
Abstract
Some lasers have demonstrated to provide effective disinfection when used as adjunctive device to the conventional treatment. The aim of this in vitro study was to determine the effectiveness of the erbium, chromium:yttrium scandium gallium garnet (Er, Cr:YSGG) laser by measuring its bactericidal effect inside the root canal experimentally colonized with Enterococcus faecalis. The laser was tested at different irradiation times (30 and 60 s) and energy of impulses (75 and 25 mJ). A total of 52 single-rooted extracted human teeth were endodontically prepared with rotary instrumentation. All were sterilized and inoculated with a suspension of E. faecalis (105 bacteria/ml). The teeth were randomized into three treatment (group 1, group 2, and group 3) and one control groups. In all groups, teeth were chemically irrigated with 5.25 % sodium hypochlorite and 17 % ethylenediaminetetraacetic acid. Groups 1 and 2 were also irradiated at 30 and 60 s, respectively, with an Er, Cr:YSGG laser at 75 mJ. Teeth of group 3 were treated with laser for 60 s at 25 mJ. Samples were processed to detect the presence of E. faecalis. For all groups, a bactericidal effect was observed. The use of laser at 75 mJ with an irradiation time of 30 and 60 s eliminated a percentage of 92.3 and 100 % of E. faecalis, respectively. In the control group, a reduction of 92.3 % was observed. Lower percentage of reduction (46.1 %) was obtained in teeth treated with laser at 25 mJ for 60 s. No statistical differences were observed between the groups (P = 0.543, Fisher’s exact test). The results indicated a bactericidal effect of Er, Cr:YSGG laser irradiation at the settings used in this study. The highest bactericidal effect of this laser was observed at 60 s of irradiation time, using an energy pulse of 75 mJ.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The success of endodontic treatment depends on the effective elimination of microorganisms from the root canal. Approximately 50 microbiota have been quoted as being involved in root canal infections, but anaerobic bacteria play a key role in infectious conditions of the root canal [1]. Enterococcus faecalis (E. faecalis) has been shown to be the most commonly encountered bacterium in posttreatment dental infections as it is characterized by a marked persistence despite effective chemo-mechanical procedures. Indeed, the biological properties of this species allow the bacterium to survive in the adverse conditions within the canal, where concentrations of nutrients are low and alkaline conditions are prevalent. It has been reported that the bacterium could be isolated from one third of root canals after unsuccessful endodontic treatment [2–5].
The eradication of microorganisms from infected root canals is a complicated issue [6]. Several procedures have been described by which to disinfect root canals, including the use of numerous mechanical techniques, combined with different irrigation regimens and intra-canal medicaments. As bactericidal potential is developed through direct cell contact, chemical disinfections have to spread into the system in order to be effective. It has been demonstrated that sodium hypochlorite (NaOCl) is of limited use in penetrating and disinfecting dentinal tubules, and its efficacy is susceptible to temperature, concentration, and exposure time. Ethylenediaminetetraacetic acid (EDTA) is more effective in penetrating dentinal tubules than NaOCl, but no total disinfection has been demonstrated. The use of chlorexidine in disinfecting root canals was introduced as a final rinse, but it has weak penetrative power [7–11]. The relative importance of deep dentine infections for the prognosis of treatment is not yet known, but all infected habitats within the system may well represent important reservoirs, from which root canal infection may reoccur after treatment [12].
Recently, new antimicrobial approaches to improving the disinfection of root canals have been suggested, and one of these includes the use of lasers. Laser light is thought to be able to reach areas which are inaccessible with conventional techniques (e.g., bacteria deeply located in the fins, lateral canals isthmuses, and dentinal tubules). Given the characteristics of laser light (i.e., monochromatic, coherent, and directional) and the fact that direct contact between the target and fiber tip is not required, the use of laser (in addition to traditional procedures) could point the way to disinfecting areas which are difficult to access. Various laser systems have demonstrated their disinfecting capability when used in addition to conventional treatment [13, 14]. For example, the erbium, chromium:yttrium scandium gallium garnet (Er, Cr:YSGG) laser has been approved by the FDA for the cleaning of root canals [15]. Little is known about the effectiveness of the Er, Cr:YSGG laser in eliminating bacteria which may infect root canals, and the results of studies on this field are somewhat conflicting. Moreover, few studies have investigated the correlation between the irradiation time and the effectiveness of bactericidal action. Finally, the effectiveness of the Er, Cr:YSGG laser set at low impulse energy has not been extensively researched.
