
Abstract
Identification of adhesions on computed tomography (CT) in cases of small-bowel obstruction (SBO) is currently a diagnosis of exclusion. The purpose of this study is to examine whether the presence of findings suggestive of an extraluminal band can be used as a CT sign for adhesive SBO. CT scans of 142 patients with surgically proven SBO performed within 72 h of exploratory surgery were reviewed. The studies were evaluated for the cause of SBO and the presence of extraluminal bands. An extraluminal band was considered present if there was a change in the conformation of the transition zone, suggesting extraluminal compression of the bowel by a linear obstructive band. The presence of extraluminal bands in the area of the transition zone had a high positive predictive value for adhesive SBO. Of the 73 cases in which bands were present, SBO was due to adhesions in 52 instances, with a corresponding positive predictive value of 71% (95% confidence interval 0.60–0.80) and a p value of 0.008. The extraluminal band was 61% sensitive and 63% specific for adhesive SBO. The presence of an extraluminal band on CT in the area of the transition zone in cases of SBO correlates well with a diagnosis of SBO secondary to adhesions. In the absence of a source of SBO, the presence of an extraluminal band can serve as a helpful diagnostic adjunct for adhesive SBO.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Intestinal obstruction, of which small-bowel obstruction (SBO) comprises 60–80% of cases [1], accounts for 20% of acute surgical admissions [2]. While there are many possible causes of SBO, the clinical presentation rarely indicates the exact etiology. Computed tomography (CT) has been shown to be useful in determining the site, level, and cause of obstruction [3–6]. However, adhesive bands, the most common cause of SBO, are not clearly visualized at CT [5, 7–9]. Identification of adhesions as a cause of SBO thus remains a diagnosis of exclusion that must be based on the finding of an abrupt change in bowel caliber without evidence of another cause of obstruction [5, 7, 9]. As adhesions are responsible for the majority of SBOs (50–75%), no obvious source of obstruction is seen on CT in most cases [10–12]. It is important to accurately diagnose SBO secondary to adhesions because it warrants a trial of conservative therapy (i.e., intravenous fluids, electrolyte replacement, nasogastric tube decompression, and antibiotics) unless high-grade obstruction or signs of strangulation are present [9, 13]. While adhesive bands themselves may not be identified at CT, recognition of findings suggestive of an extraluminal band compressing the bowel at the transition zone could enhance the radiologist’s ability to diagnose SBO due to adhesions. This study tests this hypothesis.
Materials and methods
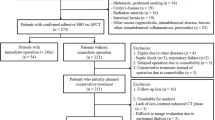
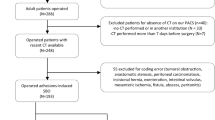
The study was conducted as a retrospective, blinded review of patients with surgically proven SBO. A computerized search of medical records at our institution between July 1998 and July 2003 revealed 990 cases with a diagnosis of possible, probable, or likely SBO on CT. Of these, 217 patients had exploratory surgery within 72 h of the CT scan. At exploratory surgery, the diagnosis of SBO was confirmed in 166 cases. From this group, 142 subjects were selected for inclusion in the study. The remaining 24 patients were excluded for the following reasons: images were not available on the Picture Archive Communication System (PACS) (n=17), surgical reports were unclear regarding the cause of obstruction (n=5), or images were too poor for diagnostic purposes due to excessive patient motion (n=2).
