
Abstract
Aim
To validate Liano score as a prognostic scoring system in acute renal failure (ARF): a prospective study in Indian patients.
Patients and methods
Prospective study including 100 patients over a period of 1 year, from March 2006 to July 2007. Inclusion criteria were patients with no previous renal disease or any systemic disease known to affect the kidney and who presented with acute rise (hours to days) in serum creatinine. Exclusion criteria were patients with preexisting chronic renal failure, age younger than 12 years and ultrasound of the abdomen showing contracted kidneys.
Results and conclusions
In this study there were 68 males and 32 females. Peak incidence by age was in the fifth decade. There was no increased mortality in any age group (p = 0.278). A total of 19 patients had pre-renal ARF, 74 patients had intrinsic ARF, of which 46 were acute tubular necrosis (ATN); 7 patients had obstructive ARF. A total of 21 patients had Liano score greater than 0.9, of which 18 patients died and 3 were discharged against medical advice in a critical condition (and died later at home). Calculated sensitivity was 62.1%, specificity was 100% and positive predictive value was 100%. Sensitivity and specificity when calculated separately for intrinsic renal ARF (after excluding post renal ARF) were 60.7% and 100%, respectively. There was statistically significant correlation between Liano score and mortality (p < 0.001).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute renal failure (ARF) is a common problem affecting critically ill patients; the mortality of ARF has remained high, reaching 80% in intensive care unit (ICU) settings [1–7]. There are several confounding factors involved in the comparison of clinical studies in ARF patients: use of different definitions of ARF [8], study design, different evaluated outcomes [8], heterogeneity of patients [9] and associated therapies. A number of factors have been suggested as influencing prognosis based upon correlation with either good or poor outcome [8, 9]. For heterogeneous populations of ICU patients, several severity scoring systems have been widely accepted and used in multicentric clinical trials to confirm successful randomization [12–17]. An ideal prognostic scoring system should be simple and should test a limited number of clinical variables for easy and wide clinical utility.
Fernando Liano and Julio Pascual suggested that several clinical conditions, assisted respiration, hypotension, oliguria, coma and jaundice have a detrimental effect on outcome. Previous health status, premorbid illnesses and age also seem to affect the outcome [18–21].
The beginning and ending supportive therapy for the kidney (BEST Kidney) study [22], which included more than 1,700 patients from 54 centers, tested and compared six scoring systems; in their international sample, none of these had an area under receiver operating characteristics (ROC) curve above the conventional threshold of 0.7 that is typically considered satisfactory for clinical use. Among the scoring systems the group tested, they found the Liano score to have the best discrimination and calibration [22]. The study described herein was conducted with the aim of validating the Liano score in ARF (irrespective of etiology) in Indian patients.
Patients and methods
The study was done prospectively on 100 consecutive patients diagnosed with ARF and admitted to Kasturba Hospital, Manipal between March 2006 and July 2007.
Inclusion criteria
Patients with no previous renal disease or any systemic disease known to affect the kidney and who presented with acute rise (hours to weeks) in serum creatinine were included in the study.
Exclusion criteria
The exclusion criteria for the study were:
-
1.
Patients with acute on chronic renal failure
-
2.
Age younger than 12 years
-
3.
Ultrasound showing grossly contracted kidneys (size ≤80 mm).
Liano score
Liano score was determined using the formula
Probability of death = 0.032 (age in decades) − 0.086 (sex) − 0.109 (nephrotoxic) + 0.109 (oliguria) + 0.116 (hypotension) + 0.122 (jaundice) + 0.150 (coma) − 0.154 (consciousness) + 0.182 (assisted respiration) + 0.210.
A score of 1 was ascribed for the presence, and a score of 0 for the absence, of the following non-numerical clinical parameters in the Liano score:
-
1.
Sex: male
-
2.
Nephrotoxic: use of nephrotoxic drugs, presence of pigmenturia, hemoglobinuria or rhabdomyolysis
-
3.
Oliguria: 24-h urinary volume <400 ml
-
4.
Hypotension: systolic blood pressure <100 mmHg for 8 h with or without ionotropes
-
5.
Jaundice: clinically jaundiced or total bilirubin more than 2.0 mg%
-
6.
