
Abstract
Historically, brain tumour resection has relied upon standardised anatomical atlases and classical mapping techniques for successful resection. While these have provided adequate results in the past, the emergence of new technologies has heralded a wave of less invasive, patient-specific techniques for the mapping of brain function. Functional magnetic resonance imaging (fMRI) and, more recently, diffusion tensor imaging (DTI) are two such techniques. While fMRI is able to highlight localisation of function within the cortex, DTI represents the only technique able to elucidate white matter structures in vivo. Used in conjunction, both of these techniques provide important presurgical information for thorough preoperative planning, as well as intraoperatively via integration into frameless stereotactic neuronavigational systems. Together, these techniques show great promise for improved neurosurgical outcomes. While further research is required for more widespread clinical validity and acceptance, results from the literature provide a clear road map for future research and development to cement these techniques into the clinical setup of neurosurgical departments globally.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In recent years, there has been significant interest in using functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI) for localising brain regions that may be at risk during neurosurgical procedures. There is an increasing number of groups worldwide that have integrated both of these modalities with existing stereotaxic guidance systems, resulting in clinical insights for the neurosurgeon particularly in terms of mapping eloquent cortical regions. The successful resection of primary brain tumours can improve survival, functional performance as well as the effectiveness of adjuvant therapies, provided that surgically induced neurological deficits can be avoided [56]. Eloquent regions of cortex must therefore be identified pre- and intraoperatively, so that resection can spare these areas. Traditionally, mapping of eloquent cortex has been achieved by invasive methods such as direct electrical stimulation (DES) in the awake patient, implantation of a subdural grid with extraoperative stimulation mapping or operative sensory-evoked potential recordings [56]. While accurate, these techniques are difficult to perform, place great stress on the patient and often require a larger craniotomy than necessary for the removal of the tumour. For example, DES, long considered as the ‘gold standard’ for functional mapping during tumour resection near eloquent cortex [9], is not without its limitations. Although it can be performed during tumour resection to identify motor pathways in deep WM structures, it prolongs the operating time, is unable to reveal the full three-dimensional extent of an important white matter (WM) tract and can only be undertaken once the specific tract has been encountered surgically [15]. In contrast to the invasiveness of the aforementioned techniques, fMRI and DTI are both less invasive methods for the mapping of brain structure and function. fMRI can be obtained preoperatively, is repeatable and is entirely noninvasive. The integration of functional imaging data (obtained from fMRI) together with WM tractography (obtained from DTI) into a neuronavigation systems provides the neurosurgeon with a coregistered map of spatial localisation of both functional and structural information within eloquent cortex. As a general rule, differentiating tumour from normal brain parenchyma during surgery can be challenging, given the limitations of visual inspection. In addition, many primary brain tumours often grow by infiltration of healthy tissue, meaning that there may be functional WM tracts within the boundaries of certain tumour types [53]. Thus, knowing the position of important WM tracts in relation to intracranial lesions can help prevent significant functional damage subsequent to an overarching resection and help modify the approach to the tumour’s removal, thereby enabling a safer, more patient-specific procedure [49].
MRI and blood oxygen level-dependent fMRI
MRI is an imaging technique that enables the depiction of the inner organs of the body based on the physical properties of unpaired atomic nuclei and typically has a spatial resolution of 1–3 mm. fMRI, on the other hand, is used to estimate and localise neuronal activation in the grey matter of the brain. This method is based on the principle of neurovascular coupling, which implies that an increase in neuronal activity will cause a rise in blood oxygen consumption and a concomitant rise in local cerebral perfusion. This increased blood flow to the activated region alters the ratio between the deoxyhaemoglobin and oxyhaemoglobin. Deoxyhaemoglobin is paramagnetic, allowing it to influence the signal (termed the blood oxygenation level dependent; BOLD) registered in the MRI. The BOLD response reflects the degree of oxygenation of the blood in capillaries supplying brain tissue, and its neurophysiological basis lies in changes to blood flow and level of oxygenation in response to neuronal activity. Although the exact physiological mechanisms relating BOLD and neuronal activity are yet to be fully explicated, it is generally accepted that changes in the BOLD signal indirectly reflect neuronal activity [7].
Several groups have shown good concordance between fMRI and other brain mapping techniques including DES in localisation of motor, somatosensory and visual areas [32, 34]. fMRI has also been used in delineating language areas, with Desmond et al. [13] showing good correlation between fMRI and Wada findings in hemispheric language localisation. Results of precise language localisation have been mixed, with Spena et al. [54] precisely identifying language areas in only 42.8 % of cases in their study of 27 patients harbouring eloquent-area tumours. Roux et al. [50], on the other hand, reported all of the 22 language sites identified by intraoperative cortical mapping to be correlated with fMRI findings in their study of 14 patients with left hemispheric tumours. This variability in findings may be due to (a) multiple and widely distributed nature of language functional epicentres and (b) methodological differences between research groups. Regardless, due to its noninvasiveness, fMRI is repeatable, both for many runs in a single session and on multiple occasions to longitudinally follow patients over an extended time course. It is also suitable for use in children, provided they are able to complete the requisite task with adequate compliance (e.g. with minimal head movement).