Institutional Review Board (IRB) approval was obtained. Written informed consent was not required for this retrospective review of medical records. An investigator not involved in interpretation of the images reviewed the medical records of all patients. The study population was identified by a retrospective review of medical charts, surgical operative reports, and radiology reports. The 142 subjects selected for inclusion in the study were divided into two groups based on intraoperative findings: those in whom adhesions were a cause of SBO and those with SBO secondary to other causes. The adhesive SBO group was composed of 85 subjects (34 men and 51 women) with an age range of 18–97 (mean, 56.28). The nonadhesive SBO group consisted of 57 subjects (24 men and 33 women) with an age range of 18–95 (mean, 55.96). Surgical diagnoses in the nonadhesive SBO group included SBO secondary to external hernia (n=19), neoplasm (n=14), volvulus (n=9), internal hernia (n=8), appendicitis/intra-abdominal abscess formation (n=3), bezoar/foreign object (n=3), intussusception (n=2), Crohn’s disease (n=1), stricture (n=1), and gallstone ileus (n=1). There were 18 cases in which more than one cause of obstruction was identified intraoperatively. The various combinations of causes of obstruction included adhesions + internal hernia (n=11), adhesions + volvulus (n=2), appendicitis + abscess (n=2), external hernia + carcinomatosis (n=1), volvulus + internal hernia (n=1), and adhesions + carcinomatosis (n=1). Fifty-five subjects (38.7%) had CT scan within 24 h of exploratory surgery, 55 subjects (38.7%) were scanned 24–48 h before surgery, and 32 subjects (22.5%) had CT scan 48–72 h before surgery.
The CT examinations were performed on multidetector row GE Lightspeed QX/i CT scanners (General Electric Medical Systems, Milwaukee, WI) in accordance with our abdomen and pelvis protocol. Patients were asked to ingest 900 ml of oral contrast (Readi-Cat 2 Barium Sulfate Suspension; E-Z-EM, Westbury, NY) in three split doses 120, 90, and 60 min prior to scanning. Enhanced axial CT images from the diaphragm to the symphysis pubis were obtained using 5-mm-thick sections and 5-mm intervals in high-speed (HS) mode (pitch 6:1), with rotation speed of 0.8, table speed of 15 mm/rotation, 120 kV, and 210 mA (190 mA was selected for thin patients and 230 mA for obese patients at the discretion of the technologist or radiologist). One hundred fifty milliliters of iopamidol (Isovue 370; Bracco Diagnostic, Princeton, NJ) was then injected intravenously at a rate of 2 ml/s with a mechanical power injector using 18- to 20-gauge catheters placed in an antecubital vein. Image acquisition started approximately 70 s after i.v. injection or by utilizing the SmartPrep technique (General Electric Medical Systems). Studies were viewed on a PACS monitor (General Electric Medical Systems) generally in the cine or stack mode scrolling through the images to evaluate the abdomen and pelvis. When available, coronal reconstructed images were also reviewed following the review of the axial images (99 patients, 70%).
Cases were reviewed by three board-certified radiologists specialized in abdominal imaging. All reviewers were blinded to clinical history and surgical diagnosis. Cases were reviewed jointly, making observations on a consensus basis. CT studies were analyzed for the presence of extraluminal bands, and attempts to identify the transition zone on both axial and coronal reconstructed images were made. An extraluminal band was considered present if there was an appearance of the transition zone suggestive of an extrinsic linear band resulting in extraluminal compression of the bowel. (Fig. 1).

A 52-year-old woman who had been complaining of abdominal pain radiating to the back and groin. At laparotomy, a closed-loop small-bowel obstruction due to an adhesion was found. Axial contrast-enhanced CT shows extraluminal compression of the bowel caused by an adhesion. The resultant appearance is suggestive of a linear band extending across the bowel in the plane indicated by the arrows
Computed tomography findings with respect to the presence of extraluminal bands were compared with the cause of SBO identified intraoperatively at exploratory surgery. The 95% confidence intervals (CI) were calculated for sensitivity, specificity, p value, and positive and negative predictive values of the extraluminal band as a sign for adhesive SBO.
Cases were reviewed by a fourth radiologist who specialized in abdominal imaging, also blinded to clinical history and surgical diagnosis, who made observations about whether the transition zone could be identified on the axial and coronal images in cases where the reformatted images were available.
