
Abstract
Background
We aimed to identify patients with a chief complaint of hematuria who could safely avoid unnecessary radiation and instrumentation in the diagnosis of bladder cancer (BC), using automated urine flow cytometry to detect isomorphic red blood cells (RBCs) in urine.
Methods
We acquired urine samples from 134 patients over the age of 35 years with a chief complaint of hematuria and a positive urine occult blood test or microhematuria. The data were analyzed using the UF-1000i ® (Sysmex Co., Ltd., Kobe, Japan) automated urine flow cytometer to determine RBC morphology, which was classified as isomorphic or dysmorphic. The patients were divided into two groups (BC versus non-BC) for statistical analysis. Multivariate logistic regression analysis was used to determine the predictive value of flow cytometry versus urine cytology, the bladder tumor antigen test, occult blood in urine test, and microhematuria test.
Results
BC was confirmed in 26 of 134 patients (19.4 %). The area under the curve for RBC count using the automated urine flow cytometer was 0.94, representing the highest reference value obtained in this study. Isomorphic RBCs were detected in all patients in the BC group. On multivariate logistic regression analysis, only isomorphic RBC morphology was significantly predictive for BC (p < 0.001). Analytical parameters such as sensitivity, specificity, positive predictive value, and negative predictive value of isomorphic RBCs in urine were 100.0, 91.7, 74.3, and 100.0 %, respectively.
Conclusion
Detection of urinary isomorphic RBCs using automated urine flow cytometry is a reliable method in the diagnosis of BC with hematuria.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of hematuria has been reported to be as high as 9–18 % in large screening studies [1, 2]. In patients with hematuria, bladder cancer (BC) is one of the most important diseases that need early and correct diagnosis. Although the need to evaluate all patients with macrohematuria for the presence of BC is widely recognized [3, 4], evaluating patients with microhematuria is controversial [5]. Despite American Urological Association (AUA) best practice policy recommendations including urine testing, imaging, and cystoscopy [6, 7], Jung et al. [8] recently reported that in a large population of patients who underwent microscopic urinalysis, the prevalence of urinary tract cancer was much lower (0.43 %). In addition, the prevalence of urothelial cancer in the general population is low (0.01–3 %) [1, 9–11], translating to a low prior probability of disease for screening. Nevertheless, the AUA practice recommendations did not perform well in identifying which patients were most likely to have malignant tumors, suggesting that there may be alternative criteria that better identify patients who truly require further evaluation [12]. Thus, these limitations of the standard methods for detection of BC have provoked the search for a new easy, reliable, and objective method of diagnosing BC in urine samples [13].
Red blood cell (RBC) morphology in urine is an important piece of diagnostic information when it comes to determining the etiology of hematuria [14–22]. Hematuria can be classified as two types: glomerular (dysmorphic RBCs) and non-glomerular (isomorphic RBCs) [15, 16]. However, a widespread controversy persists regarding the diagnostic value of urinary isomorphic RBCs, primarily because the criteria and methods for examining isomorphism in urinary RBCs remain vague and unstandardized and it is difficult to overcome the intra- and interobserver variation [14, 23, 24].
The new automated urine flow cytometer is an instrument that analyzes urine samples in batches by combining flow cytometry with fluorochrome and impedance analysis [17]. On the basis of these findings, we undertook a discovery prospective cohort study, to determine the diagnostic value of this new fully-automated urine flow cytometer for the specific detection of BC.
Patients and methods
Patients
Between June and December 2011, we conducted a discovery cohort analysis of urine samples from 134 patients with a chief complaint of hematuria. All patients with or without a referral visited our urological department because of a positive urine occult blood test or microhematuria. According to AUA guidelines [25], we included patients over the age of 35 years. Their evaluations were performed according to a standard protocol that essentially mirrored the AUA best practice recommendations for hematuria [4, 6]. Staging and grading were performed in accordance with the 2009 TNM staging and the 2004 World Health Organization grading systems [26]. Informed consent was obtained from each participant. This study was conducted in accordance with an assurance filed with the Ministry of Health, Labor and Welfare and in compliance with the moral, ethical, and scientific principles governing clinical research as set out in the Declaration of Helsinki 1989.
