
Abstract
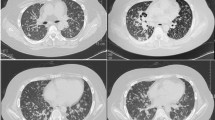
A 23-year-old man with no recent medical history was hospitalized complaining of high fever and cough. In addition to very marked eosinophilia, chest X-ray revealed extensive bronchovascular bundle thickening. Transbronchial lung biopsy (TBLB) showed moderate eosinophil infiltration. Cryptococcus neoformans infection was diagnosed, based on blood culture, cerebrospinal fluid culture, urine culture, and lung biopsy specimens. The eosinophilia was successfully alleviated by treatment for cryptococcal meningitis. Furthermore, cryptococcal sepsis resolved with amphotericin B and 5-flucytosine treatment. Eosinophilia commonly occurs following chronic Aspergillus infection, but the present case suggests the involvement of Cryptococcus in another mechanism for eosinophilia.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Diamond RD. Cryptococcosis. In: Maddell GE, Benett JE, Dolin R, editors. Mandell, Douglas, Bennett’s principles and practice of infectious diseases, vol 2. 5th ed. Philadelphia: Churchill Livingstone; 2000. p. 2707–2718.
Doutsu Y, Masaki M, Masuyama Y, Yamashita K, Oka M, Koga H, et al. Clinical and therapeutic studies in 11 cases of primary pulmonary cryptococcosis. Nihon Kyobu Shikkan Gakkai Zassi 1987;25:229–239.
Marwaha RK, Trehan A, Jayashree K, Vasishta RK. Hypereosinophilia in disseminated cryptococcal disease. Pediatr Infect Dis J 1995;14:1102–1103.
Starr JC, Che H, Montgomery J. Cryptococcal pneumonia simulating chronic eosinophilic pneumonia. South Med J 1995;88:845–846.
Tanaka H, Urase F, Hasegawa K, Tsubaki K, Irimajiri K, Horiuchi A, et al. Sarcoidosis with severe eosinophlia due to cryptococcus infection. Rinsho Ketsueki 1988;29:208–213.
Yamamoto T, Tanida T, Ueta E, Kimura T, Doi S, Osaki T. Pulmonary infiltration with eosinophilia (PIE) syndrome induced by antibiotics, PIPC and TFLX during cancer treatment. Oral Oncol 2001;37:471–475.
Ohnishi H, Abe M, Yokoyama A, Hamada H, Ito R, Hirayama T, et al. Clarithromycin-induced eosinophilic pneumonia. Intern Med 2004;43:231–235.
Ii T, Doutsu Y, Ashitani J, Taniguchi H, Mizuta M, Toshimori H, et al. A case of loxoprofen-induced pulmonary eosinophilia. Nihon Kyobu Shikkan Gakkai Zassi 1992;30:926–929.
Slavin RG, Fisher VW, Levine EA, Tsai CC, Winzenburger P. A primate model of allergic bronchopulmonary aspergillosis. Int Arch Allergy Appl Immunol 1978;56:325–333.
Ray D, Sara K, Date A. Raised serum IgE levels in chronic inflammatory lung diseases. Ceylon Med J 1995;40:14–18.
Traynor TR, Kuziel WA, Toews GB, Huffnagle GB. CCR2 expression determines T1 versus T2 polarization during pulmonary Cryptococcus neoformans infection. J Immunol 2000;164:2021–2027.
Stone BD, Wheeler JG. Disseminated cryptoccocal infection in a patient with hyperimmunoglobulinemia E syndrome. J Pediatr 1990;117:92–95.
Garty BZ, Wolach B. Cryptoccocal meningitis in a child with hyperimmunoglobulin E syndrome. Pediatr Allergy Immunol 1995;6:175–177.
Wasser L, Talavera W. Pulmonary cryptococcosis in AIDS. Chest 1987;92:692–695.
Miller WT Jr, Edeman JM, Miller WT. Cryptococcal pulmonary infection in patients with AIDS: radiographic appearance. Radiology 1990;175:725–728.
Khoury MB, Godwin JD, Ravin CE, Gallis HA, Halvorsen RA, Putman CE, et al. Thoracic cryptococcosis: immunologic competence and radiologic appearance. AJR Am J Roentgenol 1984;141:893–896.
Sayler NR, Sayler DC, Backer RD. Primary complex of Cryptococcus and pulmonary lymph nodes. Journal of Infectious Diseases 1974;130:74–77.
Craig TJ. Adverse reaction to fluconazole: illustrative case with focus on desensitization. J Am Osteopath Assoc 1997;97:584–587.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Yamaguchi, H., Komase, Y., Ikehara, M. et al. Disseminated cryptococcal infection with eosinophilia in a healthy person. J Infect Chemother 14, 319–324 (2008). https://doi.org/10.1007/s10156-008-0618-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10156-008-0618-z