Results
On CT in SBO, the presence of a transition point with the appearance suggestive of a band extending across and resulting in extraluminal compression of the bowel correlated well with a diagnosis of adhesive SBO. In this study, among the 85 patients with surgically proven SBO secondary to adhesions, an extraluminal band was noted on CT in the area of the transition zone in 52 cases (Table 1). This corresponds with a sensitivity of 61% (95% CI 0.51–0.71). The extraluminal band was absent in 36 of 57 cases of nonadhesive SBO, yielding a specificity of 63% (95% CI 0.50–0.75). Among the 73 cases in which the extraluminal band was identified on CT, the obstruction was proven to be secondary to adhesions at exploratory surgery in 52 cases, resulting in a positive predictive value of 71% (95% CI 0.60–0.80). The p value was 0.008. Negative predictive value was 52% (95% CI 0.41–0.64), but this was not statistically significant because the lower bound of the 95% confidence interval crossed 50%.
While the adhesive band itself is not visualized on CT in SBO, it results in a transition zone with distinct characteristics. Figure 1 demonstrates the characteristic, although not pathognomonic, appearance of extraluminal compression of the bowel in adhesive SBO. In some instances, the presence of adhesive bands may result in the compression of a loop of bowel at two separate points (Fig. 2). Extraluminal bands may also cause kinking or angulation of the bowel at the transition point. This finding further enhances one’s ability to identify the presence of a band (Fig. 3).

An extraluminal band in a 77-year-old woman with a history of colon cancer status post resection 2 years prior to admission, presenting with an adhesive small-bowel obstruction. Coronal contrast-enhanced CT demonstrates extraluminal compression of a loop of small bowel at two separate points (arrows); the appearance is suggestive of an extraluminal band extending across the bowel oriented in the plane indicated by the arrows

Extraluminal band in a 59-year-old woman with a history of ovarian cancer and other abdominal surgery presenting with small-bowel obstruction due to adhesions. a Axial contrast-enhanced CT demonstrates a kink in the bowel in the area of transition (arrow) with an appearance suggestive of an extraluminal band causing a linear impression on the bowel at this point. b Coronal reformatted image better illustrates the kinking and angulation resulting from the adhesive band
In this series, coronal reformatted images were available on the PACS in 99 cases (70%). Among the 99 cases in which coronal reformatted images were available, the transition zone could be identified on the coronal images in 61 patients (62%). In two cases, the transition zone was not successfully identified on axial images but was found on the coronal reformatted images.
While the presence of an extraluminal band in the area of the transition zone had a high positive predictive value for adhesive SBO, similar bands were identified in 21 false-positive cases (Fig. 4) . False positives were most often related to SBO secondary to neoplasm (n=9), internal hernia (n=5), and volvulus (n=3). Other causes included external hernia, foreign object, and gallstone ileus.

A 55-year-old woman with a history of ulcerative colitis who presented with nausea and vomiting. In this axial contrast-enhanced CT, there is the appearance of a linear impression on the bowel (arrows) suggestive of extraluminal compression of the bowel caused by an adhesive band extending across the bowel. However, at exploratory laparotomy, the patient was found to have a small-bowel obstruction secondary to a metastatic colon carcinoma and peritoneal carcinomatosis. History of malignancy was not known to the readers
A longer time interval between CT scan and exploratory surgery did not correlate with a higher proportion of false-positive cases. Among the 21 false-positive cases, 8 (38%) had the CT scan 0–24 h before surgery, 8 (38%) had the CT scan 24–48 h before surgery, and 5 (24%) had the CT scan 48–72 h before surgery.
The high number of false-positive cases related to malignancy prompted analysis of the usefulness of the sign in patients without a history of abdominal malignancy. Thirty-nine patients with a history of a malignancy arising in the abdomen, lymphoma, or malignancy that had metastasized to the abdomen were excluded, and the results were reevaluated (Table 2). Among the 14 cases in which malignancy was found to be the cause of obstruction at laparotomy, 11 were due to tumor, 2 were secondary to carcinomatosis, and in 1 case, both forms of neoplasm were present.
Among the 63 patients with adhesive SBO, the extraluminal band was identified on CT in 40, resulting in a sensitivity of 64% (95% CI 0.51–0.74). In the nonadhesive SBO group, 28 of 40 did not have an extraluminal band on CT, yielding a specificity of 70% (95% CI 0.55–0.82). The positive predictive value for the extraluminal band sign predicting obstruction was 77% (95% CI 0.64–0.86), and the negative predictive value was 55% (95% CI 0.41–0.68). The p value was 0.002. The negative predictive value was not statistically significant because the lower bound of the confidence interval crossed 50%.