Even in the brains of healthy individuals, there exists considerable variability in terms of function and anatomy. Interindividual variability, the effects of brain tumours and their associated mass effects can distort common anatomical landmarks, making reliance upon anatomy-based localisation of function less accurate. Hence, fMRI allows the neurosurgeon to set aside an a priori conception of brain functional organisation and instead favour a more objective, individually tailored and pathology-based approach [54].
fMRI in practice
The functions most commonly mapped during fMRI studies include motor, auditory, somatosensory, visual perception, as well as both language production and comprehension. When testing for motor centres, common tasks include finger tapping, lip pouting and flexion and extension of the toes [56]. Patients with mild to severe motor-hand paresis can perform hand clenching in place of finger tapping. In cases of paralysis, localisation of a patient’s primary motor cortex (M1) may be substantiated indirectly via pure sensory mapping of primary somatosensory cortex (S1). According to Lee et al. [31], this can be achieved by stroking or brushing the associated region of the body. For mapping of primary and secondary auditory cortices, a variety of simple auditory stimuli can be used. Language expression is identified through word generation tasks and may include picture naming, verbal fluency, and verb-to-noun generation, which all involve regions in close relation to and including Broca’s [50]. Language comprehension abilities related to Wernicke’s area can be mapped by semantic judgement tasks. However, in cases where these tasks are too difficult or the patient is suffering from cognitive decline, then listening to spoken language or reading written language can be an alternative, albeit a less optimal one [56]. Recently, a novel language task developed by Berntsen et al. [5], termed the ‘Jeopardy task’, has been shown to reliably map both Broca’s and Wernicke’s areas in the one experimental task, thereby reducing the burden on the patient. Finally, visual stimuli such as flashing lights or flickering checkerboards can be used to arouse activity in the occipital region of the brain. According to Sunaert et al. [57], more detailed mapping of primary and higher-order visual areas, including V1, V2, V3, V3A and V4 and hMT/V5, can be rapidly produced using wedge-shaped alternating checkerboards placed on vertical and horizontal axes in the visual field.
BOLD fMRI limitations and considerations
Considerations regarding the BOLD signal
There is a latency of several seconds in the observed signal change in BOLD imaging, making the temporal resolution of the fMRI poor when compared to other techniques such as DES or electroencephalography [58]. This is due to the ‘haemodynamic response delay’ given the time required for production and diffusion of vascular signal substances to dilate the vascular bed and cause a washout of deoxygenated haemoglobin. Another consideration, raised by Lu et al. [33], is that BOLD fMRI does not measure the neuronal activity directly but rather the changes in the haemodynamic properties of the region. This could imply that intersubject variability in functional localisation may in fact be a result of physiological differences in the BOLD signal rather than differences in neuronal activity per se. To this end, it has been found that the BOLD signal can be influenced by various pharmacological agents. Accordingly, Laurienti et al. [29] has shown that caffeine is able to increase the BOLD response to a task. In contrast, antihistamines reduce it. Critically, in the context of brain tumours, numerous groups have found that the tumour can exert adverse effects on the precision of the BOLD signal. Ulmer et al. [59] found that a tumour’s vascularisation may influence functional maps. Hou et al. [22] found that gliomas reduced signal at their periphery and that the grade of the glioma correlated with the reduction in the observed signal in their study of tumour neovascularisation and its effect on BOLD fMRI in the primary motor cortex. Grade IV gliomas exerted a greater effect relative to their grade II and grade III counterparts. Notably, glioma tumours have even been found to influence the BOLD signal in normal vascular territories somewhat removed from the tumour mass [52]. The pathophysiology behind these findings hinges on the ability of neoplasms to influence the brain’s ability to autoregulate blood flow in areas that are still functioning, implying that an affected area would no longer match increased neural activity to increased local cerebral blood flow—a concept referred to as neurovascular uncoupling. Indeed, the hypothesis that is tested at each voxel of an imaged brain is that there is no effect of the fMRI task compared to the baseline condition, and the statistical analysis involves making a decision as to whether or not this null hypothesis is true or false. Since fMRI measurements are intrinsically noisy, this leads to a relatively high number of false negative voxels—areas with actual neural activation but large physiological and/or technique-dependent noise that do not show up on the activation maps. These findings serve to highlight that an absence of fMRI activity in a particular brain region does not indicate that neuronal activity within this area is nonexistent.
Considerations regarding fMRI
One issue that arises in relation to fMRI results is that of essential vs. expendable regions of the brain. Expendable areas are those that correlate with but which are not essential for the performance of a given neurological task. In terms of methods of observing brain function, the current gold standard, DES, works by reversibly inhibiting neuronal function in certain areas so as to derive the functional consequence of its removal. fMRI, on the other hand, is an observational method which seeks to reveal, via a proxy (i.e. blood flow), increased regions of electrical activity as a result of a task or function. Mapping with fMRI demonstrates involvement of various brain areas in a specific function, without demonstrating neither necessity nor sufficiency [58], an obvious shortcoming.
Functional MRI is based on T2*-weighted MRI imaging. The use of this imaging sequence makes the technique vulnerable to distortions and artefacts of multiple origins. In regions where the magnetic field crosses between tissues (e.g. in proximity to air-filled sinuses) geometric distortion can occur, giving a false indication of the true position of the activated region. Artefacts can also arise due to subject motion or be physiology-related with cardiac pulsation and respiration both known to cause signal distortion artefacts. Krings et al. [28] found that head movement artefacts represented the most frequent cause for unusable fMRI images. Motion artefacts also occurred more frequently with tasks involving proximal rather than distal muscle use. Artefacts or distortions were also found to arise due to magnetic field inhomogeneities arising within the scanner itself. Finally, the process from image acquisition to the production of functional brain activation maps and their eventual interpretation consists of several steps, each of which is complex and vulnerable to sources of error. For this reason it is of great importance for expertise and hands-on training in fMRI acquisition, analysis and functional neuroanatomy to better ensure the correct implementation of fMRI investigations [8, 56]. The fMRI technique, therefore, has a number of shortcomings relating mainly to image quality and consistency, which the neurosurgeon must be mindful of and take into account during clinical decision making.