Coma: Glasgow coma score less than or equal to 5.
Statistics
Statistical analysis was done using the chi-square test, and receiver operating characteristics curves were applied to assess the predictive power of the score.
Observation and results
The present study included 100 consecutive patients with ARF admitted to Kasturba Hospital, Manipal between March 2006 and July 2007.
Peak incidence by age was in the fifth decade. Mean age was 46.78 years with a standard deviation (SD) of 16.58 years. There was no increased mortality in any age group (p = 0.278).
There were 68 males and 32 females. There was no significant correlation between sex and mortality (p = 0.629).
Of the 100 patients, 70 had medical, 26 surgical and 4 obstetric causes for ARF. Nineteen patients had pre-renal, 74 had renal and 7 had post-renal causes for the ARF (Table 1). The single commonest cause for ARF in this study was post-ischemic acute tubular necrosis (ATN) (46 patients). There were 58 patients with nonoliguric renal failure and 42 patients with oliguric renal failure. A total of 12 patients with nonoliguric renal failure and 22 with oliguric renal failure died, suggesting a statistically significant better outcome in the nonoliguric group (p = 0.003). Most patients with ARF could be managed with conservative measures with emphasis on rigorous fluid and electrolyte management. A total of 36 patients required dialysis, 2 cases needed continuous renal replacement therapy (CRRT) and the remaining 62 were managed conservatively. Of the 36 patients who underwent dialysis 72.2% had complete recovery whereas 19.4% died. Number of dialysis sessions did not have a bearing on mortality. Survival rate among the patients who were managed conservatively was 64.5%.
The complications seen in this study group were encephalopathy (45 patients), sepsis (30 patients), pulmonary edema (27 patients), upper and lower gastrointestinal (GI) bleeding (8 patients) and cardiac arrhythmias (7 patients). Electrolyte and acid-base abnormalities were very frequently encountered.
Overall mortality in this prospective cohort of 100 patients was 29%. The main causes for mortality were sepsis (11 patients) and acute respiratory distress syndrome (13 patients).
A total of 21 patients had Liano score greater than 0.9, of whom 18 patients died and 3 were discharged against medical advice in a critical condition (and died at home later). There was statistically significant correlation between Liano score and mortality, with p value ≤0.001 (Tables 2 and 3) and Liano score showed statistical significance even when obstructive causes were excluded (Table 4).
Discussion
In the present study, we included 100 consecutive patients with ARF (irrespective of etiology) admitted to Kasturba Hospital, Manipal between March 2006 and July 2007. There was no increased mortality in any age group nor was there any sex predilection.
There were 17 patients diagnosed with leptospirosis. Since the year 2000, we have witnessed a steady increase in the incidence of leptospirosis in patients referred to our hospital. A similar trend is seen all along the Western coastal belt of Peninsular India. Electrolyte imbalances and acid-base imbalances are almost universal in the cohort, as is anticipated in ARF. The incidence of drug-induced ARF was lower than in other series.
Patients diagnosed as having post-renal ARF fared best, with recovery almost certain after the organic obstruction was cleared. Intermittent hemodialysis was the intervention of choice in 36 patients, with a 72.2% survival rate. The survival rate among the patients who were managed conservatively was 64.5%. Overall mortality was 29%, with sepsis and pulmonary edema being the commonest causes of mortality.
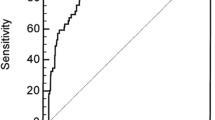
Liano score showed good discrimination for mortality with a cutoff of 0.9. When we reduced the cutoff to 0.8, the score performed satisfactorily. The area under the ROC curve was 0.992. As with all earlier studies relating to ARF-specific prognostic scoring systems, we also found excellent positive predictive value for the Liano score. The area under the ROC curve was also superior to other reported series.
The BEST Kidney study [22] with more than 1,700 patients from 54 centers in 23 countries tested and compared six scoring systems; in their international sample none of the tested systems had an area under the ROC curve above the conventional threshold of 0.7 that is typically considered satisfactory for clinical use.
