very grateful to Medical Engineering staff for assistance with dialysis efficiency and nutrition status.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Iwahori, T., Esaki, M., Hinoue, H. et al. Tolvaptan increases urine and ultrafiltration volume for patients with oliguria undergoing peritoneal dialysis. Clin Exp Nephrol 18, 655–661 (2014). https://doi.org/10.1007/s10157-013-0883-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-013-0883-8