
Abstract
A 21-year-old man presented with ankle pain after a motor vehicle accident. Imaging revealed an acute fracture of the os trigonum in addition to multiple, other lower-extremity fractures. In this case, the fracture of the os trigonum was a result of a significant traumatic injury. Thus, the presence of this fracture in an acute setting should prompt a search for other associated fractures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute fracture of the os trigonum is a rare occurrence. To our knowledge, only three cases have been reported in the English literature [1, 2]. Fractures of the posterior process of the talus, most commonly the lateral tubercle, are more frequently seen and are typically secondary to a plantar flexion or inversion mechanism [2, 3]. We report a case of fracture of an os trigonum that was associated with multiple, other lower-extremity injuries indicating a high-energy trauma.
Case report
A 21-year-old unrestrained male passenger was involved in a rollover motor vehicle accident and was found on the scene partially ejected from the vehicle and unconscious. Initial radiographic assessment revealed multiple injuries including pelvic and acetabular fractures, a right femoral shaft fracture, and multiple bilateral metacarpal fractures, among other injuries. Computed tomographies (CT) of the head, cervical spine, and abdomen were performed according to the trauma protocol and showed no internal injuries. The radiograph of the right ankle showed a diffuse soft-tissue swelling and a lucent defect in the os trigonum, suspicious of a fracture (Fig. 1). Because of the persistent pain, CT imaging of the foot and ankle was performed 2 days after admission, which showed a comminuted fracture of the os trigonum (Fig. 2a,b). The CT also showed a fracture through the lateral process of the talus (Fig. 2c), noted retrospectively on the initial radiograph. In addition, there was focal cortical interruption, depression, and sclerosis of the subchondral region of the talus at the anterior facet of the subtalar joint, indicating an impaction-type injury (Fig. 2d). Two months after injury, a follow-up radiograph of the right ankle showed interval healing of the os trigonum fracture (Fig. 3).

Lateral radiograph of the foot shows a linear lucency extending through an os trigonum (arrow). Margins of the fracture are not well corticated, indicating an acute fracture

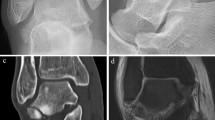
a The axial CT image shows an acute fracture of an os trigonum (arrow) with additional small fragments anterior to the os, consistent with comminuted fracture. b Sagittal CT reformatted image shows a comminuted fracture of the os trigonum (arrow). c The coronal CT reformatted image shows a fracture of the lateral process of the talus (arrow). d The axial CT image shows a cortical interruption of the head of the talus (arrow) at the anterior subtalar joint, typical for an impaction-type injury

The follow-up radiograph two months after injury shows interval healing of the os trigonum fracture (arrow). There has been fixation of the lateral talar process fracture
Discussion
A secondary ossification center of the posterior talus is usually visible in children at about age 11–13 in boys and 8–10 in girls. In most cases, the secondary ossification center fuses with the posterior surface of the talus, forming the posterior process. In some cases, the secondary center does not fuse and remains a separate bone in a skeletally mature individual, and is termed the os trigonum. The prevalence of an os trigonum ranges from 1.7 to 50% of the cases by various reports but is generally thought to be present in approximately 7% of the cases [4].
Although chronic repetitive trauma is a well-known etiology of os trigonal injury, instances of acute fracture are extremely rare. Indeed, only three cases have been reported in the English literature [1, 2].
Most instances of repetitive microtrauma to the os trigonum involve a mechanism of plantar flexion at the ankle. Thus, a similar mechanism might be proposed for acute fracture of the os trigonum. However, in our case, a coexisting lateral process fracture of the talus suggests a different mechanism. The most widely accepted mechanism for a lateral process fracture is axial loading with dorsiflexion of the foot and inversion of the ankle, although dorsiflexion and eversion [5], and dorsiflexion and external rotation [6] have recently been shown to produce this injury. Lateral talar process fractures are most commonly seen with snowboarding injuries but have been reported after high-speed impaction such as a fall from a height or motor vehicle accidents [5]. The mechanism of axial loading from high-speed impaction almost certainly provided the major force triggering the injuries in this case, as it is consistent with all three bony ankle injuries seen on the CT. The case reported by Mouhsine et al. [2] of an os trigonal fracture from an axial shock (fall from a height of 2 m) supports this theory. Unfortunately, in cases of severe motor vehicle collisions, multiple mechanisms of injury often come into play, making the determination of exact mechanism difficult. Magnetic resonance imaging may have been helpful in determining possible mechanisms by revealing patterns of contusion and associated ligamentous injuries. However, because of other more pressing injuries, this was not performed.
The treatment of the three reported cases of os trigonum fracture involved rest and attempts at cast immobilization [1, 2], similar to that of a fracture of the posterior process of the os calcis. If the fracture remains ununited, it has the potential to become a source of inflammation. In the face of recurring irritation, surgical resection of the bone itself may be required. In our case, the fracture of the lateral process of the talus took precedent over the other injuries, and that fracture was surgically reduced and immobilized.
In addition to the fracture of the os trigonum, the CT showed an impaction fracture of the head of the talus and fracture of the lateral talar process. The lateral talar process fracture was overlooked on initial radiographs, as has been reported in as many as 33–41% of the cases [3]. For this reason, the presence of an os trigonum fracture on conventional radiography should prompt a search for other associated injuries.
References
Meisenbach R (1927) Fracture of os trigonum: report of two cases. JAMA 89:199–200
Mouhsine E, Djahangiri A, Garofalo R (2004) Fracture of the non-fused os trigonum, a rare cause of hindfoot pain. A case report and review of the literature. Chir Organi Mov 89(2):171–176
Judd DB, Kim DH (2002) Foot fractures frequently misdiagnosed as ankle sprains. Am Fam Phys 66(5):785–794
McDougall A (1955) The os trigonum. J Bone Jt Surg 37B(2):257–265
Funk JR, Sreebala CM et al (2003) Snowboarder’s talus fractures experimentally produced by eversion and dorsiflexion. Am J Sports Med 31(6):921–928
Boon AJ, Smith J, Zobitz ME et al (2001) Snowboarder’s talus fracture: mechanism of injury. Am J Sports Med 29:333–338
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Escobedo, E.M., MacDonald, T.L. & Hunter, J.C. Acute fracture of the os trigonum. Emerg Radiol 13, 139–141 (2006). https://doi.org/10.1007/s10140-006-0536-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-006-0536-2