
Abstract
Background
A rare and peculiar glomerulopathy has begun to be recognized in Japan. The Japanese Society of Nephrology has established a research working group and has collected cases from all over Japan in an attempt to understand the complete spectrum of this glomerulopathy.
Method
The diagnostic criterion, which was needed to collect the cases, was proposed as a glomerulopathy showing microspheres or microtubular structures or both associated with podocytic infolding into the glomerular basement membrane (GBM) on electron microscopy. The lesion shows a non-argentaffin hole in the GBM with periodic acid methenamine silver staining and is similar to membranous glomerulonephritis.
Results
Twenty-five cases were collected from 17 institutions. Patients were 20–69 years old (19 women, 6 men). Seventeen patients also had collagen diseases such as lupus nephritis and Sjögren’s syndrome. All patients had proteinuria. Proteinuria showed a remission in 15 of 23 patients within 12 months, but proteinuria remained higher than 1.0 g/day in five patients despite different types of therapy. Podocytic infolding including microspheres showed either positive or negative staining for immunoglobulins. Cluster formation of microspheres was found in 4 of 17 patients with collagen disease, and in five out eight patients without collagen disease. Electron-dense deposits in the GBM were also found in 6 of 17 patients with collagen disease but were not found in eight patients without collagen disease.
Conclusion
Some patients might have a subtype of lupus nephritis, class V, or membranous glomerulonephritis. However, we propose a new disease entity, podocytic infolding glomerulopathy, as a common basis of all 25 patients, because we suspect that microspheres or microtubular structures or both can be derived from podocytic infolding.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recently, we have begun to recognize a rare and peculiar glomerulopathy, in which microspheres or microtubular structure or both are associated with infolding of cytoplasmic processes of podocytes into the glomerular basement membrane (GBM). This type of glomerulopathy is not included in the World Health Organization’s classification of glomerular diseases [1]. We have, as yet, no idea, whether this lesion indicates a new disease entity or a transient morphological finding of a well-known disease. To more clearly understand the clinical and pathological profile, treatment, and prognosis of this glomerulopathy, we need to analyze many cases. However, it was difficult to accumulate many cases of this kind of glomerulopathy in a single institution, because the glomerulopathy is extremely rare. Therefore, the Japanese Society of Nephrology has established a research working group and has collected cases from all over Japan in an attempt to understand the complete spectrum of this glomerulopathy. As a result, 25 cases have been collected from 17 institutions across Japan. We report a summary of the findings and discuss whether a new disease entity should be proposed.
Collection of the patients
The patients were distinguished with ultrastructural studies. The following electron-microscopic finding was proposed as a common tentative criterion, which was needed to collect the cases. On electron microscopy, microspheres or microtubular structures or both are found in association with podocytic infolding into the GBM (Figs. 1, 2). The lesion was designated as podocytic infolding glomerulopathy (PIG). PIG shows a non-argentaffin hole (bubbling or stipple formation) in association with an occasional spike formation on periodic acid methenamine silver (PAM) staining (Fig. 3). Therefore, the light-microscopic findings are similar to those of membranous glomerulonephritis. On electron microscopy, cytoplasmic processes of podocytes infold into the GBM, which involves thickening of the lamina densa. At the end of an infolded cytoplasmic process of a podocyte, microspheres or microtubular structures or both are found (Fig. 4). These microstructures measuring 50–150 nm have a trilaminar limiting membrane structure, which is known as a unit membrane and may be equivalent to a cytoplasmic membrane (Fig. 5). Microspheres can show cluster formation (Fig. 6).

