
Abstract
Background
Posttraumatic stress symptom (PTSS) and posttraumatic growth (PTG) were surveyed in parents of childhood, adolescent and young adult patients with high-grade osteosarcoma.
Methods
A questionnaire survey was performed in parents of patients with osteosarcoma (51 families). The Impact of Event Scale-Revised (IES-R) and posttraumatic growth inventory (PTGI) were employed for the evaluation of PTSS and PTG, respectively. The mean scores were compared with those in preceding studies employing the same scales. In addition, the correlation between the IES-R and PTGI scores was investigated in the parents.
Results
Fifty-eight subjects of 34 families (30 fathers and 28 mothers) replied to the questionnaire. The mean IES-R score in the parents was 18.5, which was higher than that in patients with osteosarcoma (9.7) in our previous study. The mean PTGI score in the parents was 44.9, which was higher than that in university students (33.9) reported by Taku et al. A positive correlation was noted between the IES-R and PTGI scores in the parents.
Conclusions
The PTSS level tended to be higher in the parents rather than in patients with osteosarcoma. The PTG level increased as the PTSS level rose in the parents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Humans show 2 contrary reactions after experiencing mental trauma. One is a negative reaction on feeling the mental stress of the trauma, termed a posttraumatic stress symptom (PTSS) [1, 2]. The other is a positive reaction, mental growth, termed posttraumatic growth (PTG) [3]. PTSS has been reported for a long time, but the concept of PTG has only been reported over about the last decade.
We have studied the quality of life (QOL) of long-term survivors with high-grade osteosarcoma [4]. We investigated psychosocial outcomes of long-term survivors with osteosarcoma, and reported that their PTSS level was low and their PTG level was high. We also reported that a favorable family function reduced the PTSS level in long-term survivors with osteosarcoma, and the strengthening of social support elevated their PTG level [5].
In pediatric cancer cases, PTSS and PTG may occur not only in patients but also in their parents. PTSS and PTG in parents of patients with pediatric cancer have recently been increasingly reported [6–10], but there has been no study on PTSS and PTG in which the subjects were limited to parents of childhood, adolescent and young adult patients with high-grade osteosarcoma. We performed a questionnaire survey on PTSS and PTG in parents of patients with osteosarcoma treated at our center to clarify the current state and problems.
To our knowledge, this is the first report in which PTSS and PTG were investigated in parents of patients with osteosarcoma. This study showed that the PTSS level tended to be higher in the parents than in the patients with osteosarcoma. In addition, the PTG level increased as the PTSS level rose in the parents.
Materials and methods
Participants
Fifty-one patients with osteosarcoma met all of the following 4 conditions: (1) patients with high-grade osteosarcoma treated at our center in 1976 and thereafter, (2) younger than 20 years at the time of diagnosis, (3) disease-free for 3 years or longer after the completion of treatment, and (4) being followed up with a known address. A questionnaire survey on PTSS and PTG was performed in the parents of these 51 patients. Prior to this study, the protocol was approved by the Institutional Research Board. Informed consent was obtained from each participant.
Evaluation of PTSS and PTG in parents
The Impact of Event Scale-Revised (IES-R) was employed to evaluate PTSS in the parents, and the posttraumatic growth inventory (PTGI) for PTG. The mean scores were compared with those in previous studies employing the same scales.
IES-R is a self-report questionnaire comprising 22 items. The PTSS level rises as the score increases. IES-R contains 3 subscales (Intrusion, Avoidance, Hyperarousal) [1, 11]. PTGI is also a self-report questionnaire comprising 18 items, and the PTG level rises as the score increases. PTGI contains 4 subscales (Relating to others, New possibilities, Personal strength, Spiritual change and appreciation of life) [3, 12, 13].
Factors correlated with IES-R and PTGI of parents
Correlations of the IES-R and PTGI scores of parents with the parents’ age at the time of survey, parents’ gender, patients’ age at the time of diagnosis, patients’ gender, state of the affected limb of the patients, and time after the end of treatment were investigated.
