
Abstract
Suboptimal placements of pedicle screws may lead to neurological and vascular complications. Computer-assisted image guidance has been shown to improve accuracy in spinal instrumentation. Checking the accuracy of the navigation system during pedicle screw placement is fundamental. We describe a novel technique of using continuous accuracy check of the navigation system during O-arm-based neuronavigation to instrument the thoracolumbar region. Forty thoracic and 42 lumbar screws were inserted in 12 patients. The Mirza evaluation system was used to evaluate the accuracy of the inserted screws. There was no neurological injury and no need to reposition any screw. The accuracy of the screws placement was excellent. Our technique of continuous at will operational accuracy check of the neuronavigation system is associated with extreme accuracy of screw placement, no need to bring a patient back to the operating room to reposition a pedicle screw, and with excellent outcome.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pedicle screws are widely implanted in the thoracolumbar area for a variety of pathological processes, traumatic and not [5]. Suboptimal placements of pedicle screws may lead to neurological and vascular complications, potentially requiring reoperation [1, 2, 6, 11, 15].
Pedicle screws are placed either free hand following anatomical landmarks, often augmented by intraoperative fluoroscopy, or using spine navigation based on intraoperative fluoroscopy or computerized tomography (CT) [1–3, 8, 10, 14, 17, 18].
The CT scans for spine navigation are most often acquired pre-operatively, even though recent reports have used intraoperative CT-based navigation [6, 7, 11].
The O-arm® Surgical Imaging System (Medtronic, Minneapolis, MN, USA) provides high-definition 3-D, multi-plane fluoroscopic images that can be automatically registered to a stealth neuronavigation station (Medtronic, Minneapolis, MN, USA) in a time-efficient process. As with any navigation system, it is imperative to assess the operational accuracy of the system while it is being used [12].
We describe our novel technique to continuously check the operational accuracy of the navigation system during thoracolumbar pedicle screw placement using O-arm-based neuronavigation.
Materials and methods
Patient population
We used the combination O-arm-stealth for intraoperative spine navigation during the placement of thoracolumbar pedicle screws in 12 patients in which a total of 82 screws were inserted. Table 1 details the levels of the spine that were instrumented. Six patients had traumatic injuries (four in the thoracic and two in the lumbar areas) while six patients had degenerative disease (all in the lumbosacral area). Nine patients underwent decompression and fusion and three patients underwent only fusion. All patients underwent post-procedural intraoperative O-arm imaging. All patients underwent post-operative thin slices control CT scan of the instrumented area (usually between 3 and 6 months). Follow-up ranged from 4 to 24 months (mean and median follow-up: 20 months).
O-arm and stealth navigation
The O-arm (Medtronic, Minneapolis, MN, USA) is an imaging system that incorporates a flat panel detector and can provide standard fluoroscopic images or 3-D, volumetric high-definition fluoroscopic images. This dataset can be downloaded to a stealth workstation (Stealth Station, Medtronic, Minneapolis, MN, USA) where it is automatically registered and readied for navigation in about 55 s.
Operative technique
The following algorithm was used :
-
Step 1: Preparation
After the patient was positioned prone on the operating room table, the O-arm was used in a conventional X-ray mode to center the area of interest (spine segments to be navigated) in the anteroposterior and lateral plane.
Next, small, 5-mm, linear incisions were made over the tips of the spinous processes of the spine segments to be navigated and 4-mm-self drilling micro-screws (Synthes, West Chester, PA ) were implanted into the exposed tip of the spinous processes. These micro-screws were to be used as reference points (internal fiducials) for verification and evaluation of the operational accuracy of the navigation system during every step of the surgery. In the lumbar spine, the navigation tracker was affixed in the iliac spine or on the cranial or caudal spinous process while in the thoracic area it was affixed on the cranial or caudal spinous process.
-
Step 2. Image acquisition
The spinal segment of interest was scanned using the O-arm and the images were automatically registered to the Stealth Station.
-
Step 3. Accuracy verification
The tip of the navigation pointer was placed on the head of the internal fiducials (spinous processes micro-screws) to assess operational accuracy. Operational accuracy was judged to be good when no difference was found between the navigation pointer tip position in patient’s space and the navigation pointer tip position in image space. (Fig. 1).
Fig. 1 
Accuracy verification. The tip of the navigation pointer is placed on the head of the internal fiducial (spinous processes micro-screw) to assess operational accuracy
If there is misalignment between these two positions we look for possible errors (smudged tracking balls, tracking instrument malfunction, etc.) and correct them.
-
Step 4: Pedicle screws placement
A navigated Pak needle was then introduced percutaneously using a short (1 cm) paramedian incision to make contact with the bone of the lateral elements of the spine. Once the Pak needle was in alignment with a suitable trajectory to enter the pedicle, we impacted it into the bone using a hammer (Fig. 2). We hammered the Pak needle well into the vertebral body. We then removed its stylet and placed a K wire through the needle. The K wire was slightly tapped into the bone advancing it a couple of millimeters from the tip of the needle. The Pak needle was then removed and a navigated tapper of appropriate size was used to tap into the vertebral body under continuous navigation guidance (Fig. 3). Next, the appropriate screw was selected and loaded on the percutaneous screw carrier. The insertion of the screw was again monitored using image guidance by navigating the screw carrier carrying on its tip the appropriate virtual screw (Fig. 4). Once the screw was inserted, the K wire was removed. Anytime we used a navigated instrument we double checked the operational accuracy according to step 3.