Diffusion tensor imaging and tractography
Until recently, assessing the structure and extent of white matter tracts within the brain has been limited. The advent of DTI and tractography techniques has overcome this obstacle and is now widely used for the studying of white matter in vivo. Diffusion imaging estimates the local direction of white matter from measurements of water diffusion. Tractography takes this a step further, piecing together this information on a voxel-by-voxel basis to infer long-range connectivity between distant brain regions. Water molecules in some tissues diffuse equally in all directions, a concept known as isotropic diffusion. In nerves and white matter tracts, however, the neural cell membranes and the myelin sheaths covering the axons pose a barrier to diffusion and therefore, diffusion of water molecules occurs preferentially in a direction parallel to the main fibre orientation rather than perpendicular to it. This concept is known as anisotropic diffusion and is the basis of this imaging technique [17]. The diffusion anisotropy enables the comparison of fibre tracts so as to allow the estimation of the main fibre orientation within each voxel of the brain. This allows insights into important white matter bundles such as the corticospinal tract, the corpus callosum, association tracts, and visual, language and limbic pathways [4, 12, 21, 25, 38].
DTI is developed from diffusion weighted imaging (DWI). Whereas standard DWI looks at the total amount of diffusion within a given voxel when viewed with no special attention to direction, DTI looks at both the true magnitude and the 3-D direction of the anisotropy in each voxel. Placing a magnetic gradient perpendicular to the direction of a nerve or tract will mean that the water diffusing in the nerve or tract will tend to stay in the same strength region of the gradient and will show relatively little decay from diffusion, gradually becoming brighter relative to the tissue around it. However, if the gradient is then oriented parallel to the direction of the tract, the anisotropically diffusing water molecules will tend to move up and down the gradient more rapidly compared with isotropically diffusing water molecules and so will experience a more rapid signal decay. As a result, the white matter bundle will tend to go dark relative to other tissues around it [30]. DTI uses gradients in six or more directions, making it possible to create a mathematical model of diffusion in three-dimensional space known as the diffusion tensor [25]. From this diffusion tensor, it is possible to calculate the direction of maximum diffusivity, which has been shown to coincide with the main fibre orientation in the white matter of the brain. At least six directions are needed to accurately describe the tensor, but the more directions the gradients are applied in, the more accurate the estimate becomes as it mitigates the effects of noise on the DT-derived parameters [26]. Typical spatial resolution in DTI is a voxel size of 2 × 2 × 2 mm3 although this is improving rapidly [23].
Fractional anisotropy (FA) is one of the main parameters that can be derived from DTI. It provides quantitative information regarding the degree of directionality of water diffusion and is expressed as a numerical value between 0 and 1 with no unit. The higher the FA value, the greater the directionality of water diffusion [36]. Colour-coded maps can also be produced following on from calculations of FA. The accepted convention regarding these maps is that blue is used to highlight tracts travelling in the superior–inferior plane, red the horizontal plane , while green represents fibres running in the anterior–posterior plane [14]. Fibre tracking is another way of presenting DTI images. This allows the visualisation of neural tracts in three dimensions and is based on specific algorithms that enable the calculation of which voxels in the different sequential slices are connected with each other based on the diffusion tensor.
DTI in practice and methodological considerations
DTI is the main imaging method in place that allows the in vivo study of WM anatomy and structural connectivity; however, it is not without its limitations. Two main tracking approaches are used in DTI: deterministic and probabilistic. In the former, the principal direction of the diffusion tensor is tracked from voxel to voxel starting from a seed voxel or region of interest (ROI) until the FA falls below a preset threshold [2]. In this repeatable form of tracking, the point that is eventually reached is not known prior to running the tracking process. In the probabilistic approach, the tracking process is the result of consecutive directions sampled at random from a Gaussian probability density function whose covariance matrix is defined by the tensor at each voxel [20]. In this approach, the connectivity between two areas of the brain can be tested by looking for the probability of the pathways that connect between these given regions [7].
The MRI sequence utilised in DTI is more sensitive to inhomogeneities of the magnetic field and head movement than that used in fMRI. Due to its reliance on heavy gradient pulses, eddy currents lead to a greater potential for signal distortions and must be corrected through the use of mathematical algorithms in the processing of the images [47]. Limitations also apply in the DTI modality itself. As previously mentioned, in tractography, the common voxel size is a cube of dimensions 2 × 2 × 2 mm3. This voxel may contain tens of thousands of axonal slices. Standard DTI, however, is based on the assumption of one main direction of diffusion per voxel known as a consensus average for each voxel. In cases where axonal crossing, kissing or merging occurs, the limited spatial resolution and the tensor’s voxel direction, being an averaged parameter [26], mean that tractography will, by definition, be inaccurate and may in fact fail [7]. This places increased importance on the selection of a suitable tracking algorithm and goes to highlight another issue with DTI technique—the lack of a consistent standardised paradigm. The processing of DTI remains highly user-dependent as it is left to the technician to choose limit values for variables like FA and maximum allowed angulations of tracts. This limits the ability to compare and reproduce results and create optimal imaging methods between centres.
Similar to limitations in fMRI, the tracking of fibres in the vicinity of or within lesions is complicated by changes in diseased tissue, such as tumour-associated oedema as well as tissue compression and degeneration. These changes deform the architecture of the white matter and, in some cases, prevent selection of the seed ROI from which fibre tracking begins. DTI, according to Spena et al. [54], underestimates the presence of functional tracts in the context of the tumour. Also worth considering is that, although DTI provides a representation of WM, it offers little specific information on the functional status or substrates of these tracts and hence the information it provides cannot be solely relied upon to perform surgery; a convergence of information has instead been recommended [54].
fMRI and DTI in presurgical planning
The use of fMRI in conjunction with DTI for presurgical planning is currently the most established clinical application of these neuroimaging techniques (see Fig. 1 for overview of typical procedural steps). The aim is to provide the surgeon with functional information about the area that surrounds the tumour, as well as its connections to adjacent areas. Traditionally, the placing of tracking ROIs has been undertaken using anatomical atlases. More recently, however, the use of fMRI landmarks for ROI selection has been shown to enhance the fibre-tracking performance compared to strictly anatomically based ROI selection and is usually considered reliable in the healthy but may be inaccurate in those harbouring brain lesions [51]. Similarly, Kleiser et al. [27] found that DTI results were more accurate than those using anatomical landmarks alone, in their study using fMRI to localise start points for DTI tract reconstruction. Presurgical planning is also assisted by the ability of DTI to image the local effects of neoplasms on the integrity and trajectory of white matter tracts. Four patterns of anisotropy have been observed in relation to WM tracts in tumour vicinity: (a) normal signal with altered position or direction, seen in cases of tract displacement; (b) decreased but present signal with normal direction and location, supposedly corresponding with vasogenic oedema; (c) decreased signal with disrupted maps, believed to correspond with tumour infiltration; and (d) loss of anisotropic signal corresponding to fibre tract destruction [25]. Information on WM tracts may prove invaluable in preoperative planning by assisting in the avoidance of intact tracts affected by tumour and/or oedema while also providing the surgeon greater confidence when working in areas of the brain where critical WM tracts ought to be but where DTI reveals pre-existing tract destruction.