Discussion
The diagnosis of SBO is based on clinical signs, patient history, and radiographic findings [5]. CT has assumed a central role in the diagnosis of SBO because of its ability to pinpoint the site, level, and cause of bowel obstruction as well as associated complications such as ischemic bowel and other intra-abdominal pathology [3–6]. CT also has a role in triaging cases for surgical compared with conservative management because it is more sensitive for signs of strangulation and volvulus—findings that necessitate urgent laparotomy—than clinical signs such as peritoneal irritation [14]. One failing of CT, however, has been its inability to reliably identify adhesions in adhesive SBO.
Uncertainty with the diagnosis of adhesions as the cause of SBO stems from the fact that adhesive bands are not typically seen on CT [3, 5, 7, 8] unless they are complicated by inflammation or carcinomatosis, where they may appear as linear bands of soft tissue [15]. Instead, the CT diagnosis of adhesions must be based on an abrupt change in bowel caliber without evidence of another cause of obstruction [5, 6, 16, 17]. This is a serious weakness because adhesions are the cause of 50–75% of all SBOs [10–12]. Thus, in the majority of cases, a presumptive diagnosis is being made that is based in large part on the high prevalence of SBO secondary to adhesions and the lack of another discernable cause. Basing the diagnosis of adhesive SBO entirely on the absence of an obvious cause is problematic because other conditions with subtle radiographic appearances can be misrepresented as adhesions.
The transition zone is the natural place to look for clues to the etiology of SBO. Some researchers such as Herlinger and Ha et al. have suggested that there may be a characteristic appearance of the transition zone in adhesive SBO [18, 19]. Ha et al. further determined that the appearance of the transition zone could be used to differentiate strangulated from nonstrangulated bowel [19]. It is reasonable to expect that the presence of an obstructing adhesive band would have a pronounced effect on the appearance of the transition zone. In fact, Welch noted that a single obstructive band is usually fibrous and constrictive, and generally prone to high-grade obstruction [20]. Because at least 50% of patients with SBO due to adhesions are ultimately found to have a single obstructive band [21], one would expect the transition zone in the majority of adhesive SBOs to reflect the extraluminal compression of the bowel that would be produced by a linear adhesive band.
While several researchers have commented on the appearance of the transition zone in SBO, to our knowledge, none has examined the utility of the appearance of the transition zone alone in the diagnosis of adhesive SBO. This study, through a retrospective review of CTs of a relatively large number of patients with SBO, evaluated the usefulness of a sign the authors termed the extraluminal band in the diagnosis of adhesive SBO. The extraluminal band refers to a change in the conformation of the transition zone that would be seen as a result of extraluminal compression by a single obstructive adhesive band (i.e., linear impression on the bowel; Fig. 3a).
In this study, identification of an extraluminal band sign on CT in cases of SBO correlated highly with a diagnosis of adhesive SBO. The appearance of a linear impression on the bowel in the area of the transition zone had a positive predictive value of 71% for SBO secondary to adhesions. With a moderately high positive predictive value, the extraluminal band may be a helpful diagnostic adjunct, but by itself, it is clearly not diagnostic of adhesive SBO.
However, in this study, reviewers were blinded to clinical history, which can often aid in the identification of the cause of obstruction. Menzies and Ellis noted that patients who have undergone laparotomy at least once are found to have adhesions at subsequent surgery in over 90% of cases [22]. Moreover, 80% of adhesions occur after surgery [12]. Thus, a clinical history of abdominal surgery obviously raises the radiologist’s suspicion for adhesive SBO. When combined with this history, the positive predictive value of the extraluminal band might have been higher. It would have been interesting to test this hypothesis or even the positive predictive value of a history of previous abdominal surgery alone for adhesive SBO. However, this information was not available in the medical record in every case, so an analysis was not attempted.