The aim of this in vitro study was to determine the effectiveness of the Er, Cr:YSGG laser by measuring its bactericidal effect inside root canals which had been experimentally colonized with E. faecalis. We also tested its antimicrobial effect for different irradiation times (30 and 60 s), and the effectiveness of the Er, Cr:YSGG laser was evaluated using different impulse energies in order to assess its disinfecting capability in the absence of any thermal potential.
Material and methods
Specimens
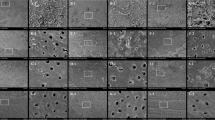
Seventy human teeth were obtained from patients affected by dental caries or severe periodontal disease. Those having one root and single canal were selected, whereas those having curved roots or any other abnormal shape were discarded. Those roots having more than one canal were also discarded, leaving a total of 52 human teeth which were used in the study. The teeth were carefully cleaned with a curette to completely remove soft tissues and adherent materials; they were then stored in a phosphate buffer until required. The root was separated from the rest of the tooth with the use of a diamond bur, and the root canal depth was measured with a K-file no.10. Selected roots were cleaned with a simultaneous technique deploying Ni-Ti files with a 30.06 gauging final apical preparation, using an Mtwo file system (VDW GmbH, Munich, Germany) [16]. The whole operation was mechanically performed under continuous irrigation with sodium hypochloride 5.25 % and EDTA 17 %. The specimens were finally rinsed with NaCl for 30 s, and the canals were closed in their apical region by means of bonding to prevent bacterial leakage (Fig. 1).

View of some specimens obtained after the mechanical procedures
Experimental procedures
The specimens were placed into test tubes and sterilized by autoclaving (121 °C for 20 min). Thereafter, the specimens were dried and placed in a sterile box at 37 °C for 24 h. A pure culture of E. faecalis, grown in a brain–heart infusion broth (BHI) (Difco, Detroit, MI, USA) was used to contaminate the root canals. The broth culture was obtained by incubating E. faecalis at 37 °C for 24 h. After checking for turbidity (using a McFarland standard and a quantitative determination by serial dilutions), an aliquot of 10 μl of the E. faecalis broth culture at a density of about 105 CFU/ml was inoculated into each root canal using sterile 1-ml tuberculin syringes.
After contamination, the specimens were incubated at 37 °C for 24 h, according to previously described protocols [17–19]; they were then divided into four groups (13 specimens each) following a simple randomization and treated according to the following protocols:
-
Group 1:
laser irradiation, 30 s cycle in 17 % EDTA and 5.25 % NaOCl (E = 75 mJ);
-
Group 2:
laser irradiation, 60 s cycle in 17 % EDTA and 5.25 % NaOCl (E = 75 mJ);
-
Group 3:
laser irradiation, 60 s cycle in 17 % EDTA and 5.25 % NaOCl (E = 25 mJ);
-
Group 4:
17 % EDTA and 5.25 % NaOCl irrigation as a control group.
The assignment of the specimens to the groups was performed in a double-blind manner.
During the laser irradiation cycles, the root canals were steadily irrigated with a 2-ml fluid in order to maintain hydration and levels, using a hand syringe with a 27-gauge needle which was positioned at the root canal entrance, accordingly to the above protocol (Fig. 2). Thereafter, the group 1, 2, and 3 specimens were immediately rinsed with saline water, and the group 4 specimens were rinsed with saline water after 30 min.

The use of Er, Cr:YSGG laser during the experimental procedures
The E. faecalis residual colonies in the root canal were extracted with sterile paper points which were left in the canal for 1 min and then transferred into tubes containing 5 ml of BHI broth. The broths were vortexed and incubated at 37 °C to a maximum of 4 days. An aliquot of 100 μl of each broth tube was then subcultured onto two vancomycin-resistant enterococci (VRE) agar base plates, whilst the remaining broth was incubated at 37 °C for 4 days. This allowed for a qualitative and quantitative assessment of bacterial survival. The turbidity of the incubated broth was inspected every day for 4 days, and, when present, the presence of E. faecalis was confirmed by subculturing the broth onto VRE agar.
Microbiological procedures were performed in a blind manner.
