
Abstract
The purpose of this study was to evaluate the diagnostic equivalence, radiation dose, clinical usefulness and radiographic aspects of a low-dose, full-body digital X-ray machine in a busy trauma unit. A digital trauma X-ray machine known as "LODOX" was compared with conventional radiography between June 1999 and November 2001 in the Groote Schuur Hospital Trauma Unit, Cape Town. Digital images of a variety of body regions commonly imaged in trauma were compared for diagnostic image quality in a number of categories with equivalent conventional radiographs. A seven-point equivalence scoring system ranging from much inferior (−3) through equivalent (0) to much superior (+3) was used in each category. Radiation dose was recorded and compared with that in conventional measurements. Turnaround times of patients undergoing digital and conventional X-rays were evaluated. Clinical and radiographic issues were assessed by staff feedback. The digital images when compared with conventional film had an overall mean equivalence score of −0.429, with a standard deviation (SD) of 0.77. The best digital performance was in the mediastinum (mean 0.346, SD 0.49) and the weakest was for bony detail (mean −0.654, SD 0.81). Relative digital radiation dose compared to conventional varied from 72% (chest) to 2% (pelvis), with a simple average of 6%. Radiographic points included full-body imaging capability and differing positioning, penetration, workflow and practicality considerations. The digital images required overall patient times of 5–6 min, compared with 8–48 min for conventional X-rays. New installations are under way, and computed tomography and angiography applications are being explored. FDA approval is awaited. Projected cost is similar to that of flat-panel digital units. This digital unit was felt to be diagnostically substantially equivalent to conventional radiographs, with low-dose full-body imaging, improved workflow, digital technology and long-term cost benefits as potentially favourable contributions to trauma imaging.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Despite the escalating role of computed tomography (CT) in trauma, radiography remains important in the acute management of many trauma patients. Ideally, X-ray imaging should permit comprehensive radiographic evaluation of all injured areas. However, to save time and expedite triage the chest, pelvis and lateral cervical spine are often the only areas X-rayed immediately. Inherent delays, relatively high radiation dose and practical difficulties in acquiring radiographs in the multi-injured patient can adversely affect management, bearing in mind the critical importance of physician access to badly injured patients during the "golden hour". Despite many benefits, digital radiography has not yet replaced conventional X-ray film in most trauma units.
The purpose of this study was to compare the diagnostic performance, radiation dose and clinical utility of a new type of trauma-oriented, full-body digital X-ray machine with reference to conventional radiography in a busy trauma unit. This digital unit purports to offer workflow advantages that may add value to trauma management, including the ability to rapidly acquire frontal or lateral images of any or all regions at low dose. Other potential applications including CT and angiographic options were also evaluated.
Materials and methods
This digital radiography device was initially locally developed as a very-low-dose unit for the detection of smuggled diamonds, based on an X-ray security scanner. It was subsequently felt to be suitable for medical use. Following clinical testing of an earlier prototype [1], a thoroughly redesigned trauma-specific unit was manufactured for further clinical testing (Fig. 1). The present trial was conducted in the Trauma Unit of Groote Schuur Hospital, Cape Town, during the period 1 June 1999 to 30 November 2001. The current device was named "LODOX" (derived from "low-dose X-rays"), in reference to the low radiation dose used to obtain images.

Digital X-ray unit demonstrating X-ray tube and detector arm mounted on C-arm. Direction of travel is indicated
The machine makes use of an X-ray tube mounted on one end of a C-arm (Fig. 1). This emits a low-dose collimated fan-beam of X-rays. Fixed to the other end of the C-arm is the X-ray detector unit, comprising scintillator arrays optically linked to charge-coupled devices (CCDs). The detectors have a 60-μm size, and are generally used in combination, providing up to 5,800 elements along the length of the detector arm. Variations of spatial resolution from 1.6 to 4.1 line-pairs per millimetre are possible. They are able to record 14 bits of contrast resolution. The C-arm is able to rotate axially around the patient to any angle up to 90°, permitting horizontal-beam, shoot-through lateral, erect and oblique views. This rotation has been increased to 100° in a later prototype. The C-arm travels along the table length at speeds of up to 138 mm/s when emitting radiation. This device is able to rapidly acquire images of part or all of the body; a full body scan requires 13 s, with smaller areas requiring proportionately less time.
A special integral docking table was designed to receive incoming patients to eliminate the need to transfer the injured patient to another stretcher, also permitting easier transport, scanning and patient access. The ability to lift or depress either end of the table allows some compound oblique views. A computer-controlled operating and viewing system with standard DICOM 3 (Digital Imaging and Communication in Medicine 3) output is included.
After obtaining institutional review board permission, images obtained on the digital device were judged for diagnostic performance against conventional radiography of the same regions, where possible using the same subjects (Figs. 2, 3, 4, 5, 6; Tables 1, 2). Two experienced trauma radiologists used a seven-point comparative scale derived from Huda et al. [2], with ratings ranging from much inferior (−3), through equivalent (0) to much superior (+3). Digital images were displayed on a high-luminance medical-quality monitor and compared with the equivalent conventional radiographs placed on a viewing box alongside.