A flow chart of the steps involved in producing fMRI and DTI maps for neurosurgical planning
Many groups have studied the impact of presurgical planning on patient care noting differences in treatment prior to surgery itself, as well as in the approach to corticotomy, extent of resection and postsurgical outcome. In a study [6] of presurgical DTI and fMRI for assessment of surgical strategy in both glioma and non-glioma patients, surgeries were not undertaken in two (of 51) cases because their imaging results showed that the tumour had embedded itself deep within the motor strip (in one case) or was in close proximity to the frontal language area (the other). In these cases, any attempts to surgically remove the tumour would have resulted in even further functional deficit. Overall, Bertnsen et al. found that the preoperative assessment of eloquent areas had a direct impact on clinical decision making in 8 % of cases, while only one of 33 glioma patients (3 %) experienced a deterioration of neurological status that was specifically caused by surgical manipulation of eloquent areas. In two trials looking at a modification of the surgical approach to corticotomy, the presurgical use of DTI/fMRI led to a change in the surgical approach to resection in 16–21 % of cases [48, 49]. Similarly, Rasmussen et al. also found this presurgical approach to be effective in all five of the cases examined [46]. However, the utility of the technique has been contested by others who found presurgical planning to influence their surgical approach in only 5 % (i.e. 1/19) of their patients [9]. Functional outcome postsurgery represents another set of parameters to be analysed following the use of these techniques. Cao et al. [10] found that, in a restrospective analysis of nine patients with brainstem lesions, presurgical planning using DTI enabled the neurosurgeon to undertake a patient-specific surgical approach and helped achieve an improved modified Rankin scale at follow-up of 0.56–1.66 points over the preoperative average of 2.22 points. The extent of tumour resection can also be analysed subsequent to preoperative fMRI/DTI. Yu et al. [61] reported that, from a patient group of 16, the extent of tumour resection, when assessed postoperatively, was greater than the control group. Notably, Spena et al. [54] found that fMRI/DTI underestimated the presence of functional tracts in the context of the tumour, either surrounding or inside a mass, in all (15) of their patients.
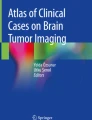
In addition to the more conventional uses of fMRI and/or DTI preoperatively, a number of groups have begun looking at novel uses in relation to tumour surgery. For example, DTI has been used for assessing the probability of an extensive tumour resection. It is has been found that as the distance between tumour and eloquent cortex (otherwise known as the ‘lesion to eloquent area distance’ or ‘LEAD’) decreases, so too does the likelihood of a complete surgical resection. In this way, DTI was seen as a tool that might identify which patients would benefit most from surgery by obtaining a total resection and, thus, having longer term survival [11]. Other preoperative uses have focused on diagnosis of tumour itself with Misaki et al. [36], highlighting the ability of DTI to diagnose astrocytic tumour preoperatively, while in a retrospective review of 40 patients, Jakab et al. [24] found that preoperative DTI could reliably distinguish tumour grading with 92.5 % sensitivity and 88.5 % specificity for low-grade and high-grade gliomas. What is more, preoperative estimation of damage was shown to be possible using fMRI/DTI data [16]. Overall, by providing information essential to preoperative planning, fMRI/DTI helps surgeons form a mental map before opening the dura, thus improving the accuracy of preoperative risk assessments (Fig. 2). These techniques have found widespread use for presurgical planning and represent practical options because of their noninvasiveness and their ease of acquisition [7].

Graphical output of fMRI and DTI analysis. a fMRI results in response to sensorimotor activation and the proximity of the tumour (depicted in green) with respect to the activated cortex. b Proximity and relationship between a intraventricular neurocytoma and the fibres of the corpus callosum
fMRI and DTI in functional neuronavigation
Neuronavigation, is nowadays widely applied in brain surgery and has become a standard procedure in most neurosurgical centres [56]. Integration of fMRI/DTI into neuronavigation systems, termed functional neuronavigation, is still in its infancy (i.e. in terms of its worldwide uptake); however, it represents a promising tool for performing patient-specific surgical procedures and for optimal guidance during tumour resection. Particularly in the vicinity of cerebral masses which may be distorting anatomical landmarks, knowing the exact location of important functional areas is of critical importance for surgical outcome [46]. Clinical articles have suggested that the additional information provided by these imaging modalities via a coregistered map delivered to the neurosurgeon on a heads-up display is valuable and facilitates safe resection [6]. Current methods for the intraoperative display of tractography data generally involve preoperative clustering of certain critical fibres using an ROI approach, representing the selected fibres in a static 3-D shape and displaying the geometric body onto the structural and functional images already included in the clinical navigation system [40].