The laser
An Er, Cr:YSGG laser (Biolase, Irvine, CA) with a wavelength of 2,780 nm was used to irradiate the root canals after mechanical instrumentation (Fig. 3). The laser operating parameters used for groups 1 and 2 (using the free-running emission mode) were as follows: E = 75 mJ, 0.75 W, 10 pulses per second, with a pulse duration of 140 μs, and peak power of 535 W. The laser was set at E = 25 mJ, 0.25 W, 10 pulses per second, with a pulse duration of 140 μs, and peak power of 178 W for group 3 specimens. The coaxial water spray feature of the handpiece was set to off. The tip (Waterlase MD Endolase RFT; diameter = 200 μm; length = 25 mm) was placed at the root canal entrance, and it was kept stationary and not advanced any further into the canal. The loss of power was as much as 70 %, with the use of this tip.

The Er, Cr:YSGG laser used in the study
Statistical analysis
The data obtained were statistically analyzed for differences using the Fisher exact test, comparing pairs of groups, with a significant level established at P < 0.05. Data management and analysis were performed using a statistical software program (StatView 5.0.1., SAS Institute, Inc. Cary, NY).
Results
The data obtained for each treatment group are presented in Table 1.
A bactericidal effect was observed for all groups. One of the previously contaminated root canals untreated with laser and one that had received laser irradiation lasting for 30 s yielded positive cultures. Bacterial growth was verified in six specimens treated with the laser for 60 s (E = 25 mJ). E. faecalis was recovered from all positive cultures, and a positive culture was not detected among the group 2 specimens.
The use of the laser at 30 and 60 s (E = 75 mJ) eliminated 92.3 and 100 % of E. faecalis, respectively, and a reduction of 92.3 % was observed in the control group; a lower reduction percentage (46.1 %) was obtained for the group 3 specimens. No statistical differences were observed between the four groups (P = 0.543, Fisher’s exact test).
Discussion
In this study, the root canal system was contaminated with E. faecalis, a facultative Gram-positive anaerobic coccus, also known as an endodontic pathogen. It was selected for use because it exhibits a high level of resistance to a wide range of antimicrobial agents, and it is frequently recovered from the root canals of teeth associated with posttreatment diseases [2–5]. Instrumentation techniques using rotary instruments and chemical irrigation still fail to completely eliminate this microorganism from inside the root canal. It is important to validate the bactericidal action of different methods by using a resistant microorganism such as E. faecalis. In addition to its resistance, the persistence of E. faecalis is associated with the difficulty of hand-irrigated, antimicrobial agents reaching various areas of the root canal system (apical third of the canal, oval extensions, isthmuses, and anastomoses) and penetrating into the dentinal tubules.
The use of lasers at different wavelengths has been proposed to supplement conventional endodontic cleaning procedures in order to enhance the success of this treatment. The action of the laser is founded not on the direct elimination of microorganisms by thermal vaporization but probably by the photomechanical streaming of fluids which were laser-activated in the coronal portion of the tooth, with the formation of a cavity containing bubbles inside a fluid (cavitation). This light energy phenomenon is described as photon-induced photoacoustic streaming [20]. This process can allow the irrigants to access otherwise inaccessible areas more easily, which might be of assistance in the cleaning of canals of various shapes. In addition, the cavitation bubbles expand, become unstable, and then collapse (implosion) [21]. This implosion will have an impact on the surfaces of the root canal, causing shear forces, surface deformation, and the removal of surface material [22].
In this study, an Er, Cr:YSGG laser was developed. During the experimental procedures, the tip of the laser was accurately placed in the coronal portion of the root and kept there for the entire duration of irradiation. Thus, the undesired effects of the thermal energy (previously described in the literature) were avoided. Moreover, it has been suggested that this facilitates the occurrence of the photomechanical effects in the root canal, and this may be of use in cleaning canals of different shapes [23]. As the laser beam delivers energy only where it is focused, a special 200-μm diameter endodontic fiber tip was used to enhance directing the laser light into the root canals. Moreover, access to the entrance of the root canal was improved by virtue of the reduced dimension of the tip.
The Er, Cr:YSGG laser was tested for different irradiation times (30 and 60 s) and at different impulse energies to investigate the importance of time as a variable for the effectiveness of the bactericidal action, as reported in previous studies [23, 24]. The different impulse energies (75 vs 25 mJ) were used in order to detect any differences in the effectiveness of disinfection in the absence of any thermal potential. As the tooth root is in contact with the alveolar bone (via the periodontal membrane and ligament), thermal injury to the periodontal tissues is of concern during laser use for intracanalar applications. Thus, the use of low energy would be beneficial in minimizing the increase in temperature in the surrounding areas.