Comparative chest images obtained with (a) conventional system and (b) digital X-ray unit

Example of full-body digital X-ray of patient with multiple injuries

Example of flying-angel view of the cervicothoracic junction obtained on the digital unit

High-resolution digital view of the wrist demonstrating good trabecular detail

Means and standard deviations of diagnostic equivalence scores in the categories evaluated. Mean, block; standard deviation, bar
A medical physicist measured radiation doses for corresponding procedures on the digital unit and on a predicate conventional system (Siemens Polydoros) using standard dosimeters.
Details of the perceived clinical utility of the digital device and any radiographic and technical issues encountered were obtained from trauma unit medical staff and radiographers.
Results
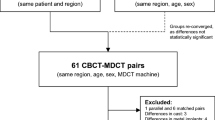
The relative individual and overall diagnostic equivalence scores in the various categories are given in Table 2 and Fig. 6. A separate overall judgement of acceptability was made, which was in the affirmative for all digital images. A total of 26 patients underwent both digital and conventional imaging, while for 13 patients digital images were compared with equivalent conventional images of other patients. Radiation dose measurements for conventional and digital techniques are given by radiographic region in Table 3 and Fig. 7. Clinical imaging times are summarised in Fig. 8 [3].

Mean radiation doses for conventional and digital radiographs, by category

Comparative imaging times (in minutes at top of columns) in patient groups using LODOX digital and conventional X-rays. Patient numbers are given in parentheses. Reproduced from [3] with permission
Positive user feedback was obtained on overall ease of use, full-body view capability, local motion tolerance, patient accessibility and workflow benefits. Unfavourable comments were made concerning the physical bulk of the unit, penetration in some thick body regions, unfamiliar radiographic positioning requirements and intermittent reliability issues.
Discussion
In spite of a number of reports on the use of digital radiography in trauma, this form of imaging has not yet become dominant for a variety of reasons, many of them technological and financial [4]. An early attempt at use of a somewhat similar low-dose trauma digital machine was compromised by low resolution, limited viewing options and lack of hard copy [5]. Other fan-beam, slot-scanning or similar X-ray digital devices have been reported [5, 6, 7, 8, 9, 10, 11]. The use of a digital image intensifier in a trauma center has also been described [12]. Competing digital radiography technologies in trauma-related areas include computed radiography (CR) [8, 13, 14, 15], which has the benefit of a long-standing presence in the radiology sector. Flat-panel detectors [2, 16] have yet to make a major impact on day-to-day radiology or trauma. In addition, requirements for skeletal digital radiography [14, 17, 18, 19, 20, 21] differ from those of general radiography [22]. Analogue X-rays remain a strong gold standard.
The dedicated trauma digital X-ray device described in this article appears to offer some advantages, including good quality images, low dose, ease of use and the ability to obtain full-body views. The image quality was regarded as substantially equivalent to that of conventional X-rays in all categories. Although the scores in certain categories were slightly less than those for conventional film, this deviation was not felt to be significant, and the digital device exceeded the standard in other categories. The mean combined score was −0.429, with a standard deviation of 0.77. In mediastinal, lung and soft tissue categories, the digital images were judged superior. For bone detail, bone contrast, spine, rib, spatial resolution, contrast resolution and image mottle, the digital images fared slightly less well than conventional images. Even so, important high-detail features such as lung fissures, pneumothoraces and fractures were readily detected. Mediastinal structures and soft tissue contrasts were confidently seen. With the C-arm rotated to 90°, horizontal-beam lateral shoot-throughs or decubitus views on injured or immobile patients were possible. In projections through thick parts of the body, such as the lateral cervicothoracic (Fig. 4) and lateral lumbar views, it was difficult to consistently obtain images with good trabecular detail, although bony alignments were visible. This was improved by upgrading the X-ray tube.
The digital radiation dose measurements were always less than those for conventional radiography, with the smallest discrepancy in the chest (where digital images required 72% of conventional dose) and the most marked for pelvic images (where digital imaging required 1.6% of conventional dose). By simple averaging, the mean conventional dose was 0.573 R (5.73 mGy), while the mean digital dose was 0.033 R (0.33 mGy), 5.9% of conventional. The lower doses have long-term staff and population consequences, particularly when regulatory and public pressures come to the fore. The overall impression was that the diagnostic outcome on this machine was substantially equivalent to that of regular X-rays, despite the lower dose (Table 3, Fig. 7). Other digital radiography devices have also reported dose reduction benefits [5, 7, 9, 10, 14, 23, 24, 25, 26], although performance has not always been equivalent to that of conventional radiography [5, 10, 26, 27].