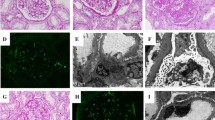
a Electron micrograph of case 19 shows global and diffuse distribution of microstructures in the GBM (×3,000). b The microstructures show microspheres measuring 50–150 nm in diameter (×15,000)

Electron micrograph of case 3 shows microtubular structures with a diffuse distribution measuring 50–100 nm in width (×10,000)

Light microscopy of case 19 shows a non-argentaffin hole (bubbling or stipple formation) in the GBM. Spike formation was not remarkable (PAM stain)

a Electron micrograph of case 21 shows cytoplasmic processes of podocytes infolded into the GBM. At the end of an infolded cytoplasmic process of podocyte, microspheres or microtubular structures or both were found. b The infolded cytoplasmic process of a podocyte went through the middle layer of the GBM, which was accompanied by thickening of the lamina densa (×10,000)

The microspheres of case 19 measuring 50–150 nm in diameter have a trilaminar limiting membrane structure, which is known as a unit membrane (×30,000)

The microspheres of case 23 measuring 40–60 nm in diameter showed a cluster formation (×20,000)
We can classify the podocytic infolding into two categories, such as primary infolding and microstructure in the GBM, by which the finding of podocytic infolding can be more clearly understood. Primary infolding is infolding of the podocytic cytoplasmic process into the GBM. Microstructures in the GBM including microspheres or microtubular structures or both are budding from the primary infolding, which is seen in the GBM. With the combination of primary infolding and microstructures in the GBM, PIG is divided into three types: type A with only primary podocytic infolding, type B with both primary podocytic infolding and microstructures in the GBM, and type C with only microstructures in the GBM (Fig. 7). We can recognize the microstructures in the GBM (type C) as bubbling formation on PAM staining, whereas primary podocytic infolding (type A) corresponds to spike formation on PAM staining.

A diagram of primary podocytic infolding and microstructures in the GBM. Podocytic infolding glomerulopathy was divided into three types: type A with only primary podocytic infolding, type B with both primary and microstructures in the GBM, and type C with only microstructures in the GBM
With these diagnostic criteria for PIG, 25 cases were collected from 17 Japanese institutions. Five cases (case 1, 11, 14, 15, and 17) had previously been reported by Sato et al. [2]. The remaining cases, including case 2 [3], case 3 [3], case 4 [4], case 5 [5], case 6 [6], case 7 [6], case 8 [7], case 9 [8], case 10 [9], case 12 [10], case 13 [11], case 16 [3], case 18 [12], case 19 [13], case 20 [14], case 21 [15], case 22 [16], case 23 [17], case 24 [18], and case 25 [19], correspond to each reference which has been published in this special issue.
The clinical findings analyzed issues included age, sex, grade of proteinuria (g/day) at the time of renal biopsy and at the end of observation, hematuria, serum creatinine level at the time of renal biopsy, blood pressure, treatment, and a concomitant diseases.
The morphological findings analyzed included light-microscopic diagnoses, presence of podocytic infolding, microspheres, clusters of microspheres, microtubules, electron dense deposits in the GBM, GBM thickening, and results of immunostaining (granular pattern at the glomerular peripheral loops).
Results
Clinical profile (Table 1)
The patients ranged in age from 20 to 69 years. The greatest number of patients was in the fourth decade (Fig. 8). Nineteen patients were women, and 6 patients were men. All 25 patients showed proteinuria (<1.0 g/day in six cases, 1.0–2.9 g/day in 13 cases, >3.0 g/day in six cases), and six patients had nephrotic syndrome. Only three patients had microhematuria (more than five erythrocytes per high-power field on light microscopy of urine sediments). Hypertension (systolic blood pressure > 140 mmHg or diastolic blood pressure > 90 mmHg) was present in 7 of 25 patients. Serial measurement of urinary protein levels in 22 patients showed that proteinuria remitted within 12 months in 15 patients and that proteinuria remained higher than 1.0 g/day during the observation period in five patients. Serum creatinine levels were within the normal range in 21 of 25 patients and the remaining four patients showed increased level of serum creatinine levels greater than 1.4 mg/dl, all of whom had hypertension. Prednisolone was administered to 18 patients, three of whom underwent steroid pulse therapy, and immunosuppressants such as cyclosporine A and mycophenolate mofetil were additionally used in three patients. The patients treated with prednisolone included 15 of the 17 patients with collagen disease and three of the eight patients without collagen disease. In 12 of 18 patients, proteinuria decreases with steroid administration. Prednisolone was not used in seven patients, of whom four received no treatment and three received an angiotensin II receptor antagonist or diuretics or both.