In this study, a solution of sodium hypochlorite was applied to the root canals for 30 min because the latter corresponds to the time required for this agent to be activated [25]. The time difference between laser and sodium hypochlorite treatments (30 and 60 s vs 30 min) is acknowledged, and it reflects clinical conditions.
The results of this study have demonstrated a bactericidal effect of Er, Cr:YSGG laser irradiation at the settings used in this study. The highest bactericidal effect of this laser was observed for an irradiation time of 60 s with an impulse energy of 75 mJ. Bacterial growth of E. faecalis was verified in six specimens treated with laser for 60 s at E = 25 mJ, in one specimen treated with laser for 30 s at E = 75 mJ, and in the control group. A greater degree of disinfection was thus observed at higher irradiation times and impulse energies. However, these differences did not prove to be statistically significant.
Similar results have been obtained by Arnabat et al. [26] who investigated the effectiveness of the Er, Cr:YSGG laser by measuring its bactericidal effect inside root canals, experimentally colonized with E. faecalis. They concluded that NaOCl 5 % was as effective as the laser with an irradiation time of 60 s. However, the laser was set at a higher power in their study than that of this study (2 vs 0.25 W and 0.75 W). Thus, the impulse energy used would consequently be higher with the probable development of a thermal effect [26].
Cheng et al. [27] reached a similar conclusion when they tested an Er, Cr:YSGG laser for disinfecting root canals contaminated with E. faecalis. The bacterial reductions in the root canals treated with laser were significantly greater after treatment than those obtained after only being treated with saline [27]. The ability of an Er, Cr:YSGG laser to disinfect E. Faecalis-infected canal roots was also investigated by Gordon et al. [24]. As in this study, the authors found that bacterial recovery decreased with increasing laser irradiation duration or power [24].
A correlation between the duration of Er, Cr:YSGG laser irradiation and its effectiveness in removing a smear layer and debriding the root canal walls was also found by DiVito et al. [23]. They showed that root canals irradiated for 40 s were significantly cleaner than those irradiated for 20 s. Unlike our study, they showed that standardized instrumentation, followed by a final Er:YAG laser irradiation resulted in significantly improved smear layer removal than was the case with traditional irrigation methods. However, the root canals of the control group were irrigated with saline, which does not have an antibacterial effect [23].
The irradiation time was also analyzed by Peeters and Suardita [28], who observed the total absence of a smear layer in root canals treated with Er, Cr:YSGG laser for 60 s, while the root canals of teeth irradiated for 30 s exhibited a moderate smear layer [28]. Different results to this study were also reached by Eldeniz et al. [29] who compared the efficacy of Er, Cr;YSGG laser with 3 % NaOCl in root canals contaminated with E. faecalis using similar experimental procedures. Their findings showed that treatment with laser reduced the viable microbial population in root canals, but it did not eradicate all bacteria, while the NaOCl solution effectively sterilized all root canals. However, in this study by Eldeniz et al. [29], the pulse energy setting was not specified (the authors referred to a range of between 25 and 300 mJ) and the tip was inserted into the root canal and moved from the apex to crown; therefore, it is not possible to make a comparison between the two studies [29].
It is the opinion of the authors of this paper that an Er, Cr:YSGG laser used at E = 75 mJ and irradiated for 60 s constitutes a valid alternative to conventional treatment protocols (without a laser). One reason is the greatly reduced time required for total disinfection which was obtained by using a laser compared with the time spent during treatment using chemical–mechanical protocols; in our study, the same bactericidal potential was observed when the laser was used for 60 s and when irrigation was reduced in the root canals after a period of 30 min. This is an important advantage (a) for the dentist who could perform a successful endodontic disinfection, reducing operative times, and (b) for patients who would benefit from reduced recovery time, thereby minimizing fear and anxiety. Moreover, the complete sterilization of root canals was observed in this study when the laser was used for 60 s at 75 mJ. The study demonstrated that the photoactivated irrigant could reach all bacterial cells and also those located in the irregularities of the root canal. On the other hand, root canals of teeth treated without laser revealed the persistence of E. faecalis, even to a small degree. In a clinical setting, this would be associated with unsuccessful endodontic treatment.