In their study, Bello et al. [3] were able to show good correlation between DTI tracking and intraoperative DES when combining the two techniques, supporting the use of fMRI/DTI intraoperatively. Several groups have assessed the effect of these techniques on resection procedures with an impact on the definition of resection margins seen in 64 and 68 % in two surgical series, respectively [48, 49]. In these two series, the techniques themselves had an impact in 80 and 82 % of respective cases with the authors citing the improvement of pre-existing symptoms and the absence of any lasting deficits in the postoperative phase as confirming the value of the technique. Nimsky et al. [39] concurred with this point, arguing that DTI-based navigation allowed extended resections with low likelihood of new postoperative defects, with only one patient (or 2.8 % of the sample) showing neurological deterioration postoperatively. By using these techniques in neuronavigation systems via the coregistration of fibre tract data with standard anatomic data, they were able to use it to good effect in 16 patients with tumours close to the pyramidal tract or optic radiation [40, 44]. While it involved a smaller study cohort, Rasmussen et al. [46] found fMRI/DTI to be useful in two out of the four patients for which these techniques were used during resection, albeit with intraoperative ultrasonography for guidance. To our knowledge, only one prospective randomised trial examining the clinical impact of DTI data on the degree of tumour resection, clinical outcome and survival has been published. In their study of 238 eligible patients with high-grade gliomas, Wu et al. [60] found that patients harbouring these types of lesions had increased tumour resection, improved postoperative outcome and extended survival when DTI data were used to navigate intraoperatively in comparison to the control group who underwent surgery with conventional neuronavigation using MRI data only. Despite this, opinions regarding DTI in neuronavigation are divided, with Buchmann et al. [9] claiming that the impact of DTI data on their case series was minimal. In this study, it was intraoperative DES that influenced resection strategy, although, by their own admission, tumour borders in their patient group were easily discernible and separate from critical WM bundles such as the corticospinal tract.
With a few but growing number of more recent exceptions, most of the literature has implemented frameless stereotactic neuronavigation techniques that rely on preoperative fMRI/DTI scan images. This can be problematic as tissue deformation and brain shift during the course of the surgery result in the loss of spatial congruency between cerebral structures and preoperative images, thereby severely limiting anatomic accuracy. With regards to brain shift, there have been three main types described [37]. Type-I shift is a local outward bulging that occurs after the skull and dura are opened but before a mass lesion is resected; type-II shift is a local collapse of the brain tissue into the space previously occupied by the tumour; and type-III shift is related to loss of cerebrospinal fluid or brain dehydration and is considered to be due to a general loss of brain volume. No mathematical model currently exists that can accurately compensate for brain shift, as it is generally held that it occurs nonuniformly across different brain regions. According to Nimsky et al. [41], the extent of brain shift for WM tracts in patients undergoing tumour resection has been shown to vary from an inward shift of 8 mm to an outward shift of 15 mm. In a separate paper, the same author reported that the absolute degree of shifting correlated with tumour volume and that the direction of white matter tract shifting, whether inward or outward with respect to the craniotomy opening, displayed no such correlation or pattern [42]. While the neurosurgeon may be able to correct for brain shift intuitively [6] or use repeated landmark checks [3], its nonuniform nature has led some groups to state that it is impossible to acquire useful data from preoperative imaging about the position of WM tracts once the dura has been opened [54]. Automatic correction with intraoperative imaging is seen by many as therefore imperative to proper accuracy. The most commonly available systems to provide image updates and registration are intraoperative MRI, computed tomography and intraoperative ultrasonography [38]. Other issues include the possibility of image registration errors and distortion when DTI data are implanted into a neuronavigational system which has led to the recommendation of a safety margin of about 5 mm to be taken into account when approaching eloquent tracts [40–42]. Others speak of a ‘golden rule’ or safe resection distance between tumour and an eloquent structure. Haberg et al. [19], for example, have shown that the risk of postoperative loss of function was significantly lower when the distance between tumour border and region of functional localisation was 10 mm or more. Nimsky et al., on the other hand, proposed a distance of 5 mm as reliable when dealing with tumours near the pyramidal tract [43]. The margin may nonetheless vary in noncentral areas of the brain due to the typical distortion of echo planar images in proximity to the skull base and vault. Another source of error in the intraoperative system that must be taken into account includes the optical tracking error of the surgical tool tip. Peritumoural oedema and fibre crossing remain important issues, with the former being shown to potentially lead to failure to reconstruct a fibre pathway despite the presence of intact axonal structures in that region [61]. FA threshold is another important consideration in the context of WM tract reconstruction with Stadlbauer et al. [55], showing that different FA thresholds can have marked effects on the representation fibres in the vicinity of gliomas. They demonstrated that an increase in the FA threshold increases the distance between the reconstructed fibre bundles and the tumour and, conversely, reduced the number of detectable fibre bundles. This result could have significant effects on a patient’s surgical outcome.
In those patients able to undergo awake craniotomy, at the very least, these techniques can be used in conjunction with DES due to the complementary information they provide. This information also has the potential to reduce surgical time by guiding DES. What is more, DTI information is achieved so quickly and noninvasively, and places no extra stress on the patient who may themselves be in a state of heightened anxiety [35]. In patients who cannot undergo awake craniotomy, then fMRI and/or DTI is essential, as the surgeon must rely exclusively on this form of mapping during the surgery. Further, emerging techniques such as turboprop-DTI [1], stereoscopic virtual reality technology [45] and high angular resolution diffusion methods appear to promise improvements in modelling brain shift and fibre crossing [18, 30].