Microscopic analysis
We routinely collected urine by the clean-catch method. Immediately after collection, aliquots from these samples were analyzed using the following examinations. Prior to the microscopic analysis of urinary sediment, all urine specimens were routinely examined by automated semiquantitative urinalysis using the US-3100R Plus® (Eiken Chemical Co., Ltd., Tokyo, Japan) to detect positive occult blood (OB) in the urine. OB was scored as 1+, 2+ or 3+ corresponding to values of 3–20, 20–100 and >100 RBCs/μL, respectively. A score of 3+ was considered positive for OB. The urine samples (6–12 ml, depending on concentration of RBCs) were then centrifuged at 1,600 rpm for 5 min. The supernatant was discarded, and a drop of sediment suspension was used for microscopic examination. RBCs were counted manually in accordance with urine sample examination standards [27]. A count of 5 or more RBCs/high power field (HPF) (1 field, 400× magnifications) was considered positive for microhematuria [27]. Urine cytology was categorized into 5 classes. Urine cytology findings ≥4 suggested BC. The technicians who performed these procedures were blind to all clinical information.
Automated urine analysis
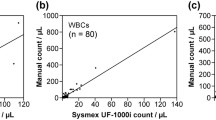
The samples were tested using the UF-1000i ® (Sysmex Co., Ltd., Kobe, Japan), a new flow cytometer that combines diode laser technology with hydrodynamic focusing conductometry [18–20, 28, 29]. The UF-1000i is a fully automated flow cytometer that is capable of classifying and counting cells and formed particles (bacteria, white blood cells, RBCs, yeast-like cells, epithelial cells, crystals, casts, spermatozoa, small round cells, and mucus) in fresh, uncentrifuged urine specimens [19]. The urine sample is automatically mixed, aspirated (0.8 ml in manual mode, 1.2 ml in automated mode), and stained in 2 dedicated analytical channels with new specific fluorescent polymethine dyes: one for bacteria, and a second for leukocytes, yeast-like cells, and urine particles [20]. Each sample is then delivered to a flow cell using hydrodynamic focusing to ensure that each particle passes under the laser beam individually and is aligned lengthwise. For each particle, the scattered light is detected by a photo diode at two different positions (forward- and side-scattered light) and converted into electronic signals, together with fluorescence intensity. The forward scatter provides information on the size, and the side scatter provides information on the surface and internal complexity, while the fluorescence intensity provides information on the nucleic acid content of each particle [20].
The RBCs in urine were classified into two types: glomerular (dysmorphic RBCs) and non-glomerular (isomorphic RBCs), based on data acquired from UF-1000i analysis. As a prerequisite for determining erythrocyte morphology in urine, there must be at least 20 non-hemolytic RBCs per μL in the sample. The flagging of RBC information is determined by the forward scatter (Fsc) histogram. The morphology of RBCs using the Sysmex UF-1000i is determined by 2 other pieces of information: specifically, the comprehensive size of RBCs (RBC-P70Fsc) and the variety of forward scatter of those RBCs [RBC-Fsc-Distribution Width (DW)] are used as standards for judgment. Since the diagnostic criteria for isomorphic RBCs are ≥100 channels (ch) of RBC-P70Fsc and ≤50 ch of RBC-Fsc-DW, the necessity of manually counting the individual isomorphic RBCs is precluded with the UF-1000i.
Statistical analysis
Patients were allocated to two groups based on the presence or absence of BC. The clinical parameters, including sex, age, smoking history (Brinkman index), and results of urine analysis including OB, microhematuria, urine cytology, bladder tumor antigen (BTA) test, and the morphology of RBCs in urine were compared between groups. The final diagnosis of BC was based on clinical (cystoscopy, biopsy, and radiological imaging methods) and/or pathological data. Independent urologists, who were unaware of the laboratory analysis findings, made the clinical diagnosis.