Trauma medical staff viewed favourably the 13-s full-body scan time and the low overall interference with resuscitation. The digital device required a total of 5–6 min of patient time to produce images, compared with between 8 and 48 min for conventional X-rays (Fig. 8). This difference was most marked in the resuscitation category, where an average of 6 min for the digital unit compared well with the 48 min for the conventional system. In addition, patient accessibility was felt to be better on the digital unit.
Images of small localised areas, up to the entire patient, were possible. Good-quality images of a number of regions could be obtained by zooming in on a single full-body acquisition. This permitted rapid evaluation of the entire patient, quickly identifying injuries and expediting continuing management. As far as is known, full-body images at this level of detail are not available on other devices. The full-body feature was of particular value in detecting bullets in the body, especially in unexpected locations. The closest analogous means of acquiring full-body images is the "scannogram" or "scout view" used for CT scanning [25], although at lower resolution. The option of repeating specific views at higher resolution increased the functionality of the unit. The versatility and ease of operation in allowing frontal, oblique, lateral or horizontal projections was favourably commented on. Oblique X-rays could be obtained by a combination of patient positioning and rotating the C-arm. Slight geometric distortion due to beam divergence was noted on some lateral views, but could be simply corrected by software.
At a practical level, the radiographic positioning requirements for this device were different from those of regular X-ray units. It was sometimes difficult to ensure optimal positioning of the body for the most favourable radiography of multiple areas, especially when obtaining full-body views. For example, combining frontal skull, cervical spine, humeri, chest, pelvis and leg views required all these parts to be radiographically well positioned. In some cases, compromise positioning was necessary, especially with restless patients. Motion tolerance was particularly notable, with slight or moderate patient movement only producing a rubbery deformity of the region concerned [6, 28].
The rapid availability of images for interpretation because of their digital nature and the reduced need for repeat exposures because of faulty radiography were also felt to be strengths. Standard DICOM-compatible output was provided, allowing access to other advantages of digital imaging, including seamless distribution and viewing on a variety of computer platforms [29].
Perceived limitations include the physical bulk of the device and the reliability of the prototype. User feedback on hardware and software errors was noted, with failed exposures and operational interruptions reported as intermittent problems. Rigorous re-engineering and further extensive debugging of the hardware and software of the unit are aimed at addressing these.
The overall cost of this trauma digital unit is projected to be competitive with that of flat-plate digital detector systems. As with other digital radiography devices, the high initial capital cost of the unit stands to be offset by lower consumable costs. A sophisticated support service would be required to maintain the unit, although its construction is in many areas based on industry-standard devices and software.
New units are being built for further development work and clinical testing in trauma units elsewhere.
Additional potential applications include use as a general-purpose digital radiography unit. This would be especially but not exclusively suited to skeletal surveys. It also has potential as a chest-screening device, such as for pulmonary tuberculosis. Erect chest radiographs of multiple side-by-side patients would be feasible during one traverse of the laterally rotated C-arm. A related system of computer-aided detection for miliary tuberculosis is also being developed.
The speed of travel of the C-arm is thought to be very suitable to acquiring digital angiography of the entire lower extremity. This could be unsubtracted or subtracted. The ability to perform angiography is due to be tested formally, and may have a specific role in trauma. This does assume that the angiography catheter is already placed, or that allowance is made for a means of fluoroscopic monitoring, such as a mobile C-arm, during the placement of the angiographic catheter. A form of visual feedback and adjustable scan-speed during the bolus injection would add value. Another potential subtraction application concerns the use of dual energy subtraction (DES).
The increasingly important role of spiral CT in trauma imaging has the one disadvantage of a significantly higher radiation dose. The full benefits of multi-slice and "whole-body" CT on trauma have yet to be clarified. The strengths of the digital X-ray device under investigation in this report include its full-body capability, versatility and low radiation dose, but the purely two-dimensional presentation of the image remains a major shortfall compared to CT. A unit has therefore been deployed to allow research and development into possible acquisition of CT images, specifically aimed at achieving limited-angle computed tomography (LACT). This would be achieved by acquiring a number of images with the C-arm at different radial angles. At present reasonable images are possible by combining acquisitions from reversed table positions, but the challenge is to allow this to be more rapidly and easily performed (Fig. 9). The intended limited-angle technique of acquisition does mean that this method would be unlikely to compete for speed with fast spiral CT scanners.