Patients ranged in age from 20 to 69 years. The greatest number of patients was in the fourth decade
Concomitant diseases included systemic lupus erythematosus (SLE) in 14 patients, which was combined with Sjögren’s syndrome, hydronephrosis, and Takayasu’s disease in two, three, and one patient, respectively, and Sjögren’s syndrome in four patients, which was combined with SLE, primary biliary cirrhosis, and rheumatoid arthritis in two, one, and one patient, respectively. Mixed connective-tissue disease (MCTD), hypothyroidism due to chronic thyroiditis, hepatitis B virus infection, ovarian mature teratoma, and vesicoureteral reflux (VUR) associated with bilateral hydronephrosis and Basedow’s disease were each present in one patient.
Therefore, the 25 patients can be divided into a group of 17 patients, in whom PIG was associated with a collagen disease (lupus nephritis, Sjögren’s syndrome, rheumatoid arthritis, or MCTD), and eight patients, in whom PIG was associated with non-collagen disease (chronic thyroiditis, hepatitis B virus infection, ovarian mature teratoma, or VUR with Basedow’s disease).
Pathological profile (Table 2)
Tentative light-microscopic diagnoses must be made without using the terminology of PIG. The diagnoses of a primary glomerulonephritis included membranous nephropathy (stage 2–3) in four patients and focal segmental glomerulosclerosis (FSGS) with bubbling in the GBM in four patients. The diagnoses of a secondary glomerulonephritis included lupus nephritis in 12 patients (class 1 in one patient, class II in four patients, and class V in seven patients). In four patients who had clinical diagnoses of Sjögren’s syndrome, light-microscopic diagnoses included minor glomerular abnormality (MGA) in three patients and membranoproliferative glomerulonephritis (MPGN) type 3 in one patient. One patient of MCTD showed MGA.
On electron microscopy, podocytic infolding was seen in all 25 patients, of whom four patients (patients 16, 19, and 20, and 21) showed mild primary podocytic infolding but prominent microstructures in the GBM. Microspheres were present in 24 of 25 patients, of whom nine patients showed cluster of microspheres. Clusters of microspheres were found in four of 17 patients with collagen disease and in five of eight patients without collagen disease. Microtubular structures in the GBM were present in 14 of 25 patients, of whom 13 patients also showed microspheres. Thickening of the GBM, especially in the lamina densa, was seen in 24 of 25 patients. In patients with collagen disease-associated PIG, amorphous electron-dense deposits suggesting immune complex deposition as seen in membranous glomerulonephritis, were found in the mesangial area in 17 patients. However, in addition to the deposition in the mesangial area, electron-dense deposits were also found in the GBM co-localized with podocytic infolding in six of 17 patients. On the other hand, in patients with collagen disease-irrelevant PIG, electron-dense deposits could not be found in the GBM nor in the mesangial area.
On immunological studies, immunoglobulins and complements were all negative along the glomerular capillary loops in seven patients, including five of 17 patients with collagen disease-associated PIG and two of eight patients with collagen disease-irrelevant PIG. Only IgG was positive in six patients, including one patient who showed hepatitis B virus surface antigen (HBVs). Four patients were positive for IgG, IgA, C3, and C1q; 2 for IgG, IgA, IgM, and C3; 2 for IgG, IgM, and C1q, 1 for IgG, IgA, and C3, and 2 for IgG and IgA, or IgM or both. IgM only was positive in one patient. There was no apparent difference in the mode of immunoglobulin deposition between collagen disease-associated PIG and collagen disease-irrelevant PIG. Podocytic infolding including microstructures in the GBM showed either positive or negative staining for immunoglobulins.