Furthermore, the activation of NaOCl by the Er, Cr:YSGG laser enables the irrigant to reach less accessible areas without any risk to the patient [30]; NaOCl is unselective and damages human cells, dentine, and periodontal tissues with clinical consequences. The branches of the facial nerves or the inferior alveolar nerve have been reported to have been affected by NaOCl which can lead to severe sequelae [31, 32]. This could happen when irrigation is performed at high pressure, with a discharge of the irrigant exiting the apex. Newly developed commercial devices for irrigating have been proposed which would permit the dissemination of NaOCl throughout the canal areas, thus minimizing the risk of discharge. To date, these devices have met with little success due to their complexity of use [33, 34]; the use of lasers with the tip placed in the coronal aspect of the canal involves minimal risk, requiring a shallower learning curve by the operator.
In conclusion, the results presented in this paper indicate a bactericidal effect of Er, Cr:YSGG laser irradiation for the settings used in this study. Chemical–mechanical treatment in the absence of a laser, as recommended by the standard protocol, has demonstrated the same potential. Moreover, the highest bactericidal effect of this laser was observed at a 60-s irradiation time with a pulse energy of 75 mJ, although the differences between the groups were not statistical significant. These findings suggest that the addition of laser treatment to conventional treatment protocols provides similar bactericidal effects to conventional treatment alone but in a shorter time. These results are of practical relevance as they have demonstrated that the use of Er, Cr:YSGG laser leads to a high bactericidal effect with a significant reduction in operative times (for dentists and patients), with a shallower learning curve for dentists. Moreover, the clinical procedures performed in endodontic treatment with this laser greatly reduce any risk to the patient.
References
Gomes BP, Pinheiro ET, Gadê-Neto CR et al (2004) Microbiological examination of infected dental root canals. Oral Microbiol Immunol 19:71–76
Hancock HH, Sigurdsson A, Trope M, Moiseiwitsch J (2001) Bacteria isolated after unsuccessful endodontic treatment in a North American population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 91:579–586
Pinheiro EP, Gomes BP, Ferraz C et al (2003) Microorganisms from canals of root-filled teeth with periapical lesions. Int Endod J 36:1–11
Sood S, Malhotra M, Das BK, Kapil A (2008) Enterococcal infections & antimicrobial resistance. Indian J Med Res 128:111–121
Skucaite N, Peciuliene V, Vitkauskiene A, Machiulskiene V (2010) Susceptibility of endodontic pathogens to antibiotics in patients with symptomatic apical periodontitis. J Endod 36:1611–1616
Peters OA, Peters CI, Schonenberger K, Barbakow F (2003) ProTaper rotary root canal preparation: effects of canal anatomy on final shape and analysed by micro CT. Int Endod J 36:86–92
de los Angeles Bulacio M, Raiden G (2009) Dye diffusion in instrumented root canals irrigated with different solutions. Acta Odontol Latinoam 22:207–214
Alves FR, Almeida BM, Neves MA et al (2011) Disinfecting oval-shaped root canals: effectiveness of different supplementary approaches. J Endod 37:496–501
Zou L, Shen Y, Li W, Haapasalo M (2010) Penetration of sodium hypochlorite into dentin. J Endod 36:793–6
Kuga MC, Gouveia-Jorge É, Tanomaru-Filho M et al (2011) Penetration into dentin of sodium hypochlorite associated with acid solutions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 112:155–159
Pérez-Heredia M, Ferrer-Luque CM, González-Rodríguez MP (2006) The effectiveness of different acid irrigating solutions in root canal cleaning after hand and rotary instrumentation. J Endod 32:993–997
Nair PNR, Henry S, Cano V et al (2005) Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after ‘one-visit’ endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:231–252
Kimura Y, Wilder Smith P, Matsumoto K (2000) Laser in endodontics: a review. Int Endod J 33:173–85
Sadık B, Arıkan S, Beldüz N et al (2013) Effects of laser treatment on endodontic pathogen Enterococcus faecalis: a systematic review. Photomed Laser Surg 31:192–200