Among the scoring systems tested in the BEST Kidney study, the Liano score showed the best discrimination and calibration. This finding is consistent with a previous study by Douma et al., who tested seven general and four ARF-specific scoring systems with their database. This study included 238 patients who received their first dialysis for ARF in the ICU. These authors also reported that the Liano score had the highest area under the ROC curve (0.78) among the four ARF-specific scores and that the observed mortality rate closely followed that predicted by the Liano score.
The Stuivenberg Hospital, Nephrology-Hypertension Antwerp and the Faculty of Medicine, University of Antwerp proposed the original SHARF score; the subsequent modified SHARF 2 score added three parameters: serum bilirubin, sepsis and hypotension [23]. The proposal of the acute dialysis qualitative index in 2004 resulted in classifying ARF in a system called RIFLE (risk, injury, failure, loss of kidney function and end-stage renal disease).
RIFLE class is determined based on the worst of either GFR criteria or urine output [24].
Perhaps the best scoring system is the one developed by Liano et al. The tool was initially obtained by retrospectively obtained data and has been validated prospectively.
The correlation between probability of death obtained with equations from the initial phase applied to control patients and real evolution of these patients, survival and death was excellent.
Liano et al. established a cutoff point of the discriminative score above which no patient survived (cutoff 0.9, specificity 100%, positive predictive value 100%).
It remains to be seen if these results hold true when external validation is attempted in larger series of patients. To our knowledge, this is the first attempt in India to use the Liano score to assess outcome in patients with ARF.
Conclusions
-
1.
Age (p = 0.278), sex (p = 0.629) and presence of jaundice (p = 0.091) do not have a significant correlation with mortality.
-
2.
There was a statistically significant correlation between exposure to nephrotoxic agents and mortality (p = 0.017), presence of anuria/oliguria and mortality (p = 0.001), presence of hypotension and mortality (p < 0.001), presence of coma and mortality (p < 0.001) and need for ventilation and mortality (p < 0.001).
-
3.
The outcome of patients with ARF is poor. Hospital mortality is 29% and another 5% of patients were discharged against medical advice in a critical condition. (The clinical condition at the time of discharge makes survival improbable.)
-
4.
Liano scoring in this study identified 21 patients with a score ≥0.9, all of whom died. Statistical significance was achieved between Liano score and mortality (p < 0.001) when a cutoff of Liano score 0.9 was chosen. Calculated sensitivity was 62.1%, specificity was 100% and positive predictive value was 100%.
-
5.
Statistical significance was also achieved (p < 0.001) when the cutoff Liano score was lowered to 0.8. Only 1 out of 29 patients with a Liano score above 0.8 (i.e., 0.82) survived. Calculated sensitivity was 82.4%, specificity was 98.5% and positive predictive value was 96.5%.
-
6.
Liano score was also calculated after excluding obstructive causes and was found to be statistically significant.
-
7.
This suggests that the ARF-specific severity-of-illness Liano score is a very reliable indicator of mortality in patients diagnosed with ARF.
References
Nolan CR, Anderson RJ. Hospital-acquired acute renal failure. J Am Soc Nephrol. 1998;9:710–8.
McCarthy JT. Prognosis of patients with acute renal failure in the intensive-care unit: a tale of two eras. Mayo Clin Proc. 1996;71:117–26.
Brivet FG, Kleinknecht DJ, Loirat P, Landais PJ. Acute renal failure in intensive care units–causes, outcome, and prognostic factors of hospital mortality; a prospective, multicenter study. French study group on acute renal failure. Crit Care Med. 1996;24:192–8.
Hamel MB, Phillips RS, Davis RB, Desbiens N, Connors AF Jr, Teno JM, et al. Outcomes and cost-effectiveness of initiating dialysis and continuing aggressive care in seriously ill hospitalized adults. SUPPORT investigators. Study to understand prognoses and preferences for outcomes and risks of treatments. Ann Intern Med. 1997;127:195–202.
MacKay K, Moss AH. To dialyze or not to dialyze: an ethical and evidence-based approach to the patient with acute renal failure in the intensive care unit. Adv Ren Replace Ther. 1997;4:288–96.
Groeneveld AB, Tran DD, van der Meulen J, Nauta JJ, Thijs LG. Acute renal failure in the medical intensive care unit: predisposing, complicating factors and outcome. Nephron. 1991;59:602–10.