Correlation between IES-R and PTGI in parents
The correlation between the IES-R and PTGI scores in parents was investigated. IES-R was divided into 3 subscales: IESR-Intrusion, IESR-Avoidance, and IESR-Hyperarousal, and PTGI was divided into 4 subscales: PTGI-Relating to others, PTGI-New possibilities, PTGI-Personal strength, and PTGI-Spiritual change and appreciation of life. The correlation between the individual subscales was investigated.
Statistical analysis
Correlations were investigated employing Pearson’s correlation coefficient. A p value <0.05 was considered to be statistically significant for all tests. The data were analyzed with StatView 5.0 (Abacus Concepts, Inc., Piscataway, NJ, USA).
Results
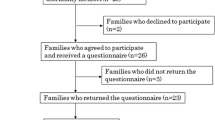
Thirty-four families (66.7%) replied to the questionnaire. The patients’ clinical characteristics of the 51 eligible families and 34 families included in the study are shown in Table 1. Only the father participated in 6 families, only the mother participated in 4 families, and both parents participated in 24 families; 30 fathers and 28 mothers replied to the questionnaire. The age of the parents at the time of survey was 41–79 years (mean 61.6 years), and those of fathers and mothers were 45–79 (mean 63.1 years) and 41–76 years (mean 59.8 years), respectively. The time after the completion of treatment was 43–375 months (mean 210 months).
The mean IES-R score was 18.5 in the parents of patients with osteosarcoma (Table 2), 9.7 in patients with osteosarcoma in our previous study [5], and 18.34 in parents of patients with pediatric cancer reported by Jurbergs et al. [9] (Table 3).
The mean PTGI score was 44.9 in the parents of patients with osteosarcoma (Table 2), 51.8 in patients with osteosarcoma in our previous study [5], and 33.9 in Japanese university students reported by Taku et al. [12] (Table 3).
Neither the IES-R nor the PTGI score was significantly correlated with the parents’ age at the time of survey, parents’ gender, patients’ age at the time of diagnosis, patients’ gender, state of the affected limb of the patients, or time after the end of treatment (Table 4).
A significant positive correlation was observed between the mean IES-R and PTGI scores in the parents (r = 0.478, p = 0.0001). A significant correlation was absent only between ‘Hyperarousal’ of IES-R and ‘Personal strength’ of PTGI. All other subscales of IES-R and PTGI were significantly correlated (Table 5).
Discussion
In pediatric cancer cases, PTSS and PTG may occur not only in patients but also in their parents. PTSS and PTG in parents of patients with pediatric cancer have recently been increasingly reported [6–10], but there has been no study on PTSS and PTG in which the subjects were limited to parents of patients with osteosarcoma.
In the literature concerning PTSS of parents of patients with pediatric cancer, Kazak et al. [6] measured the PTSS level by employing IES-R in parents of survivors with pediatric cancer, and observed that the mean scores in the mothers and fathers were 28.2 and 24.2, respectively. Jurbergs et al. [9] also measured the PTSS level by employing IES-R in parents of patients with pediatric cancer, and observed a mean score in the parents of 18.34.
In our study, the mean IES-R score was 18.5 in the parents of the patients with osteosarcoma, similar to that reported by Jurbergs et al. [9]; that in patients with osteosarcoma was 9.7 in our previous study [5]. The mean IES-R score tended to be higher in the parents rather than in the patients with osteosarcoma, showing that the PTSS level tended to be higher in the parents rather than in the patients. Continuous appropriate counseling may be necessary not only for patients but also for their parents.
Jurbergs et al. [9] reported that the mean IES-R score was high in parents whose children were under treatment or experienced recurrence, showing a high PTSS level in these parents. Our study investigated parents of long-term survivors with osteosarcoma, but did not include parents whose children were under treatment or experienced recurrence. A higher PTSS level is expected in parents of patients under treatment and with experience of recurrence. PTSS in these parents remains to be investigated.
The mean PTGI score was 44.9 in the parents of the patients with osteosarcoma, and this was higher than that in university students in Japan (33.9) reported by Taku et al. [12], showing that they mentally grew through experiencing their child’s disease, but the mean PTGI score in the parents was lower than that in patients with osteosarcoma (51.8) previously reported by us [5], showing that the PTG level of the parents tended to be lower than that of the patients.
