
Abstract
Background
This study sought to identify and compare the current practice of surgeons in Australia, the UK and the US when presented with a left-sided colonic emergency.
Methods
Questionnaires were posted to 500 US, 500 UK and 500 Australian surgeons. Demographic data were collected regarding the surgeon’s age and surgical interest, as well as their preferred method of managing left-sided colonic emergencies (namely obstruction and perforation in stable and unstable patients). The results were analysed using the chi-squared test.
Results
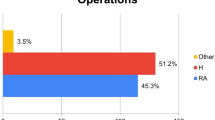
Completed questionnaires were received from 224 UK surgeons (45%), 180 US surgeons (36%) and 259 Australian surgeons (52%). All the US surgeons had an interest in gastrointestinal surgery, while 31% of the UK surgeons and 22% of Australian surgeons had an interest in colorectal surgery. In a haemodynamically stable patient with a good anaesthetic risk presenting with a complete sigmoid obstruction, significantly more UK (84%) and Australian surgeons (70%) would perform a resection and anastomosis than US surgeons (54%, p<0.0001). Of those with a colorectal interest, 97% of UK surgeons and 80% of Australian surgeons would opt for resection and anastomosis. In a haemodynamically stable patient with a good anaesthetic risk with a perforation of the sigmoid colon and purulent peritonitis, 46% of UK surgeons, 32% of Australian surgeons and 33% of US surgeons would opt for resection and anastomosis, and among colorectal surgeons, 68% of UK surgeons and 50% of Australian surgeons would opt for resection and anastomosis.
Conclusions
The management of left-sided colonic emergencies varies depending on geographic location and degree of colorectal subspecialization. While the literature suggests that single-stage procedures are accepted and safe, the reasons for this variation are explored.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Australian Institute of Health and Welfare (2004) Cancer in Australia 2001. Australian Institute of Health and Welfare, Australasian Association of Cancer Registries, Canberra
Ohman U (1982) Prognosis in patients with obstructing colorectal carcinoma. Am J Surg 143:742–747
Mandava N, Kumar S, Pizzi WF et al (1996) Perforated colorectal carcinomas. Am J Surg 172:236–238
Hart AR, Kennedy HJ, Stebbings WS et al (2000) How frequently do large bowel diverticulae perforate? An incidence and cross-sectional study. Eur J Gastroenterol Hepatol 12:661–665
Engledow AH, Bond-Smith G, Motson RW et al (2008) Treatment of left sided colonic emergencies: a comparison of US and UK surgical practices. Colorectal Dis (in press)
Goyal A, Schein M (2001) Current practices in left sided colonic emergencies: a survey of US gastrointestinal surgeons. Dig Surg 18:399–402
Irvin TT, Greaney MG (1977) The treatment of colonic cancer presenting with intestinal obstruction. Br J Surg 64:741–744
Irvin TT, Goligher JC (1973) Aetiology of disruption of intestinal anastomosis. Br J Surg 60:461–464
Carty NT, Ravichandran D (1996) The management of malignant large bowel obstruction. In: Johnson CD, Taylor I (eds) Recent advances in surgery 19. Churchill Livingstone, London, pp 1–18
Fielding LP, Stewart-Brown S, Blesovsky I (1979) Large bowel obstruction caused by cancer: a prospective study. Br Med J 2:515–517
Koruth NM, Krukowski ZH, Youngson GG et al (1985) Intra-operative colonic irrigation in the management of left-sided large bowel emergencies. Br J Surg 72:708–711
Vigler L, Tzur N, Huber M et al (1985) Management of obstructive cancer of the left colon: comparative study of staged and primary resection. Arch Surg 120:825–828
Kronborg O (1986) The missing randomised trial of two surgical treatments for obstruction due to carcinoma of the left colon and rectum: an interim report. Int J Colorect Dis 1:162–166
Waldron RP, Donovan IA (1986) Mortality in patients with obstructing colorectal cancer. Ann R Coll Surg Engl 68:219–221
Huddy SPJ, Shorthouse AJ, Marks CG (1988) The surgical treatment of intestinal obstruction due to left sided carcinoma of the colon. Ann R Coll Surg Engl 70:40–43
Dixon AR, Holmes JT (1990) Hartmann’s procedure for carcinoma of rectum and distal sigmoid colon: 5-year audit. J R Coll Surg Edinb 35:166–168
Stephenson BM, Shandall AA, Farouk R et al (1990) Malignant left sided large bowel obstruction managed by subtotal colectomy. Br J Surg 77:1098–1102
Gandrup P, Lund L, Balslev I (1992) Surgical treatment of acute malignant large bowel obstruction. Eur J Surg 158:427–430
Allen-Mersh TG (1993) Should primary anastomosis and on-table colonic lavage be standard treatment for left colonic emergencies. Ann R Coll Surg Engl 75:195–198
Pearce NW, Scott SD, Karran SJ (1992) Timing and method of reversal of Hartmann’s procedure. Br J Surg 79:839–841
Carty NJ, Corda AP (1992) Which surgeons avoid a stoma in treating left sided colonic obstruction? Results of a postal questionnaire. Ann R Coll Surg Engl 74:391–394