Chi squared analysis (sex, smoking history, urine cytology, BTA test, OB, microhematuria) and t test (age) were used to compare outcomes between the BC group and non-BC group. Multivariate logistic regression analysis was used to identify predictors of BC. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were also evaluated. Receiver operating characteristics (ROC) curve analysis was performed to predict BC. Statistical analysis was done using R (version 2.14.0). A p value <0.05 indicated statistical significance.
Results
Patient characteristics
Table 1 summarizes the clinical parameters for all 134 patients in this study. The median age was 74 years (range 35–91 years). BC was clinically and/or pathologically confirmed in 26 of 134 patients, for a positive rate of 19.4 %. The causes of hematuria in 108 patients without BC are as follows: benign prostate hyperplasia (BPH)/lower urinary tract symptom (LUTS) 28 cases (20.9 %), urolithiasis 22 cases (16.4 %), urinary tract infection (UTI) 17 cases (15.7 %), patients on oral anticoagulants 15 cases (11.2 %), renal cysts 4 cases (3.7 %), glomerulonephritis 2 cases (1.9 %), prostate cancer 1 case (0.7 %), wandering kidney 1 case (0.7 %), and unknown 18 cases (16.7 %). We identified no patients with upper urinary tract cancer. There were slight differences in age between the BC group and non-BC group (Table 2). The results of malignancy potential and clinical staging were as follows: low grade 6 (23.1 %), high grade 19 (73.1 %), unknown 1 (3.8 %); cTa 7 (26.9 %), cT1 5 (19.2 %), cT2 2 (7.7 %), cT3 1 (3.8 %), cT4 6 (23.1 %), and cTis 5 (19.2 %).
Comparative findings between BC group and non-BC group (Table 2)
We compared several clinicopathological parameters in urine between the BC group and non-BC group (Table 2). All OB-positive patients had microhematuria. Microhematuria was detected in 74 participants (96.2 % of BC group, 45.4 % of non-BC group). Although OB demonstrated significant differences between BC group and non-BC group, only 65.4 % patients in BC group and 6.5 % patients in non-BC group were OB-positive. Although almost all patients except one in the BC group demonstrated microhematuria, in the non-BC group 45.4 % showed microhematuria. The BTA test showed positive results in only 5 patients (19.2 %) in the BC group and 34 patients (31.5 %) in the non-BC group, and did not demonstrate any significant differences between the BC group and non-BC group. Although there were significant differences in urine cytology between the BC group and non-BC group, only 4 of 26 BC patients were rated class V for positive urinary cytology. On the other hand, surprisingly, isomorphic RBCs were detected in all patients in the BC group (Table 2). In contrast, the findings were more heterogeneous among the 108 patients in the non-BC group. A few patients had isomorphic RBCs (9 patients, 8.3 %), mixed RBCs (12 patients, 11.1 %), and dysmorphic RBCs (2 patients, 1.9 %). The primary diseases of these patients with isomorphic RBCs in the non-BC group were urolithiasis (3 cases), BPH (2 cases), currently taking oral anticoagulants (1 case), wandering kidney (1 case), and unknown (2 cases).