Conclusion
Hitherto, the extant literature supports the notion that the use of fMRI and DTI for preoperative planning and functional neuronavigation is beneficial for both the neurosurgeon and patient as it enables localisation of eloquent areas, formulation of a patient-specific approach and increased resection of brain lesions with reduced risk of iatrogenic neurological deficits. However, its current use is largely restricted to specialist institutions with the necessary infrastructure (including the local technical support from physicists and imaging specialists) required to maintain a powerful and clinically useable technique. While there are various considerations to bear in mind, the feeling is that, given that no single mapping technique is able to engender all information, a confluence of information will enable better patient outcomes. Interindividual variability and distortion due to tumour mass effect make purely anatomical references, in the context of recent technological advancements, insufficient. The effort to acquire the additional information on the part of the patient is negligible as the DTI scan can be acquired in a few more minutes in the same scan session in which all the other necessary images for the surgery are acquired (anatomical and fMRI data) [27]. The data processing is performed offline with dedicated software packages without involvement of the patient. These are all factors that make this technology attractive. Shortcomings such as an inability to model brain shift and fibre crossing remain key sticking points, but progress is being made within these areas [1, 18, 45]. The fact that there is no consistency in the use of paradigms, that different centres use different paradigms to identify the same brain functions [9] and that preprocessing and analysis is such a user-defined process also sees hesitance towards the techniques’ accuracy. Regardless, the complementary information provided by fMRI and DTI represents a quantitative overview of both the structural integrity of the WM and the functional status of the interconnected relevant cortical areas that may in some way affect the tumour. This information can be used not only to enhance presurgical planning and intraoperative decision making but also to predict postoperative course and thus improve patient counselling.
References
Arfanakis K, Gui M, Lazar M (2005) Optimization of white matter tractography for pre-surgical planning and image-guided surgery. Oncology Reports 15:1061–1064
Basser P, Pajevic S, Pierpaoli C, Duda J, Aldroubi A (2000) In vivo fiber tractography using DT-MRI data. Magn Reson Med 44(4):625–632
Bello L, Gambini A, Castellano A, Carrabba G, Acerbi F, Fava E, Giussani C, Cadioli M, Blasi V, Casarotti A, Papagno C, Gupta AK, Scotti G, Falini A (2008) Motor and language DTI fiber tracking combined with intraoperative subcortical mapping for surgical removal of gliomas. NeuroImage 39:369–382
Berman J, Berger M, Mukherjee P, Henry R (2004) Diffusion tensor imaging-guided tracking of fibres of the pyramidal tract combined with intraoperative cortical stimulation mapping in patients with gliomas. J Neurosurg 101:66–72
Berntsen E, Rasmussen I-A, Samuelsen P, Xu J, Haraldseth O, Lagopoulos J, Malhi G (2006) Putting the bran in jeopardy: a novel comprehensive and expressive language task? Acta Neuropsychiatrica 18:115–119
Berntsen EM, Gulati S, Solheim O, Kvistad KA, Torp SH, Selbekk T, Unsgard G, Haberg AK (2010) Functional magnetic resonance imaging and diffusion tensor tractography incorporated into an intraoperative 3-dimentional ultrasound-based neuronavigation system: impact on therapeutic strategies, extent of resection, and clinical outcome. Neurosurgery 67:251–264
Bick AS, Mayer A, Levin N (2011) From research to clinical practice: implementation of functional magnetic imaging and white matter tractography in the clinical environment. J Neurol Sci. doi:10.1016/j,jns2011.07.040
Bookheimer S (2007) Pre-surgical language mapping with functional magnetic resonance imaging. Neuropsychol Rev 17(2):145–155
Buchman N, Gempt J, Stoffel M, Foerchler A, Meyer B, Ringel F (2011) Utility of diffusion tensor-imaged (DTI) motor fiber tracking for the resection of intracranial tumours near the corticospinal tract. Acta Neurochir 153:68–74
Cao Z, Lv J, Wei X, Quan W (2010) Appliance of preoperative diffusion tensor imaging and fiber tractograhy in patients with brainstem lesions. Neurology India 58(6):886–889
Castellano A, Bello L, Michelozzi C, Gallucci M, Fava E, Iadanza A, Riva M, Casaceli G, Falini A (2011) Role of diffusion tensor magnetic resonance tractography in predicting the extent of resection in glioma surgery. Neuro-Oncology. doi:10.1093/neuronc/nor188
Catani M, Jones D, Donato R, Ffytche D (2003) Occipitotemporal connections in the human brain. Brain 126:2093–2107
Desmond J, Sum J, Wagner A, Demb J, Shear P, Glover G, Gabrieli J, Morrell M (1995) Functional MRI measurement of language lateralization in Wada-tested patients. Brain 118:1411–1419
Douek P (1991) MR color mapping of myelin fiber orientation. J Comput Assist Tomogr 15(6):923–929
Elhawary H, Liu H, Patel P, Norton I, Rigolo L, Papademetris X, Hata N, Golby A (2011) Intraoperative real-time querying of white matter tracts during frameless stereotactic neuronavigation. Neurosurgery 68:506–516
Fernandez-Miranda JC, Engh JA, Pathak SK, Madhok R, Boada FE, Schneider W, Kassam AB (2010) High-definition fiber tracking guidance for intraparenchymal endoscopic port surgery. J Neurosurg 113:990–999
Filler A (2009) Magnetic resonance neurography and diffusion tensor imaging: origins, history, and clinical impact of the first 50000 cases with an assessment of efficacy and utility in a prospective 5000-patient study group. Neurosurgery 65:A29–A43
Frank L (2002) Characterization of anisotropy in high angular resolution diffusion-weighted MRI. Magn Reson Med 47(6):1083–1099
Haberg A, Kvistad K, Unsgard G, Haraldseth O (2004) Preoperative blood oxygen level-dependent functional magnetic resonance imaging in patients with primary brain tumours: clinical application and outcome. Neurosurgery 54:902–914