Computer tomographic scan of head phantom obtained by combining two 90° acquisitions. (With acknowledgements to Mattieu de Villiers)
Commercialisation of the unit is anticipated, and distribution and support infrastructures are being developed. A submission to the USA Food and Drug Administration for 510 k approval was made at the end of 2001.
Conclusions
The substantially equivalent diagnostic performance and overall functionality of this low-dose digital X-ray unit have both clinical and radiographic promise. Easy digital imaging of any region up to a full-body view can be achieved with minimal interruption in the patient's management. The unit appears well suited to the trauma milieu and may offer a new paradigm of efficient radiographic evaluation in patient management. This contribution is presently undergoing further assessment, as are additional studies of the relevance of alternative planned specific features.
References
Beningfield SJ, Potgieter JH, Bautz P, Shackleton M, Hering E, de Jager G, Bowie G, Marshall M, Cox G, Pagliari G, Coetzee N (1999) Evaluation of a new type of direct digital radiography machine. S Afr Med J 89:1182–1188
Huda W, Scalzetti EM, Geiger R, Roskopf ML (2001) Clinical performance of a commercial prototype flat-panel digital detector for general radiography. Medical Imaging, The International Society for Optical Engineering, San Diego, 17–23 February 2001
van As AB, Beningfield SJ, Vaughan CL, Potgieter JH (2000) Trauma assessment in the third millennium; the LODOX imaging device. 4th European Congress, Trauma & Emergency Surgery, European Association of Trauma and Emergency Surgery, Pisa, 16–20 April 2000
Gray JE, Karsell PR, Becker GP, Gehring DG (1984) Total digital radiology: is it feasible? Or desirable? Am J Roentgenol 143:1345–1349
Curtis DJ, Ayella RJ, Whitley J, Moser RP, Rugh KS (1979) Digital radiology in trauma using small-dose exposure. Radiology 132:587–591
Tesic MM, Sones RA, Morgan DR (1984) Single-slit digital radiography: some practical considerations. Am J Roentgenol 142:697–702
Slasky BS, Sashin D, Horton JA, Sternglass EJ, Bron KM, Deutsch M, Herron JM, Kennedy WH, Boyer JW, Girdany BR, Skinner SR, Simpson RW, Hoy RJ, Feist JH (1987) Digital radiography of the chest by self-scanning linear diode arrays. Acta Radiol 28:461–466
Smathers RL, Brody WR (1985) Digital radiography: current and future trends. Br J Radiol 58:285–307
Kushner DC, Cleveland RH, Herman TE, Zaleske DJ, Ehrlich MG, Correia JA (1986) Radiation dose reduction in the evaluation of scoliosis: an application of digital radiography. Radiology 161:175–181
Kushner DC, Cleveland RH, Herman TE, McLoud TC, Waltman AC, Shepard JA, Dedrick CG, Kopans DB, Greene RE (1987) Low-dose flying spot digital radiography of the chest: sensitivity studies. Radiology 163:685–688
Sones RA, Lauro KL, Cattell CL (1990) A detector for scanned projection radiography. Radiology 175:553–559
Vandemark RM, Fay ME, Porter FR, Johnson GA (1997) Digital image-intensifier radiography at a level I trauma center. Am J Roentgenol 168:944–946
Elam EA, Rehm K, Hillman BJ, Maloney K, Fajardo LL, McNeill K (1992) Efficacy of digital radiography for the detection of pneumothorax: comparison with conventional chest radiography. Am J Roentgenol 158:509–514