Multivariate analysis to examine the significant factors in diagnosis of BC
The reference values for BC were based on ROC curve analysis of the automated urine flow cytometry RBC counts, BTA, urine cytology, OB, and microhematuria (Fig. 1). As shown in Fig. 1, the area under the curve (AUC) for the automated urine flow cytometry RBC counts was 0.94, which was higher than those for BTA (0.44), urine cytology (0.74), OB (0.89), and microhematuria (0.75). In addition, on multivariate logistic regression analysis, OB (p = 0.078), microhematuria (p = 0.291), and urine cytology (p = 0.012) were not significant predictors of BC, whereas isomorphic RBCs (p < 0.001) was a single significant predictor for BC (Table 3). Diagnostic performance in terms of sensitivity (100.0 %), specificity (91.7 %), PPV (74.3 %), NPV (100.0 %), and diagnostic accuracy (93.3 %) of isomorphic RBCs in urine for detecting BC were satisfactory (Fig. 2); namely, isomorphic RBCs in urine are associated with greater sensitivity, NPV, and accuracy, and almost equal specificity and PPV as compared with urine cytology and OB.

ROC curves of predicted probabilities of BTA, urine cytology, OB, microhematuria, and the automated urine flow cytometeric RBC counts to identify BC. A score of +++ is considered positive for OB

The sensitivity, specificity, PPV, and NPV of isomorphic RBC, urine cytology, and OB to detect BC were as follows: isomorphic RBC: 100.0, 91.7, 74.3, 100.0 %, urine cytology by classifying the class III samples as negative: 19.2, 99.1, 83.3, 83.6 % (urine cytology by classifying the class III samples as positive: 69.2, 76.0, 40.9, 91.1), OB: 65.4, 93.5, 70.8, 91.8 %, respectively
Discussion
Hematuria is a frequent manifestation of the diseases of the urinary tract [30]. The AUA Guidelines recommend cystoscopy for all patients aged 35 years and older presenting with hematuria and all asymptomatic microhematuria patients who present with risk factors for urinary tract malignancy regardless of age [25]. Cystoscopy, however, is a highly invasive procedure with significant associated risks, including urinary bleeding and febrile UTI [31]. Approximately 10 % of patients with macrohematuria and 2–5 % of patients with microhematuria are ultimately determined to have BC [3, 32]. Loo et al. [12] reported that asymptomatic microscopic hematuria is an unreliable predictor of urothelial malignancy, and suggests that routine testing for malignancy in patients with asymptomatic microscopic hematuria may be unnecessary and may expose patients to unnecessary risks. In fact, most patients and physicians prefer to avoid cystoscopy as a diagnostic tool. Therefore, noninvasive, established, high-integrity and conventional screening tests for BC have been eagerly anticipated.
In this study, all of the OB positive patients had microhematuria. In clinical practice, however, many patients with OB-positive results do not have hematuria. Furthermore, it is well recognized that the effectiveness of OB screening for BC is limited to a small number of patients [33]. Consistent with previous reports, multivariate logistic regression analysis demonstrated that OB was not a significant predictor for BC in this study (Table 3). Although microscopic examination of the urinary sediment currently occupies a critical role in screening for BC, the AUA practice policy reported that only a small percentage (2.6 %) of 3,762 asymptomatic microhematuria patients were found to have a urinary tract malignancy [6]. Despite all patients in this study having high risk factors for BC, the false-positive rate of microhematuria was high at 45.4 % compared with only 8.3 % isomorphic RBCs. As with previous reports [6, 34, 35], the BTA test showed positive results in only 5 patients (19.2 %) belonging to BC group, and the findings were similar between the BC group and non-BC group (Table 2) in the present study. Although urine cytology is also commonly used to screen for BC in cases with a definitive diagnosis of hematuria, this test is associated with a high rate of false-negative results [6, 35], and 27 studies have reported a wide range of sensitivity values, ranging from 0 to 100 %, and specificity values, ranging from 62.5 to 100 % [6]. Urine cytology allows detection of BC with a high grade of malignancy, but the technique is much less reliable in tumor cells with low grade malignancy. In addition, the accuracy of cytological diagnosis depends, to a large extent, on the experience of the cytologist and can inevitably vary from one cytologist to another. In this study, urine cytology had a sensitivity of only 19.2 % (Fig. 2), and was not a significant predictor for BC in multivariate logistic regression analysis (Table 3). On the other hand, the sensitivity of isomorphic RBCs in urine was 100.0 %, considerably higher than that of urine cytology (19.2 %, Fig. 2), and isomorphic RBCs were significant predictors for BC (p < 0.001, Table 3).