It is also interesting to note that neoplasm emerged as the predominant cause of false-positive diagnosis in this study. These were likely extrinsic lesions because most intrinsic bowel lesions causing obstruction manifest with mural thickening at the transition zone [16]. Obstructing malignancies extrinsic to the small bowel typically produce rounded outline deformities on the bowel [18] rather than an acute angulation of the bowel wall expected of a single adhesive band. However, it is possible that these extrinsic neoplasms produce an appearance similar to an extraluminal band when viewed in only one plane. Another possible confounder is that neoplasms may be associated with desmoplastic reactions [5, 15, 18], simulating the appearance caused by a single adhesive band.
When reexamining the data and applying the extraluminal band sign exclusively in cases without a history of intra-abdominal malignancy, the positive predictive value rose to 77% (Table 2). Thus, had the reviewers been aware of a clinical history of malignancy, the false-positive rate might have been significantly lower secondary to a higher index of suspicion for a nonadhesive etiology of obstruction.
Internal hernia was also a prominent cause of false-positive diagnosis in this study. It is possible that these cases occurred in situations where there was a narrow opening in the mesentery and an acute change in the direction of the bowel near the point of impingement and obstruction; the resultant kinking and acute angulation could simulate an extraluminal band.
Coronal reformatted images proved quite helpful in identifying the transition zone. The fact that the transition zone was identified in 62% of cases in which the reformatted images were available highlights the opportunities for examining the transition zone from multiple perspectives. As noted by Caoili and Paulson, multiplanar reformatted images afford the prospect of better characterization of the transition zone [15]. Figure 3 illustrated how the extraluminal band may be more prominent on the coronal reformatted image than on the image in the axial plane. At a minimum, multiplanar reformatted images offer the opportunity to confirm findings seen on axial images such as the location of the transition zone. Yet, the two cases in this study in which the transition zone could only be identified on the coronal reformatted images underscore the opportunity to complement the findings of images in the axial plane.
The study was limited by its retrospective nature. Under ideal conditions, exploratory surgery would have been done within just a few hours of the CT scan in all cases to ensure that CT findings correlate precisely with intraoperative findings. Additionally, the investigators had to rely on surgical operative reports for the intraoperative findings and what the surgeons considered to be the cause of obstruction in each case. In five cases, surgical operative reports were not clear about the cause of obstruction. These cases were excluded from the study. In the 14 cases where adhesions and another cause of obstruction were identified in the surgical report, adhesions were counted as the primary cause of SBO.
While a prospective study would have been ideal, our study sample is more representative of those situations in which the application of the extraluminal band sign would be most useful. This patient sample likely represents those patients in whom the etiology of SBO was most unclear from a clinical standpoint and in whom imaging could be obtained. Those patients whose condition was most severe, as in the case of an incarcerated or strangulated bowel, were likely taken to the operating room before imaging could be performed. Therefore, this sample represents those patients most likely to undergo imaging in a real-life scenario.
Another limitation of the study was related to the fact that imaging findings were decided by consensus among the three readers. There was no assessment of intra- or interobserver variability. Also of note is that while the positive predictive value for the extraluminal band is statistically significant, the prevalence of adhesions in this population was high (60%), and this obviously contributed to the high positive predictive value that was attained in the study.
Despite these limitations, the authors of this study believe the extraluminal band can serve as a helpful diagnostic adjunct for adhesive SBO. The study demonstrated that the appearance suggestive of an extraluminal band on CT in patients with SBO is associated with a high predictive value for an underlying adhesion causing the obstruction. The increase of the positive predictive value from 71 to 77% when excluding all patients with a history of intra-abdominal malignancy leads us to believe that this could be a more powerful test when applied in select cases, although more research is needed on this topic. In the absence of an obvious cause of SBO, the presence of an extraluminal band can increase the radiologist’s confidence in a diagnosis of adhesive SBO.