Discussion
Twenty-five patients were divided into a group with collagen disease-associated PIG and a group with collagen disease-irrelevant PIG. In the former group, differentiation from lupus nephritis, class V should be discussed, because 14 of 17 patients had SLE. In this group, in addition to the electron-dense deposition in the mesangial area, electron-dense deposits were also found in the GBM in six of 17 patients, whereas no electron-dense deposits were found in patients with collagen disease-irrelevant PIG. Electron-dense deposits are supposedly positive for immunoglobulins and complement. It was true that the patients who showed electron-dense deposits in the GBM (patients 4, 8, 10, 11, 12, and 15), showed IgG or other immunoglobulins or both and complement on the glomerular peripheral loops. However, the patients who showed no dense deposits but only podocytic infolding lesion were divided into a group positive for immunoglobulins or complements or both and a group negative for all immunoglobulins and complement. These findings suggest that some cases of collagen disease-associated PIG are not distinct from a variant of lupus nephritis, class V. In other words, lupus nephritis, class V can makes the transition to PIG. However, how PIG can combine with lupus nephritis in only a very small population is unclear.
In patients with collagen disease-irrelevant PIG, no electron-dense deposits were found in the GBM. However, light-microscopic diagnoses included membranous glomerulonephritis with positive immunoglobulins or complement or both in the glomerular peripheral loops and focal segmental glomerulosclerosis (FSGS) without staining for immunoglobulins. A differentiation of PIG from membranous nephropathy is to be discussed. Primary podocytic infolding (type A in Fig. 7) can also be found in membranous nephropathy stage 2 or stage 3 together with a reaction of the basement membrane surrounding electron-dense deposits (Fig. 9a, b) and in some cases of minimal change nephrotic syndrome [20]. Therefore, primary podocytic infolding alone cannot be a critical finding for differentiation. Microstructures in the GBM such as microspheres or microtubular structures or both(type B and type C in Fig. 7) are usually not found in membranous nephropathy excepting granular and membranous debris in stage 3 membranous nephropathy [21, 22] and in rare cases of HBV-associated glomerulonephritis [21, 23]. From this point of view, our patient 23 (Fig. 6), who was positive for HBV antigens might have a variant of membranous glomerulonephritis. Fourteen patients with clustered microspheres in the GBM have recently been reported [24]. The morphological characteristics have been described as cluster formation of spherular structures in the subepithelial space with an average diameter of 84.5 nm and electron lucent core associated with a targetoid appearance, which shows morphological similarity to nuclear pore complexes. However, the spherular structure was negatively stained with antinuclear pore antibody and antineutral endopeptidase (NEP) (CD 10) antibody. Membranous nephropathy with microspheres has also been reported in a male infant whose mother had a deficiency of NEP and had become immunized against the antigen before delivery [25]. These two reports considered the glomerulopathy to be a subtype of membranous glomerulonephritis. Our patient 22 showed a primary podocytic infolding, around the tip of which clusters of the microspheres could be seen in the GBM (Fig. 10a). The glomeruli were strongly positive for all immunoglobulins and complement. The distribution of clustered microspheres distributed was mainly from the subepithelial space to the middle layer of the lamina densa in the GBM, similar to that of membranous glomerulopathy, stage 2 (Fig. 10b). Therefore, this case can be also interpreted as a subtype of membranous glomerulonephritis. In fact, there was a case of membranous glomerulonephritis that showed microspheres in limited parts of the electron dense deposits (Fig. 11). On the other hand, microspheres with or without cluster formation, in type B and type C of some cases of PIG showed positive staining with anti-human immunoglobulins or complement or both antibodies. From this point of view, it may be difficult to discriminate immunoglobulin-positive PIG from a subtype of membranous glomerulonephritis. However, we can say that a subtype of membranous glomerulonephritis shows clusters of microspheres mainly in the subepithelial space of the GBM, which is strongly positive for immunoglobulins and complement. Meanwhile, more than half of the cases of the PIG did not show cluster formation and microspheres distributed throughout the GBM, but did not confine in the subepithelial space. Moreover, in patients with collagen disease-irrelevant PIG who did not show electron-dense deposits but show only microspheres in the GBM, glomerular peripheral loops were either negative or positive for immunoglobulins. Likewise in patients with collagen disease-associated PIG without electron dense deposits in the GBM, glomerular capillary loops were either positive or negative for immunoglobulins. Why PIG can be either positive or negative for immunoglobulins is unknown. At least, collagen disease-irrelevant PIG showing FSGS with negative staining for immunoglobulins can be clearly differentiated from a subtype of membranous nephropathy.