Sural S, Sharma RK, Singhal MK, Kher V, Gupta A, Arora P, et al. Acute renal failure in an intensive care unit in India—prognostic factors and outcome. J Nephrol. 1999;12:390–4.
Ahlström A, Kuitunen A, Peltonen S, Hynninen M, Tallgren M, Aaltonen J, et al. Comparison of 2 acute renal failure severity scores to general scoring systems in the critically ill. Am J Kidney Dis. 2006;48:262–8.
Uchino S, Bellomo R, Morimatsu H, Morgera S, Schetz M, Tan I, et al. Beginning and ending supportive therapy for the kidney (B.E.S.T. Kidney) investigators. External validation of severity scoring systems for acute renal failure using a multinational database. Crit Care Med. 2005;33:1961–7.
Liaño F, Gallego A, Pascual J, García-Martín F, Teruel JL, Marcén R, et al. Prognosis of acute tubular necrosis: an extended prospectively contrasted study. Nephron. 1993;63:21–31.
Schäfer JH, Maurer A, Jochimsen F, Emde C, Wegscheider K, Arntz HR, et al. Outcome prediction models on admission in a medical intensive care unit: do they predict individual outcome? Crit Care Med. 1990;18:1111–8.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
Le Gall JR, Lemeshow S, Saulnier F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270(24):2957–63. Erratum in: JAMA 1994;271:1321.
Lemeshow S, Le Gall JR. Modeling the severity of illness of ICU patients. A systems update. JAMA. 1994;272:1049–55.
Auriant I, Vinatier I, Thaler F, Tourneur M, Loirat P. Simplified acute physiology score II for measuring severity of illness in intermediate care units. Crit Care Med. 1998;26:1368–71.
Maher ER, Robinson KN, Scoble JE, Farrimond JG, Browne DR, Sweny P, et al. Prognosis of critically-ill patients with acute renal failure: APACHE II score and other predictive factors. Q J Med. 1989;72:857–66.
Beck DH, Taylor BL, Millar B, Smith GB. Prediction of outcome from intensive care: a prospective cohort study comparing acute physiology and chronic health evaluation II and III prognostic systems in a United Kingdom intensive care unit. Crit Care Med. 1997;25:9–15.
Liaño F, Gallego A, Pascual J, García-Martín F, Teruel JL, Marcén R, et al. Prognosis of acute tubular necrosis: an extended prospectively contrasted study. Nephron. 1993;63:21–31.
Liaño F, Pascual J. Acute renal failure, critical illness and the artificial kidney: can we predict outcome? Blood Purif. 1997;15:346–53.
Liaño F. Severity of acute renal failure: the need of measurement. Nephrol Dial Transplant. 1994;9 Suppl 4:229–38.
Liaño F, Pascual J. Epidemiology of acute renal failure: a prospective, multicenter, community-based study. Madrid Acute Renal Failure Study Group. Kidney Int. 1996;50:811–8.
Uchino S, Bellomo R, Kellum JA, Morimatsu H, Morgera S, Schetz MR, et al. Beginning and ending supportive therapy for the kidney (B.E.S.T. Kidney) investigators writing committee. Patient and kidney survival by dialysis modality in critically ill patients with acute kidney injury. Int J Artif Organs. 2007;30:281–92.
Lins RL, Elseviers MM, Daelemans R, Arnouts P, Billiouw JM, Couttenye M, et al. Re-evaluation and modification of the Stuivenberg Hospital acute renal failure (SHARF) scoring system for the prognosis of acute renal failure: an independent multicentre, prospective study. Nephrol Dial Transplant. 2004;19:2282–8. Epub 2004 July 20.
Abosaif NY, Tolba YA, Heap M, Russell J, El Nahas AM. The outcome of acute renal failure in the intensive care unit according to RIFLE: model application, sensitivity, and predictability. Am J Kidney Dis. 2005;46:1038–48.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Varricatt, V.P., Rau, N.R., Attur, R.P. et al. Validation of Liano score in acute renal failure: a prospective study in Indian patients. Clin Exp Nephrol 13, 33–37 (2009). https://doi.org/10.1007/s10157-008-0073-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-008-0073-2