References
Suh RS, Maglinte DDT, Lavonas EJ et al (1995) Emergency abdominal radiography: discrepancies of preliminary and final interpretation and management relevance. Emerg Radiol 2:1–4
McFadden DW, Zinner MJ (1994) Manifestations of gastrointestinal disease. In: Schwartz SI, Shires GT, Spencer FC (eds) Principles of surgery. McGraw-Hill, New York, pp 1015–1042
Megibow AJ, Balthazar EJ, Cho KC et al (1991) Bowel obstruction: evaluation with CT. Radiology 180:313–318
Fukuya T, Hawes DR, Lu CC et al (1992) CT diagnosis of small-bowel obstruction: efficacy in 60 patients. AJR Am J Roentgenol 158:765–769
Furukawa A, Yamasaki M, Furuichi K et al (2001) Helical CT in the diagnosis of small bowel obstruction. Radiographics 21:341–355
Maglinte DT, Reyes BL, Harmon BH et al (1996) Reliability and role of plain film radiography and CT in the diagnosis of small-bowel obstruction. AJR Am J Roentgenol 167:1451–1455
Frager DH, Baer JW (1995) Role of CT in evaluating patients with small-bowel obstruction. Semin Ultrasound CT MR 16:127–140
Hulnick DH (1986) Small intestine. In: Balthazar EJ, Megibow AJ (eds) Computed tomography of the gastrointestinal tract. Mosby, St. Louis, p 273
Balthazar EJ (1994) George W. Holms Lecture. CT of small-bowel obstruction. AJR Am J Roentgenol 162:255–261
Bizer LS, Liebling RW, Delany HM et al (1981) Small bowel obstruction: the role of non-operative treatment in simple intestinal obstruction and predictive criteria for strangulation obstruction. Surgery 89:407–413
Livingstone AS, Sosa JL (1995) Ileus and obstruction. In: Haubrich WS, Schauffnewer F, Berk JE (eds) Bockus gastroenterology, 5th edn. Saunders, Philadelphia, pp 1235–1248
Herlinger H, Maglinte DDT (1989) Small bowel obstruction. In: Herlinger H, Maglinte DDT (eds) Clinical radiology of the small intestine. Saunders, Philadelphia pp 479–507
Moses BV (2000) Surgical conditions of the small intestine. In: Ratnaike, R (ed) Small bowel disorders. Arnold, London, pp 472–481
Donckier V, Closset J, Van Gansbeke D et al (1998) Contribution of computed tomography to decision making in the management of adhesive small bowel obstruction. Br J Surg 85:1071–1074
Caoili EM, Paulson EK (2000) CT of small bowel obstruction: another perspective using multi-planar reformations. AJR Am J Roentgenol 174:993–998
Boudiaf M, Soyer P, Terem C et al (2001) CT evaluation of small bowel obstruction. Radiographics 21:613–624
Maglinte DT, Gage SN, Harmon BH et al (1993) Obstruction of the small intestine: accuracy and role of CT in diagnosis. Radiology 188:61–64
Herlinger H (1997) Radiology evaluation of small bowel obstruction. RSNA categorical course in diagnostic radiology. Gastrointestinal 49–58
Ha HK, Park CH, Kim SK et al (1993) CT analysis of intestinal obstruction due to adhesions: early detection of strangulation. J Comput Assist Tomogr 17:386–389
Welch JP (1990) Adhesions. In: Welch JP (ed) Bowel obstruction: differential diagnosis and clinical management. Saunders, Philadelphia, pp 154–165
Suter M, Zermatten P, Halkic N et al (2000) Laparoscopic management of mechanical small bowel obstruction. Surg Endosc 14:478–483
Menzies D, Ellis H (1989) Intra-abdominal adhesions and their prevention by topical tissue plasminogen activator. J R Soc Med 82:534–535
Author information
Authors and Affiliations
Corresponding author
Additional information
An editorial comment on this paper is available at http://dx.doi.org/10.1007/s10140-005-0451-3.
Rights and permissions
About this article
Cite this article
Petrovic, B., Nikolaidis, P., Hammond, N.A. et al. Identification of adhesions on CT in small-bowel obstruction. Emerg Radiol 12, 88–93 (2006). https://doi.org/10.1007/s10140-005-0450-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-005-0450-z