Sulewski JG (2009) Making the most of the 16th Annual Conference and Exhibition: a practical orientation for attendees. In: Academy of Laser Dentistry 16th annual conference and exhibition, Las Vegas, Nevada
Plotino G, Grande NM, Falanga A et al (2007) Dental removal in the coronal portion of root canals following two preparation techniques. Int Endod J 40:853–858
Neglia R, Ardizzoni A, Giardino L et al (2008) Comparative in vitro and ex vivo studies on the bactericidal activity of Tetraclean, a new generation endodontic irrigant, and sodium hypochlorite. New Microbiol 31:57–65
Siqueira JF, Machado AG, Silveira RM, Lopes HP, De Uzeda M (1997) Evaluation of the effectiveness of sodium hypochlorite used with three irrigation methods in the elimination of Enterococcus faecalis from the root canal in vitro. Int Endod J 30:279–282
Oncag O, Hosgor M, Hilmioglu S et al (2003) Comparison of antibacterial and toxic effects of various root canal irrigants. Int Endod J 36:423–432
Levy G, Rizoiu I, Friedman S, Lam H (1996) Pressure waves in root canals induced by Nd: YAG laser. J Endod 22:81–4
Gutarts R, Nusstein J, Reader A, Beck M (2005) In vivo debridement efficacy of ultrasonic irrigation following hand-rotary instrumentation in human mandibular molars. J Endod 31:166–170
Tomita Y, Shima A (1986) Mechanisms of impulsive pressure generation and damage pit formation by bubble collapse. J Fluid Mech 169:535–564
DiVito E, Peters OA, Olivi G (2012) Effectiveness of the erbium:YAG laser and new design radial and stripped tips in removing the smear layer after root canal instrumentation. Lasers Med Sci 27:273–280, 18
Gordon W, Atabakhsh VA, Meza F et al (2007) The antimicrobial efficacy of the erbium, chromium:yttrium-scandium-gallium-garnet laser with radial emitting tips on root canal dentin walls infected with Enterococcus faecalis. J Am Dent Assoc 138:992–1002
Del Carpio-Perochena AE, Bramante CM, Duarte MA et al (2011) Biofilm dissolution and cleaning ability of different irrigant solutions on intraorally infected dentin. J Endod 37:1134–1138
Arnabat J, Escriban C, Fenosa A et al (2012) Bactericidal activity of erbium, cromium: yttrium-scandium-gallium-garnet laser in root canals. Lasers Med Sci 25:805–810
Cheng X, Guan S, Lu H et al (2012) Evaluation of the bactericidal effect of Nd:YAG, Er:YAG, Er, Cr:YSGG laser radiation, and antimicrobial photodynamic therapy (aPDT) in experimentally infected root canals. Lasers Surg Med 44:824–831
Peeters HH, Suardita K (2011) Efficacy of smear layer removal at the root tip by using ethylenediaminetetraacetic acid and erbium, chromium: yttrium, scandium, gallium garnet laser. J Endod 37:1585–1589
Eldeniz AU, Ozer F, Hadimli HH, Erganis O (2007) Bactericidal efficacy of Er, Cr; YSGG laser irradiation against Enterococcus faecalis compared with NaOCl irrigation: an ex vivo pilot study. Int End J 40:112–119
Peeters HH, Mooduto L (2012) Radiographic examination of apical extrusion of root canal irrigants during cavitation induced by Er, Cr:YSGG laser irradiation: an in vivo study. Clin Oral Investig. doi:10.1007/s00784-012-0910-2
Hülsmann M, Hahn W (2000) Complications during root canal irrigation literature: review and case reports. Int Endod J 33:186–193
Zairi A, Lambrianidis T (2008) Accidental extrusion of sodium hypochlorite into the maxillary sinus. Quintessence Int 39:745–748
Pawar R, Alqaied A, Safavi K, Boyko J, Kaufman B (2012) Influence of an apical negative pressure irrigation system on bacterial elimination during endodontic therapy: a prospective randomized clinical study. J Endod 38:1177–1181
de Gregorio C, Paranjpe A, Garcia A et al (2012) Efficacy of irrigation systems on penetration of sodium hypochlorite to working length and to simulated uninstrumented areas in oval shaped root canals. Int Endod J 45:475–481
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Licata, M.E., Albanese, A., Campisi, G. et al. Effectiveness of a new method of disinfecting the root canal, using Er, Cr:YSGG laser to kill Enterococcus faecalis in an infected tooth model. Lasers Med Sci 30, 707–712 (2015). https://doi.org/10.1007/s10103-013-1410-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-013-1410-6