Since the publication by Fairley and Birch [36], it is well known that two main types of RBCs can be found in the urine: isomorphic RBC (a marker of nonglomerular bleeding) and dysmorphic RBC (a marker of glomerular diseases). Discriminating with the naked eye between glomerular and nonglomerular causes of hematuria can be difficult in clinical practice. Shichiri et al. [16] reported the distribution curves of urinary RBC size using automated blood cell analysis. Varieties of automated systems, including computer-assisted light microscopy [37], immunocytochemical staining, flow cytometric analysis of erythrocytes [21], and measurement of the size or mean corpuscular volume of erythrocytes [22], have been used to analyze RBC morphology in urine. However, the accuracy, reproducibility, and reliability of these methods have been repeatedly challenged [14, 21, 33].
The UF-1000i automated urine analyzer uses a semiconductor laser with forward- and side-scatter detection and a single DNA dye for its 2 counting channels: 1 for sediment analysis and 1 for microbes [18]. Some authors have reported the effectiveness of automated urine flow cytometry screening for other disorders [20]. On the basis of these findings, we evaluated the efficacy of automated urine flow cytometry for BC screening. Without exception, the automated urine flow cytometer detected isomorphic RBCs in the BC group (Table 2). This finding was extremely favorable in comparison with other test results (Fig. 2). On multivariate logistic regression analysis, isomorphic RBCs (p < 0.001) was the only significant predictor for BC (Table 3). In this study, we can detect isomorphic RBCs in patients not only with high grade/stage BC but also with low grade/stage BC. This is the first report to indicate the effectiveness of using isomorphic RBCs in urine by automated urine flow cytometry for BC screening in cases with hematuria. The UF-1000i determines RBC morphology based on the comprehensive size of RBCs (RBC-P70Fsc) and the degree of forward scatter observed (RBC-Fsc-DW). A previous report found that this method may be more reliable and accurate than inspection of urine RBCs by phase contrast microscopy [22]. Consequently, we can expect this fully-automated system to show high reproducibility, unlike urine cytology. The automated urine flow cytometer rapidly identified positive samples. Theoretically, it can analyze up to 100 samples per hour, requiring a volume of 4.0 ml of fresh, uncentrifuged urine samples in automated mode. Given the large number of urine samples that must be evaluated in a short time for mass screening, we believe that the automated urine flow cytometer is a useful addition to existing BC screening tools in patients with hematuria.
All patients included in this study visited our urological department due to hematuria, such as positive urine OB or microhematuria. Since our institution is a hub cancer center in North Tokyo, almost all patients were referred to our department on suspicion of urothelial cancer. Therefore, this selection bias was the major limitation of this study and produced the high detection rate of BC (19.4 %). The second limitation of this study was the small number of study subjects (n = 134). Several other potentially confounding factors warrant mention. First, we detected isomorphic RBCs in 9 patients (8.3 %) who did not have BC. The primary diseases of these patients with isomorphic RBC in the non-BC group were urolithiasis, BPH, currently-taking oral anticoagulants, and wandering kidney. In comparison with glomerular disease, the efficacy of urinary RBC morphology in diagnosis of non-glomerular diseases is scarcely known [18–20]. Consequently, we could not clarify the cause of our false-positive results. Second, Kitamoto et al. [38] showed the effect of different pH or osmolality on the shapes of urinary RBCs in glomerulonephritic patients. Although it is well-known that RBCs transform into a confetti-like shape under higher osmolality with low pH in the urine, we could not evaluate such influence on the diagnosis because of a lack of sufficient data. Third, for the purposes of this study, we defined microscopic hematuria as 5 or more RBCs per HPF on microscopic examination, in accordance with the Japanese guidelines [27]. Some global guidelines define microhematuria as 2 or more RBCs per HPF [3, 6, 39], while others range from 1 to more than 10 RBCs per HPF [6, 9]. Since the Japanese guideline represents the average of this range, we feel confident in using this value.