Fig. 2 
The navigated Pak needle is at the entry point
Fig. 3 
The navigated tapper is shown entering the vertebral body
Fig. 4 
The insertion of the screw is again monitored using image guidance by navigating the screw carrier that has on its tip the appropriate virtual screw
-
Step 5: Assessment of the position of the placed screws
After all the pedicle screws were inserted, we obtained another O-arm high-definition scan to check on the pedicle screws position (Fig. 5 left). We used the Mirza et al. scoring system to evaluate and assess the position of the inserted screw [10].
Fig. 5 
Post-procedural intraoperative O-arm scan showing good position of pedicle screws(left) and thin-slice post-operative CT of the same level (right). Both images yield comparable information
-
Step 6
Once we were done with pedicle screws placement, we proceeded with the rest of the operation that included posterior fusion with or without decompression.





Results
Overall, 82 screws (40 in the thoracic region and 42 in the lumbosacral area ) were placed in 12 patients (Table 1).
No patient experienced any complication related to pedicle screws placement. We repositioned two screws during surgery because the screws had minimal (less than 2 mm) lateral pedicle cortex breech.
None of the screws needed to be repositioned after surgery and hence no patient was brought back to the OR for screws repositioning. The post-operative thin slices CT did not yield any different information than the post-procedural intraoperative O-arm (Fig. 5).
All of our screws were in excellent position according to Mirza’s evaluation system [10].
The implanted internal fiducials were visualized very well and very easily in all the 3-D images. The operational navigation accuracy assessed using the internal fiducials was found to be excellent. The number of trajectories available to place pedicle screws using our technique was plentiful and we were able to take best advantage of each vertebra different anatomy.
Discussion
Free hand or conventional fluoroscopy-based pedicle screw placement is associated with suboptimal pedicle screw placement in 5–55 % of cases [1, 4, 6, 11, 13],while the incidence of anatomical injuries and reoperation is of 6.9–8 % [2, 5] and 4–8.8 %, respectively [1, 15, 16]. With the advent of navigation-based pedicle screws placement, the incidence of these events has decreased [18].
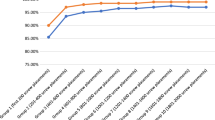
It is clear that navigation helps in improving the accuracy of pedicle screws placement. A recent meta-analysis report gives a median accuracy of 93.7 % (range 72 to 100 %) with navigation versus a median accuracy of 86.6 % (range 27 to 100 %) when navigation is not used [9].
One advantage of navigation based on intraoperative image data set acquisition (3-D fluoro or intraoperative CT) versus navigation based on pre-operative image acquisition is that the former is performed with the image acquired with the patient in the surgical position, therefore decreasing spine segments motion. In addition, the former may allow for multiple level registrations at once and does not need presence of the posterior elements of the spine, making navigation doable in revision cases [11, 19].
When one looks at the overall cost associated with placement of pedicle screws using navigation based on intraoperative image acquisition, the significant capital equipment investment of an intraoperative imaging machine, about $600,000 in the O-arm case, must be balanced by the total cost (expenses and loss of professional revenues) linked to the need of bringing a patient back to the operating room to reposition a pedicle screw. This total cost may be as high as $15,000–20,000. This is in addition to the extra cost that may be associated with treatment of injuries linked to malpositioned pedicle screws. Moreover, there is an extra value provided to the patient by avoiding neurological injuries and a second surgical procedure.
Our technique is novel because it allows for at will check of the operational accuracy, using our implanted internal fiducials, therefore controlling for errors due to instrument malfunction or system failure. As the internal fiducials were placed on each segment to be instrumented and as the spinal segment represent a volumetric unit, we felt that excellent accuracy at the tip of the spinous process would translate into excellent operational accuracy throughout that spine segment; our results seem to validate this assumption [5]. Our technique may represent an useful addition to existing technique to use neuronavigation to place pedicle screws.
Conclusions
The accuracy of pedicle screw placement in the thoracolumbar area is enhanced by using our proposed algorithmic step wise technique that includes at will check of the operational accuracy of the navigation system while utilizing the O-arm and Stealth Station. Our proposed algorithmic technique allows for efficient check of intraoperative navigational accuracy and for use of a wide variety of pedicle screws entry points.