Lee EC, Murray JJ, Coller JA et al (1997) Intraoperative colonic lavage in nonelective surgery for diverticular disease. Dis Colon Rectum 40:669–674
Hsu TC (1998) One-stage resection and anastomosis for acute obstruction of the left colon. Dis Colon Rectum 41:28–32
Koruth NM, Hunter DC, Krukowski ZH et al (1985) Immediate resection in emergency large bowel surgery: a 7 year audit. Br J Surg 72:703–707
Dudley HA, Racliff AG, McGeeham D (1980) Intraoperative irrigation of the colon to permit primary anastomosis. Br J Surg 67:80–81
Kourtesis GJ, Motson RW (1988) Primary anastomosis in emergency distal colonic surgery after on-table colonic lavage. Aust N Z J Surg 58:961–964
Arnaud JP, Casa C, Georgeac C et al (1994) Intraoperative colonic irrigation in the emergency treatment of occlusive lesions of the left colon. J Chir 131:538–540
Biondo S, Perea MT, Rague JM et al (2001) One-stage procedure in non-elective surgery for diverticular disease complications. Colorectal Dis 3:42–45
Maher M, Caldwell MP, Waldron R (1996) Staged resection or primary anastomosis for obstructing lesions of the left colon. Ir Med J 89:138–139
Murray JJ, Schoetz DJ Jr, Coller JA et al (1991) Intraoperative colonic lavage and primary anastomosis in nonelective colon resection. Dis Colon Rectum 34:527–531
Irving AD, Scrimgeour D (1987) Mechanical bowel preparation for colonic resection and anastomosis. Br J Surg 74:580–581
Amsterdam E, Krispin M (1985) Primary resection with colocolostomy for obstructive carcinoma of the left side of the colon. Am J Surg 150:558–560
Dorudi S, Wilson NM, Heddle RM (1990) Primary restorative colectomy in malignant left-sided large bowel obstruction. Ann R Coll Surg Engl 72:393–395
George SM, Fabien TC, Voeller GR et al (1989) Primary repair of colon wounds: a prospective trial in nonselected patients. Ann Surg 209:728–734
Burke P, Mealy K, Gillen P et al (1994) Requirement for bowel preparation in colorectal surgery. Br J Surg 81:907–910
Platell C, Hall J (1998) What is the role of mechanical bowel preparation in patients undergoing colorectal surgery. Dis Colon Rectum 41:875–883
Singhal R, Hull P, Budhoo M (2007) Management of left sided colorectal emergencies. Results of a postal questionnaire. Minerva Chir 62:437–441
The SCOTIA Study Group (1995) Single-stage treatment for malignant left sided colonic obstruction: A prospective randomised control trial comparing subtotal colectomy with segmental resection following intraoperative irrigation. Subtotal colectomy versus irrigation and anastomosis. Br J Surg 82:1622–1627
Regenet N, Pessaux P, Hennekinne S et al (2003) Primary anastomosis after intraoperative colonic lavage vs. Hartmann’s procedure in generalised peritonitis complicating diverticular disease of the colon. Int J Colorectal Dis 18:503–507
De Salvo GL, Gava C, Lise M et al (2004) Curative surgery for obstruction for primary left sided colorectal carcinoma: primary or staged resection? Cochrane Database of Systematic Reviews, Issue 2. Art. no. CD002101
Khot UP, Lang AW, Murali K et al (2002) Systemic review of the efficiency and safety of colorectal stents. Br J Surg 89:1096–1102
Carne PW, Frye JN, Robertson GM et al (2004) Stents or open operation for palliation of colorectal cancer: a retrospective, cohort study of perioperative outcome and long-term survival. Dis Colon Rectum 47:1455–1461
Dastur JK, Forshaw MJ, Modarai B et al (2008) Comparison of short- and long-term outcomes following either insertion of self-expanding metallic stents or emergency surgery in malignant large bowel obstruction. Tech Coloproctol 12:51–55
Alcantara M, Serra X, Bombardó J et al (2007) Colorectal stenting as an effective therapy for preoperative and palliative treatment of large bowel obstruction: 9 years’ experience. Tech Coloproctol 11:316–22
van Hooft JE, Fockens P, Marinelli AW et al (2006) Premature closure of the Dutch Stent-in I study. Lancet 368:1573–1574
van Hooft JE, Bemelman WA, Breumelhof R et al (2007) Colonic stenting as bridge to surgery versus emergency surgery for management of acute left-sided malignant colonic obstruction: a multicenter randomized trial (Stent-in 2 study). BMC Surg 7:12
Hinchey EJ, Schaal PG, Richards GK (1978) Treatment of perforated diverticular disease of the colon. Adv Surg 12:85–109
Alanis A, Papanicolaou GK, Tadros RR et al (1989) Primary resection and anastomosis for treatment of acute diverticulitis. Dis Colon Rectum 32:933–939
Leong QM, Koh DC, Ho CK (2008) Emergency Hartmann’s procedure: morbidity, mortality and reversal rates among Asians. Tech Coloproctol 12:21–25
Myers E, Hurley M, O’sullivan GC et al (2008) Laparoscopic peritoneal lavage for generalized peritonitis due to perforated diverticulitis. Br J Surg 95:97–101
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kozman, D.R., Engledow, A.H., Keck, J.O. et al. Treatment of left-sided colonic emergencies: a comparison of US, UK and Australian surgeons. Tech Coloproctol 13, 127–133 (2009). https://doi.org/10.1007/s10151-009-0469-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-009-0469-3