We concluded that isomorphic RBCs using automated urine flow cytometry is a much more reliable and non-invasive method in the diagnosis of BC in patients with hematuria compared with conventional examinations including urine cytology.
References
Mohr DN, Offord KP, Owen RA et al (1986) Asymptomatic microhematuria and urologic disease: a population-based study. JAMA 256:224–229
Freni SC, Freni-Titulaer LW (1977) Microhematuria found by mass screening of apparently healthy males. Acta Cytol 21:421–423
Cohen RA, Brown RS (2003) Clinical practice. Microscopic hematuria. N Engl J Med 348:2330–2338
Grossfeld GD, Litwin MS, Wolf JS Jr et al (2001) Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy—part II: patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology 57:604–610
Lotan Y, Capitanio U, Shariat SF et al (2009) Impact of clinical factors, including a point-of-care nuclear matrix protein-22 assay and cytology, on bladder cancer detection. BJU Int 103:1368–1374
Grossfeld GD, Litwin MS, Wolf JS et al (2001) Evaluation of asymptomatic microscopic hematuria in adults: the American Urological Association best practice policy—part I: definition, detection, prevalence, and etiology. Urology 57:599–603
Grossfeld GD, Wolf JS, Litwin MS et al (2001) Asymptomatic microscopic hematuria in adults: summary of the AUA best practice policy recommendations. Am Fam Physician 63:1145–1154
Jung H, Gleason JM, Loo RK et al (2011) Association of hematuria on microscopic urinalysis and risk of urinary tract cancer. J Urol 185:1698–1703
Sutton JM (1990) Evaluation of hematuria in adults. JAMA 263:2475–2480
Thompson IM (1987) The evaluation of microscopic hematuria: a population-based study. J Urol 138:1189–1190
Murakami S, Igarashi T, Hara S et al (1990) Strategies for asymptomatic microscopic hematuria: a prospective study of 1,034 patients. J Urol 144:99–101
Loo RK, Lieberman SF, Slezak JM et al (2013) Stratifying risk of urinary tract malignant tumors in patients with asymptomatic microscopic hematuria. Mayo Clin Proc 88:129–138
Cunderlíková B, Wahlqvist R, Berner A et al (2007) Detection of urinary bladder cancer with flow cytometry and hexaminolevulinate in urine samples. Cytopathology 18:87–95
Venkat Raman G, Pead L, Lee HA et al (1986) A blind controlled trial of phase-contrast microscopy by two observers for evaluating the source of haematuria. Nephron 44:304–308
Crop MJ, de Rijke YB, Verhagen PC et al (2010) Diagnostic value of urinary dysmorphic erythrocytes in clinical practice. Nephron Clin Pract 115:c203–c212
Shichiri M, Hosoda K, Nishio Y et al (1988) Red-cell-volume distribution curves in diagnosis of glomerular and non-glomerular haematuria. Lancet 331:908–911
Pieretti B, Brunati P, Pini B et al (2010) Diagnosis of bacteriuria and leukocyturia by automated flow cytometry compared with urine culture. J Clin Microbiol 48:3990–3996
Wang J, Zhang Y, Xu D et al (2010) Evaluation of the Sysmex UF-1000i for the diagnosis of urinary tract infection. Am J Clin Pathol 133:577–582
De Rosa R, Grosso S, Bruschetta G et al (2010) Evaluation of the Sysmex UF1000i flow cytometer for ruling out bacterial urinary tract infection. Clin Chim Acta 411:1137–1142
Manoni F, Fornasiero L, Ercolin M et al (2009) Cutoff values for bacteria and leukocytes for urine flow cytometer Sysmex UF-1000i in urinary tract infections. Diagn Microbiol Infect Dis 65:103–107