Electron micrograph of membranous glomerulonephritis stage 2 (a) and stage 3 (b). Primary podocytic infolding type A (Fig. 7) can be found also in membranous nephropathy stage 2 and stage 3 (arrows) (×10,000)

a Electron micrograph of case 22 shows a primary podocytic infolding, around the tip of which clusters of the microspheres measuring 50–70 nm can be seen in the GBM (×30,000). b The clustered microspheres distributed mainly from the subepithelial space to the middle layer of the lamina densa in the GBM. A distribution of clustered microspheres is similar to a distribution of electron-dense deposits of membranous glomerulopathy, stage 2 (×3,000)

Primary membranous glomerulonephritis, stage 2 in a 70-year-old man shows microspheres in a limited part of an electron-dense deposit (arrow) (×10,000)
Villous cytoplasmic protrusion of endothelial cells into the GBM and of mesangial cells into the mesangial matrix were also found in patients with PIG. Therefore, some intramembranous microstructures can be derived from the protruded cytoplasm of endothelial cells or mesangial cells or both. However, these villous protrusions were found in limited areas but were not a generalized manifestation, whereas the distribution of podocytic infolding was diffuse and global, and was not limited to a segmental part of the GBM. Therefore, it is conceivable that most microspheres or microtubules or both can be derived from podocytes. These findings support to use the term of podocytic, but not endothelial or mesangial, infolding glomerulopathy.
The pathogenic mechanism of PIG is unknown. Hydronephrosis was found in three of 25 patients. However, no study has shown that experimental hydronephrosis can induce podocytic infolding. Nakajima et al. [26] have used immune electron microscopy to analyze extracellular organized structures from various kinds of glomerular diseases. The organized structures were divided into microspherical structures and thread-like structure. C1s, C3d, and C9 but not IgA, IgG, fibrinogen, C1q, C1r, C3c, C4, or C5 were localized to individual membrane-like structures of both microspherical and thread-like structures. Higlais et al. [27] performed an immunohistochemical study of complement C5b-9 complexes in several human kidney diseases and have shown positive reactions on round extracellular particles and on striated membranous structures in the GBM. Therefore, the mechanism of podocytic infolding might be related to the role of special types of complement activation in situ on the microstructures [27]. Burkholder et al. have reported 55 cases in which extracellular spherical microparticles (SMPs) were found in the GBM among 1,400 renal biopsies [28]. The SMPs usually formed clusters in the extracellular matrix and have a mean size of 50–58 nm. A viral origin of SMPs was suspected in some cases. However, most SMPs were considered to be non-viral, perhaps particles discharged from cells during glomerular injury or spherical lipoprotein crystalline bodies. However, reported SMPs seemed to be heterogeneous and included tight aggregations of SMPs beneath portions of podocytes, subepithelial loose clusters of SMPs with a lucent core, and intramembranous clusters of SMPs. At least, tight aggregations of SMPs beneath podocytes as shown in Fig. 12 can be distinguished from the PIG of the present study because the aggregation can be usually found in limited, specific areas, where glomerular capillary tufts come close together with back-to-back contact of podocytes (Fig. 12). Moreover, the authors did not mention podocytic infolding as an origin of SMP. We emphasize that microspheres or microtubular structures or both of PIG can be derived by budding from the cell membrane of primary podocytic infolding tips, partially by breaking off from disintegrated podocytic cell processes and drifting into the GBM. Thickening of the GBM containing microspheres might be caused by a loss of balance between biosynthesis and degradation of the matrix of the podocytes.