Murphey MD, Quale JL, Martin NL, Bramble JM, Cook LT, Dwyer SJ (1992) Computed radiography in musculoskeletal imaging: state of the art. Am J Roentgenol 158:19–27
Saito H, Kurashina T, Ishibashi T, Shimanuki Y, Sakamoto K (1988) Digital radiography in an intensive care unit. Clin Radiol 39:127–130
Strotzer M, Gmeinwieser J, Volk M, Frund R, Seitz J, Manke C, Albrich H, Feuerbach S (1998) Clinical application of a flat-panel X-ray detector based on amorphous silicon technology: image quality and potential for radiation dose reduction in skeletal radiography. Am J Roentgenol 171:23–27
Murphey MD (1989) Digital skeletal radiography: spatial resolution requirements for detection of subperiosteal resorption. Am J Roentgenol 152:541–546
Bramble JM, Murphey MD (1990) Comparison of digital and conventional musculoskeletal radiography: observer performance study. Radiology 177:587–589
Wilson AJ (1995) Filmless musculoskeletal radiology: why is it taking so long? Am J Roentgenol 165:105–107
Buckwalter KA, Braunstein EM (1992) Digital skeletal radiography. Am J Roentgenol 158:1071–1080
Wilson AJ, Hodge JC (1995) Digitized radiographs in skeletal trauma; a performance comparison between a digital workstation and the original film images. Radiology 196:565–568
Seeley GW, Fisher HD, Stempski MO, Borgstrom M, Bjelland J, Capp MP (1987) Total digital radiology department: spatial resolution requirements. Am J Roentgenol 148:421–426
Templeton AW, Dwyer SJ, Cox GG, Lee KR, Johnson JA, Martin NL, Chang CH, Anderson WH, Hensley KS, Bialek J (1987) A digital radiology imaging system: description and clinical evaluation. Am J Roentgenol 149:847–851
Kogutt MS, Jones JP, Perkins DD (1988) Low-dose digital computed radiography in pediatric chest imaging. Am J Roentgenol 151:775–779
Aitken AG, Flodmark O, Newman DE, Kilcoyne RF, Shuman WP, Mack LA (1985) Leg length determination by CT digital radiography. Am J Roentgenol 144:613–615
Marshall NW, Faulkner K, Busch HP, Marsh DM, Pfenning H (1994) An investigation into the radiation dose associated with different imaging systems for chest radiology. Br J Radiol 67:353–359
Fajardo LL, Hillman BJ, Pond GD, Carmody RF, Johnson JE, Ferrell WR (1989) Detection of pneumothorax: comparison of digital and conventional chest imaging. Am J Roentgenol 152:475–480
Brody AS, Saks BJ, Field DR, Skinner SR, Capra RE (1986) Artifacts seen during CT pelvimetry: implications for digital systems with scanning beams. Radiology 160:269–271
Wade FA, Oliver CW, McBride K (2000) Digital imaging in trauma and orthopaedic surgery: is it worth it? J Bone Joint Surg [Br] 82-B: 791–794
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure statement:This presentation was made possible by a full grant from LODOX (Pty) Ltd.
FDA 510(K) approval granted August 2002
Rights and permissions
About this article
Cite this article
Beningfield, S., Potgieter, H., Nicol, A. et al. Report on a new type of trauma full-body digital X-ray machine. Emergency Radiology 10, 23–29 (2003). https://doi.org/10.1007/s10140-003-0271-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-003-0271-x