Hagmann P, Thuran J, Jonasson L, Vandergheynst P, Clarke S, Maeder P et al (2003) DTI mapping of human brain connectivity: statistical fiber tracking and virtual dissection. NeuroImage 19(3):545–554
Holodny AI, Watts R, Korneinko VN, Pronin IN, Zhukovskiy ME, Gor DM, Ulug A (2005) Diffusion tensor tractography of the motor white matter tracts in man. Annals of the New York Academy of Science 1064:88–97
Hou B, Bradbury M, Peck K, Petrovich N, Gutin P, Holodny A (2006) Effect of brain tumour neovasculature defined by rCBV on BOLD fMRI activation volume in the primary motor cortex. NeuroImage 32(2):489–497
Hunsche S, Moseley M, Stoeter P, Hedehus M (2001) Diffusion-tensor MR imaging at 1.5 and 3.0 T: initial observations. Radiology 221:550–556
Jakab A, Molnar P, Emri M, Berenyi E (2011) Glioma grade assessment by using histogram analysis of diffusion tensor imaging-derived maps. Neuroradiology 53(7):483–491
Jellison B, Field A, Medow J, Lazar M, Salamat M, Alexander A (2004) Diffusion tensor imaging of cerebral white matter: a pictorial review of physics, fiber tract anatomy and tumor imaging patterns. Am J Neuroradiol 25(3):356–369
Jones D (2003) Determining and visualizing uncertainty in estimates of fiber orientation from diffusion tensor MRI. Magn Reson Med 49:7–12
Kleiser R, Staempfli P, Valvanis A, Boesiger P, Kollias S (2010) Impact of fMRI-guided advanced DTI fiber tracking techniques on their clinical applications in patients with brain tumours. Neuroradiology 52:37–46
Krings T, Reinges M, Erberich S, Keremy S, Rohde V, Spetzger U, Korinth M, Willmes K, Gilsbach J, Thron A (2001) Functional MRI for presurgical planning: problems, artefacts, and solution strategies. J Neurol Neurosurg Psychiatry 70:749–760
Laurienti P, Field A, Burdette J, Maldjian J, Yen Y, Moody D (2002) Dietary caffeine consumption modulates fMRI measures. NeuroImage 17:751–757
Lazar M (2010) Mapping brain anatomical connectivity using white matter tractography. NMR Biomed 23:821–835
Lee C, Ward H, Sharbrough F et al (1999) Assessment of functional MR imaging in neurosurgical planning. Americal Journal of Neuroradiology 20:1511–1519
Li Z-X, Dai J (2007) Functional MRI and diffusion tensor tractography in patients with brain gliomas involving motor areas: clinical application and outcome. Biomedical Imaging and Intervention Journal 3:612–618
Lu H, Zhao C, Ge Y, Lewis-Amezcua K (2008) Baseline blood oxygenation modulates response amplitude: physiologic basis for intersubject variations in functional MRI signals. Magn Reson Med 60(2):364–372
Majos A, Tybor K, Stefanczyk L, Goraj B (2005) Cortical mapping by functional magnetic resonance imaging in patients with brain tumors. Eur J Radiol 15:1148–1158
Mikuni N, Okada T, Nishida N, Taki J, Enatsu R, Ikeda A, Miki Y, Hanakawa T et al (2007) Comparison between motor evoked potential recording and fiber tracking for estimating pyramidal tracts near brain tumours. J Neurosurg 106(1):128–133
Misaki T, Beppu T, Inoue T, Ogasawara K, Ogawa A, Kabasawa H (2004) Use of fractional anisotropy value by diffusion tensor RI for preoperative diagnosis of astrocytic tumours: case report. J Neurooncol 70:343–348
Nauta H, Bonnen J, Bogner M, Charles S, Grundfest W, Harrington J (1998) Problem of intraoperative anatomical shift in image-guided surgery. SPIE Proc Ser 3262:229–233
Ng WH, Mukhida K, Rutka JT (2010) Image guidance and neuromonitoring in neurosurgery. Childs Nervous System 26:491–502
Nimsky C, Ganslandt O, Enders F, Merhof D, Fahlbusch R (2005) Visualization strategies for major white matter tracts identified by diffusion tensor imaging for intraoperative use. Int Congr Ser 1281:793–797
Nimsky C, Ganslandt O, Fahlbusch R (2007) Implementation of fiber tract neuronavigation. Neurosurgery 55:160–164
Nimsky C, Ganslandt O, Hastreiter P et al (2005) Intraoperative diffusion-tensor MR imaging: shifting of white matter tracts during neurosurgical procedures: initial experience. Radiology 234(1):218–225
Nimsky C, Ganslandt O, Hastreiter P, Wang R, Benner T, Sorensen A, Fahlbusch R (2005) Preoperative and intraoperative diffusion tensor imagin-based fiber tracking in glioma surgery. Neurosurgery 56:130–138
Nimsky C, Gaslandt O, Merfhor D et al (2006) Intraoperative visualization of pyramidal tract by diffusion-tensor-imaging-based fiber tracking. NeuroImage 30:1219–1229
Nimsky C, Grummich P, Sorensen A, Fahlbusch R, Ganslandt O (2005) Visualization of the pyramidal tract in glioma surgery by integrating diffusion tensor imaging in functional neuronavigation. Zentralbl Neurochir 66:133–141
T-m Q, Zhang Y, Wu J-S, Tang W-J, Zhao Y, Pan Z-G, Mao Y, Zhou L-F (2010) Virtual reality presurgical planning for cerebral gliomas adjacent to motor pathways in an integrated 3-D stereoscopic visualization of structural MRI and DTI tractography. Acta Neurochir 152:1847–1857
Rasmussen I-A Jr, Lindeth F, Rygh O, Berntsen E, Selbekk T, Xu J, Hernes TN, Harg E, Haberg A, Unsgaard G (2007) Functional neuronavigation combined with intra-operative 3D ultrasound: Initial experiences during surgical resections close to eloquent brain areas and future directions in automatic brain shift compensation of preoperative data. Acta Neurochir (Wien) 149:365–378
Rohde G, Barnett A et al (2004) Comprehensive approach for correction of motion and distortion in diffusion-weighted MRI. Magn Reson Med 51(1):103–114
Romano A, D'Andrea G, Minniti G, Mastronardi L, Ferrante L, Fantozzi L, Bozzao A (2009) Pre-surgical planning and MR-tractography utility in brain tumour resection. Eur J Radiol 19:2797–2808
Romano A, Ferrante M, Cipriani V, Fasoli F, Ferrante L, D'Andrea G, Fantozzi L, Bozzao A (2007) Role of magnetic resonance tractography in the preoperative planning and intraoperative assessment of patients with intra-axial brain tumours. La Radiologia Medica 112:906–920
Roux F, Boulanouar K, Lotterie J, Mejdoubi M, Sage JL, Berry I (2003) Language functional magnetic resonance imaging in preoperative assessment of language areas: correlation with direct cortical stimulation. Neurosurgery 52(6):1335–1345