Electron micrograph of IgA nephropathy in 41-year-old man. Tight aggregation of SMPs beneath podocytes can be distinguished from the PIG of the present study, because the aggregation can usually be found in a specific, limited area, where glomerular capillary tufts come close together with back-to-back contact of the podocytes (×10,000)
In conclusion, we propose a new disease entity, podocytic infolding glomerulopathy, as a common basis of all 25 patients, because we suspect that microspheres or microtubular structures or both can be derived from primary podocytic infolding.
References
Word Health Organization. Section 1. Classification of Glomerular Diseases. Glossary of Terms. In: Churg J, Bernstein J, Glassock RJ, editors. Renal disease classification and atlas of glomerular diseases. 2nd ed. Tokyo: Igaku-Shoin; 1995. p. 3–26.
Sato H, Saito T, Yoshinaga K. Intramembranous fine deposit disease associated with collagen disorder: a new morphological entity? Virchows Arch A Pathol Anat Histopathol. 1992;420:447–51.
Sugiyama H, Maruyama M, Morinaga H, Inoue T, Takiue K, Kikumoto Y, et al. Unique microstructures and podocytic infolding in glomerular basement membrane associated with collagen diseases: a report of three cases.Clin Exp Nephrol. 2008, doi:10.1007/s10157-008-0098-6.
Sato M, Kogure T, Kanemitsu M. A case of systemic lupus erythematosus showing invagination of the podocyte into the glomerular basement membrane: an electron microscopic observation of a repeated-renal biopsy. Clin Exp Nephrol. 2008, doi:10.1007/s10157-008-0091-0.
Kitazawa K, Joh K, Akizawa T. A case of lupus nephritis coexisting with podocytic infolding associated with Takayasu’s arteritis. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0094-x.
Jinguuji Y, Nukui I, Wakasugi M, Yamashita H. Two cases of systemic lupus erythematosus complicated by hydronephrosis and unique small structures observed in the glomerular basement membrane. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0092-z.
Fujigaki Y, Muranaka Y, Sakakima M, Ohta I, Sakao Y, Fujikura T, et al. Analysis of intra-GBM microstructures in a SLE case with glomerulopathy associated with podocytic infolding. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0095-9.
Miura N, Mori Y, Yoshino M, Suga N, Kitagawa W, Yamada H, et al. Membranous nephropathy (bubbling appearance and spike formation) without immunoglobulin deposition in a patient with systemic lupus erythematosus. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0096-8.
Mii A, Shimizu A, Masuda Y, Ishizaki M, Sato S, Hara K, et al. A case of lupus nephritis with diffuse podocytic infolding 5 into the glomerular basement membrane. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0097-7.
Tanaka M, Watanabe K, Asahi K, Katoh T, Watanabe T. Lupus nephritis with podocytic infolding and intramembranous microstructures. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0090-1.
Koike K, Utsunomiya Y, Ito Y, Tokudome S, Miyazaki Y, Suzuki T, et al. A case of glomerulopathy showing podocytic infolding in association with Sjo¨gren’s syndrome and primary biliary cirrhosis. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0093-y.
Matsuo T, Kobayashi Y, Nemoto N, Sano T, Kamata K, Shigematsu H. A nephrotic case of vesicoureteral reflux representing focal segmental glomerulosclerosis associated with podocytic infolding lesions. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0086-x.
Arifa N, Nakashima Y, Yan Z, Le VT, Taguchi T, Nishioka K, et al. Unusual glomerulopathy with atypical thickening of glomerular basement membrane and intramembranous microparticles. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0103-0.
Inoue Y, Kanda Y, Kinoshita C, Kanda C. Intramembranous microspherical structures in focal segmental glomerulosclerosis:a case report. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0101-2.