In our previous study, no correlation was noted between PTSS and PTG in patients with osteosarcoma [5]. A significant positive correlation was present between the mean IES-R and PTGI scores in the parents in this study, showing that the PTG level increased as the PTSS level rose in the parents. Continuous appropriate counseling of parents of patients may change the negative reactions of the parents to markedly positive reactions. Counseling of patients has been slowly spreading, but continuous, appropriate counseling of parents of patients may be necessary in the future.
Regarding the limitations of this study, since the subjects were parents of patients with osteosarcoma at a single center, it is unclear whether the findings can be generalized. Moreover, the previous studies were adopted for the control, i.e., historical control, but it may be necessary to establish a control within the study. Strict comparison of IES-R and PTGI between the patients [5] and their parents (this study) was impossible because the surveys of the patients and their parents were not performed in the same period, and the cohort was not identical. We are planning to perform a multicenter study and increase the number of participants.
In conclusion, the PTSS level tended to be higher in the parents rather than in the patients with osteosarcoma. The parents mentally grew through experiencing their child’s disease, but the PTG level in the parents was lower than that in the patients. The PTG level increased as the PTSS level rose in the parents.
References
Horowitz M, Wilner N, Alvarez W (1979) Impact of Event Scale: a measure of subjective stress. Psychosom Med 41:209–218
Barakat LP, Kazak AE, Meadows AT et al (1997) Families surviving childhood cancer: a comparison of posttraumatic stress symptoms with families of healthy children. J Pediatr Psychol 22:843–859
Tedeschi RG, Calhoun LG (1996) The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress 9:455–471
Yonemoto T, Ishii T, Takeuchi Y et al (2007) Evaluation of quality of life (QOL) in long-term survivors of high-grade osteosarcoma: a Japanese single center experience. Anticancer Res 27:3621–3624
Yonemoto T, Kamibeppu K, Ishii T et al (2009) Psychosocial outcomes in long-term survivors of high-grade osteosarcoma: a Japanese single-center experience. Anticancer Res 29:4287–4290
Kazak AE, Alderfer M, Rourke MT et al (2004) Posttraumatic stress disorder (PTSD) and posttraumatic stress symptoms (PTSS) in families of adolescent childhood cancer survivors. J Pediatr Psychol 29:211–219
Phipps S, Long A, Hudson M et al (2005) Symptoms of post-traumatic stress in children with cancer and their parents: effects of informant and time from diagnosis. Pediatr Blood Cancer 45:952–959
Barakat LP, Alderfer MA, Kazak AE (2006) Posttraumatic growth in adolescent survivors of cancer and their mothers and fathers. J Pediatr Psychol 31:413–419
Jurbergs N, Long A, Ticona L et al (2009) Symptoms of posttraumatic stress in parents of children with cancer: are they elevated relative to parents of healthy children? J Pediatr Psychol 34:4–13
Michel G, Taylor N, Absolom K et al (2010) Benefit finding in survivors of childhood cancer and their parents: further empirical support for the Benefit Finding Scale for Children. Child Care Health Dev 36:123–129
Asukai N, Kato H, Kawamura N et al (2002) Reliability and validity of the Japanese-language version of the impact of event scale-revised (IES-R-J): four studies of different traumatic events. J Nerv Ment Dis 190:175–182
Taku K, Calhoun LG, Tedeschi RG et al (2007) Examining posttraumatic growth among Japanese university students. Anxiety Stress Coping 20:353–367
Taku K, Cann A, Calhoun LG et al (2008) The factor structure of the posttraumatic growth inventory: a comparison of five models using confirmatory factor analysis. J Trauma Stress 21:158–164
Conflict of interest
No author has any conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Yonemoto, T., Kamibeppu, K., Ishii, T. et al. Posttraumatic stress symptom (PTSS) and posttraumatic growth (PTG) in parents of childhood, adolescent and young adult patients with high-grade osteosarcoma. Int J Clin Oncol 17, 272–275 (2012). https://doi.org/10.1007/s10147-011-0286-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-011-0286-3