Schonberg T, Pianka P, Hendler T, Pasternak O, Assaf Y (2006) Characterization of displaced white matter by brain tumours using combined DTI and fMRI. NeuroImage 30:1100–1111
Schreiber A, Hubbe U, Ziyeh S, Hennig J (2000) The influence of gliomas and nonglial space-occupying lesions on blood-oxygen-level-dependent contrast enhancement. Americal Journal of Neuroradiology 21:1055–1063
Skirboll S, Ojeman G, Berger M, Lettich E, Winn H (1996) Functional cortex and subcortical white matter located within gliomas. Neurosurgery 38:678–685
Spena G, Nava A, Cassini F, Pepoli A, Bruno M, D'Agata F, Cauda F, Sacco K, Duca S, Barletta L, Versari P (2010) Preoperative and intraoperative brain mapping for the resection of eloquent-area tumours. A prospective analysis of methodology, correlation, and usefulness based on clinical outcomes. Acta Neurochirugica 152:1835–1846
Stadlbauer A, Nimsky C, Buslei R, Salomonowitz E, Hammen T, Buchfelder M, Moser E, Ernst-Stecken A, Ganslandt O (2007) Diffusion tensor imaging and optimized fiber tracking in glioma patients: histopathologic evaluation of tumour-invaded white matter structures. NeuroImage 34(3):949–956
Sunaert S (2006) Presurgical planning for tumour resectioning. J Magn Reson Im 23:887–905
Sunaert S, Hecke PV, Marchal G, Orban G (2000) Attention to speed of motion, speed discrimination and task difficulty: an fMRI study. NeuroImage 11:612–623
Tharin S, Golby A (2007) Functional brain mapping and its applications to neurosurgery. Operative Neurosurgery 60(2):185–202
Ulmer J, Hacein-Bey L, Matthews V, Mueller W, DeYoe E, Prost R, Robert W, Meyer G, Krouwer H, Schmainda K (2004) Lesion-induced pseudo-dominance at functional magnetic resonance imaging: implications for preoperative assessments. Neurosurgery 55(3):569–579
Wu J-S, Mao Y, Zhou L-F, Tang W-J, Hu J, Song Y-Y, Hong X-N, Du G-H (2007) Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: a prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery 61:935–949
Yu CS, Li KC, Xuan Y, Ji XM, Qin W (2005) Diffusion tensor tractograhy in patients with cerebral tumours: a helpful technique for neurosurgical planning and postoperative assessment. Eur J Radiol 56:197–204
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Mario Giordano, Hannover, Germany
In the present review the authors deal with a very actual topic in the field of neurosurgery and neuroimaging. Functional magnetic resonance imaging (fMRI) has become fundamental in surgery of intra-axial lesions adjacent to eloquent cortical areas both for preoperative planning and intraoperative guidance. However care should be taken to preserve also white matter connections of these regions in order to avoid postoperative neurological deficits.
In this scenario, diffusion tensor imaging (DTI) provides information about the normal course or the displacement of fibre tracts near the tumour allowing a noninvasive tracing of the main white matter bundles in the human brain.
Combination of both techniques with intraoperative navigation has been applied successfully in many institutions, but its diffusion is still limited. For this reason, is important for the neurosurgical community to be familiar with the basis of these techniques as well as the complete workflow from imaging to surgery. The present review tries to achieve this result in a schematic and simple way describing the technical bases and practical use of both fMRI and DTI techniques. The paper has a ‘textbook’ layout that improves its readability, reaching its educational purpose.
Christopher Nimsky, Marburg, Germany
This review by Dimou et al. gives an overview on current preoperative strategies to locate cortical and subcortical eloquent brain areas. Preoperative fMRI and DTI investigations have become routine in many neurosurgical centres for lesions close to eloquent brain regions.
Integration of these data into a navigation setup leads to so-called functional navigation, allowing intraoperative identification of these eloquent structures. This concept of functional navigation is also open to integrate further modalities like MR spectroscopy, PET, transcranial magnetic stimulation, etc., resulting in the so-called multimodal navigation.
Besides the knowledge on effects related to patient registration accuracy and intraoperative events such as brain shift, all of them decreasing the accuracy of navigation, it is important that the neurosurgical user also has a profound knowledge on the technology behind these data. Otherwise, severe misinterpretations might lead to erroneous tracking results, finally causing unwanted neurological postoperative deficits. It is important to look at the raw data, as well as the strategies on how these data are analysed. The integration of fMRI and DTI packages into commercial navigation systems increases the broad availability; however, the inexperienced user is at risk to reconstruct white matter connections and find fMRI activations that do not relate to the real anatomy. Furthermore, the user has to take into account that the raw data are distorted to some extent. Additional hulls around the reconstructed objects representing major white matter tracts are a possibility to visualise safety margins, which ideally would vary in thickness respective to the quality and reliability of the reconstructed fibre bundle. In case of noisy unreliable data, a thick hull should be added, while in the highly reliable data, the hull could be thinner. The technical, as well as clinical definition of the extent of these safety margins is still under investigation. Maximal safety requires combining electrophysiological brain mapping with functional navigation that integrates fMRI data and DTI-based fibre tracking acquired before and also during surgery.
Rights and permissions
About this article
Cite this article
Dimou, S., Battisti, R.A., Hermens, D.F. et al. A systematic review of functional magnetic resonance imaging and diffusion tensor imaging modalities used in presurgical planning of brain tumour resection. Neurosurg Rev 36, 205–214 (2013). https://doi.org/10.1007/s10143-012-0436-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-012-0436-8