Yamada S, Masutani K, Katafuchi R, Fujigaki Y, Muranaka Y, Tsuruya K, et al. Focal segmental glomerulosclerosis with intramembranous vesicle-like microstructures and podocytic infolding lesion. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0088-8.
Nomura S, Inoue-Kiyohara M, Oosugi K, Ishikawa E, Obe T, Horiki T, et al. Unusual glomerulopathy with aggregated subepithelial microspheric particles resembling membranous nephropathy: a variant of glomerulopathy associated with podocytic infolding? Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0089-7.
Nishi S, Imai N, Saito T, Ueno M, Arakawa M, Oota T, et al. A nephropathy presenting the microparticles in the glomerular basement membrane in a patient of hepatitis B viral infection. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0087-9.
Yoshimura K, Joh K, Kitamura H, Takahashi Y, Yokote S, Kasai K, et al. A case report of glomerulopathy-associated podocytic infolding 5 in a patient with tumor lysis syndrome. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0099-5.
Masuda Y, Mii A, Shimizu A, Fujita E, Aki K, Ishikawa K, et al. Invagination and infolding of podocytes in glomerular basement membrane in the cases of primary membranous nephropathy. Clin Exp Nephrol. 2008. doi:10.1007/s10157-008-0100-3.
Fujigaki Y, Kobayashi S, Nagase M, Honda N, Otawara Y, Tajima A, et al. Indentation of the glomerular basement membrane in cases with minor abnormalities. J Clin Microscopy. 1987;20:5–6.
Schwartz MM. Membranous glomerulonephritis. In: Jeannette JC, Olson JL, Schwartz MM, Silva FG, editors. Heptinstall’s Pathology of the Kidney. 6th ed. Philadelphia: Lippincott/Williams &Wilkins; 2007. p. 205–51.
D’Agati, Jennette JC, Silva FG. 7. Membranous glomerulopathy. In: King DW, editor. Atlas of Nontumor Pathology. 1st Series, Fascicle 4. Non-Neoplastic Kidney Diseases. American Registry of pathology, Armed Forces Institute of Pathology. Silver Spring: ARP Press; 2005. pp 161–188.
Venkataseshan VS, Lieberman K, Kim DU, Thung SN, Dikman S, D’Agati V, et al. Hepatitis-B-associated glomerulonephritis: pathology, pathogenesis, and clinical course. Medicine (Baltimore). 1990;69:200–16.
Kowalewska J, Smith KD, Hudkins KL, Chang A, Fogo AB, Houghton D, et al. Membranous glomerulopathy with spherules: an uncommon variant with obscure pathogenesis. Am J Kidney Dis. 2006;47:983–92.
Debiec H, Guigonis V, Mougenot B, Haymann J-P, Bensman A, Deschenes G, et al. Antenatal membranous glomerulonephritis with vascular injury induced by anti-neutral endopeptidase antibodies: toward new concepts in the pathogenesis of glomerular diseases. Am Soc Nephrol. 2003;14:27–32.
Nakajima M, Hewitson TD, Mathews DC, Kincaid-Smith P. Localization of complement components in association with glomerular extracellular particles in various renal diseases. Virchows Arch A Pathol Anat. 1991;419:267–72.
Hinglais N, Kazatchkine ND, Bhakdi S, Appay M-D, Mandet C, Grossetete J, et al. Immunohistochemical study of the C5d-9 complex of complement in human kidneys. Kidney Int. 1986;30:399–410.
Burkholder PM, Hyman LR, Barber TA. Extracellular cluster of spherical microparticle in glomeruli in human renal glomerular disease. Lab Invest. 1973;28:415–25.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Joh, K., Taguchi, T., Shigematsu, H. et al. Proposal of podocytic infolding glomerulopathy as a new disease entity: a review of 25 cases from nationwide research in Japan. Clin Exp Nephrol 12, 421–431 (2008). https://doi.org/10.1007/s10157-008-0104-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-008-0104-z