Kore RN, Dow CS, Desai KM (1999) A new automated system for urine analysis: a simple, cost-effective and reliable method for distinguishing between glomerular and nonglomerular sources of haematuria. BJU Int 84:454–460
Angulo JC, Lopez-Rubio M, Guil M et al (1999) The value of comparative volumetric analysis of urinary and blood erythrocytes to localize the source of hematuria. J Urol 162:119–126
Ohsaki H, Hirakawa E, Kushida Y et al (2010) Can cytological features differentiate reactive renal tubular cells from low-grade urothelial carcinoma cells? Cytopathology 21:326–333
Kesson AM, Talbott JM, Gyory AZ (1978) Microscopic examination of urine. Lancet 2:809–812
Davis R, Jones JS, Barocas DA et al (2012) American Urological Association. Diagnosis, evaluation and follow-up of asymptomatic microhematuria (AMH) in adults: AUA guideline. J Urol 188:2473–2481
Sauter G, Algaba F, Amin M et al (2004) Tumours of the urinary system: non-invasive urothelial neoplasias. In: Eble JN, Sauter G, Epstein Jl, Sesterhenn I (eds) WHO classification of classification of tumors of the urinary system and male genital organs. IARCC Press, Lyon, pp 29–34
Higashihara E, Nishiyama T, Horie S et al (2008) Working group for the creation of hematuria guideline: hematuria. Definition and screening test methods. Int J Urol 15:281–284
Manoni F, Tinello A, Fornasiero L et al (2010) Urine particle evaluation: a comparison between the UF-1000i and quantitative microscopy. Clin Chem Lab Med 48:1107–1111
Nanos NE, Delanghe JR (2008) Evaluation of Sysmex UF-1000i for use in cerebrospinal fluid analysis. Clin Chim Acta 392:30–33
Tesser Poloni JA, Bosan IB, Garigali G et al (2012) Urinary red blood cells: not only glomerular or nonglomerular. Nephron Clin Pract 120:c36–c41
Vasanthakumar V (1990) A study to assess the efficacy of chemoprophylaxis in the prevention of endoscopy-related bacteraemia in patients age 60 and over. Q J Med 75:647–653
Messing EM, Young TB, Hunt VB et al (1995) Hematuria home screening: repeat testing results. J Urol 154:57–61
Khan MA, Shaw G, Paris AMI (2002) Is microscopic haematuria a urological emergency? BJU Int 90:355–357
Konety BR, Getzenberg RH (2001) Urine based markers of urological malignancy. J Urol 165:600–611
Rife CC, Farrow GM, Utz DC (1979) Urine cytology of transitional cell neoplasms. Urol Clin North Am 6:599–612
Fairley KF, Birch DF (1982) Hematuria: a simple method for identifying glomerular bleeding. Kidney Int 21:105–108
van den Broek D, Keularts IM, Wielders JP et al (2008) Benefits of the iQ200 automated urine microscopy analyser in routine urinalysis. Clin Chem Lab Med 46:1635–1640
Kitamoto Y, Yide C, Tomita M et al (1992) The mechanism of glomerular dysmorphic red cell formation in the kidney. Tohoku J Exp Med 167:93–105
Elias K, Svatek RS, Gupta S et al (2010) High risk patients with hematuria are not evaluated according to guideline recommendations. Cancer 116:2954–2959
Acknowledgments
This study was supported in part by a Grant-in-Aid for Progressive Renal Diseases Research, from the Ministry of Health, Labour and Welfare of Japan.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Muto, S., Sugiura, Si., Nakajima, A. et al. Isomorphic red blood cells using automated urine flow cytometry is a reliable method in diagnosis of bladder cancer. Int J Clin Oncol 19, 928–934 (2014). https://doi.org/10.1007/s10147-013-0623-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-013-0623-9