References
Amato V, Giannachi L, Irace C, Corona C (2010) Accuracy of pedicle screw placement in the lumbosacral spine using conventional technique: computed tomography postoperative assessment in 102 consecutive patients. J Neurosurg Spine 12(3):306–313. doi:10.3171/2009.9.SPINE09261
Beck M, Mittlmeier T, Gierer P, Harms C, Gradl G (2009) Benefit and accuracy of intraoperative 3D-imaging after pedicle screw placement: a prospective study in stabilizing thoracolumbar fractures. Eur Spine J 18(10):1469–1477. doi:10.1007/s00586-009-1050-5
Benzel EC, Rupp FW, McCormack BM, Baldwin NG, Anson JA, Adams MS (1995) A comparison of fluoroscopy and computed tomography-derived volumetric multiple exposure transmission holography for the guidance of lumbar pedicle screw insertion. Neurosurgery 37(4):711–716
Berry E, Cuppone M, Porada S, Millner PA, Rao A, Chiverton N, Seedhom BB (2005) Personalised image-based templates for intra-operative guidance. Proc Inst Mech Eng H 219(2):111–118
Bjarke Christensen F, Stender Hansen E, Laursen M, Thomsen K, Bunger CE (2002) Long-term functional outcome of pedicle screw instrumentation as a support for posterolateral spinal fusion: randomized clinical study with a 5-year follow-up. Spine (Phila Pa 1976) 27(12):1269–1277
Bledsoe JM, Fenton D, Fogelson JL, Nottmeier EW (2009) Accuracy of upper thoracic pedicle screw placement using three-dimensional image guidance. Spine J 9(10):817–821
Glossop ND, Hu RW, Randle JA (1996) Computer-aided pedicle screw placement using frameless stereotaxis. Spine (Phila Pa 1976) 21(17):2026–2034
Hart RA, Hansen BL, Shea M, Hsu F, Anderson GJ (2005) Pedicle screw placement in the thoracic spine: a comparison of image-guided and manual techniques in cadavers. Spine (Phila Pa 1976) 30(12):E326–E331
Kosmopoulos V, Schizas C (2007) Pedicle screw placement accuracy: a meta-analysis. Spine (Phila Pa 1976) 32(3):E111–E120. doi:10.1097/01.brs.0000254048.79024.8b
Mirza SK, Wiggins GC, Kuntz C, York JE, Bellabarba C, Knonodi MA, Chapman JR, Shaffrey CI (2003) Accuracy of thoracic vertebral body screw placement using standard fluoroscopy, fluoroscopic image guidance, and computed tomographic image guidance: a cadaver study. Spine (Phila Pa 1976) 28(4):402–413
Nottmeier EW, Seemer W, Young PM (2009) Placement of thoracolumbar pedicle screws using three-dimensional image guidance: experience in a large patient cohort. J Neurosurg Spine 10(1):33–39. doi:10.3171/2008
Park P, Foley KT, Cowan JA, Marca FL (2010) Minimally invasive pedicle screw fixation utilizing O-arm fluoroscopy with computer-assisted navigation: feasibility, technique, and preliminary results. Surg Neurol Int 1:44. doi:10.4103/2152-7806.68705
Rajasekaran S, Vidyadhara S, Ramesh P, Shetty AP (2007) Randomized clinical study to compare the accuracy of navigated and non-navigated thoracic pedicle screws in deformity correction surgeries. Spine (Phila Pa 1976) 32(2):E56–E64
Rampersaud YR, Lee KS (2007) Fluoroscopic computer-assisted pedicle screw placement through a mature fusion mass: an assessment of 24 consecutive cases with independent analysis of computed tomography and clinical data. Spine (Phila Pa 1976) 32(2):217–222
Schizas C, Michel J, Kosmopoulos V, Theumann N (2007) Computer tomography assessment of pedicle screw insertion in percutaneous posterior transpedicular stabilization. Eur Spine J 16(5):613–617
Schwender JD, Holly LT, Rouben DP, Foley KT (2005) Minimally invasive transforaminal lumbar interbody fusion (TLIF): technical feasibility and initial results. J Spinal Disord Tech 18(Suppl):S1–S6
Sugimoto Y, Ito Y, Tomioka M, Shimokawa T, Shiozaki Y, Mazaki T, Tanaka M (2010) Clinical accuracy of three-dimensional fluoroscopy (IsoC-3D)-assisted upper thoracic pedicle screw insertion. Acta Med Okayama 64(3):209–212
Tian NF, Xu HZ (2009) Image-guided pedicle screw insertion accuracy: a meta-analysis. Int Orthop 33(4):895–903. doi:10.1007/s00264-009-0792-3
Tormenti MJ, Kostov DB, Gardner PA, Kanter AS, Spiro RM, Okonkwo DO (2010) Intraoperative computed tomography image-guided navigation for posterior thoracolumbar spinal instrumentation in spinal deformity surgery. Neurosurg Focus 28(3):E11
Conflict of interest
None of the authors has any conflict of interest concerning the financial, materials, or methods used in this study or the findings specified in this paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Alexander Brawanski, Regensburg, Germany
The authors propose an interesting method to increase the accuracy of the placemant of pedicle screws. There are several other methods to increase accuracy, their’s is an interesting alternative.
Rights and permissions
About this article
Cite this article
Ammirati, M., Salma, A. Placement of thoracolumbar pedicle screws using O-arm-based navigation: technical note on controlling the operational accuracy of the navigation system. Neurosurg Rev 36, 157–162 (2013). https://doi.org/10.1007/s10143-012-0421-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-012-0421-2