
Abstract
The aim of this narrative review was to critically evaluate in vitro studies assessing the efficacy of lasers in the bacterial decontamination of titanium implant surfaces. The MEDLINE, Web of Knowledge and Embase electronic databases were used to search for articles relating to the use of lasers in the bacterial decontamination of titanium specimen surfaces using predetermined search statements. Clinical studies, case reports, case series, review articles and animal models were excluded. Study selection was carried out independently and then cross-checked by two authors through abstract viewing. Eighteen articles were selected for full-text analysis. Erbium-doped yttrium–aluminium–garnet lasers had a wide range of powers capable of inducing bacterial decontamination. While carbon dioxide and gallium–aluminium–arsenide diode lasers demonstrated the ability to produce bacterial decontamination, the bacterial sensitivity to each varied depending on the species involved. There is no concensus on the laser type or settings that are optimal for bacterial decontamination of titanium implant surfaces as studies employ various test specimens, contamination methodologies, irradiation settings and protocols, and outcome measures resulting in limited study comparability. More investigations are required to provide guidelines for the use of laser therapy in the decontamination of implant surfaces.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Peri-implantitis is an infectious inflammatory disease associated with bleeding, suppuration and the loss of supporting bone around functioning osseo-integrated implants [1]. The presence of gram-negative anaerobic biofilm on the implant surface has been implicated in the aetiology of peri-implantitis [2].
The high prevalence, ranging from 16 to 47.1 %, of peri-implantitis has led researchers to investigate a number of therapeutic interventions for implant surface decontamination [3, 4]. These include mechanical debridement, chemical disinfection, sustained release antibiotics, and regenerative and resective surgical therapy. Recent studies have indicated that there is no gold standard for the management of peri-implantitis with most of the modalities being incapable of achieving complete removal of inflammatory tissue, bony defect debridement or implant surface decontamination [5]. Current therapies offer limited clinical improvements and have almost no microbiological improvements 6 months after treatment [5].
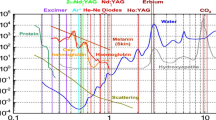
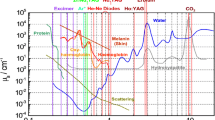
Laser irradiation has been suggested as a strategy for surface decontamination in the treatment of peri-implantitis. Multiple lasers, including erbium-doped yttrium–aluminium–garnet (Er:YAG), carbon dioxide (CO2), gallium–aluminium–arsenide (GaAlAs) diode, neodymium-doped yttrium–aluminium–garnet (Nd:YAG) and erbium- and chromium-doped yttrium–scandium–gallium–garnet, have been evaluated. Before applying an irradiation protocol at the patient level, in vitro testing is necessary to determine the optimal settings for decontamination. Currently, there is no standard recommendation pertaining to the laser type, settings or irradiation protocol for the treatment of peri-implantitis. In order to meet this objective, it is necessary to analyse the available literature in order to develop a set of evidence-based settings and protocols for laser irradiation.
As such, it is the aim of this narrative review to critically evaluate in vitro studies assessing the efficacy of lasers in the bacterial decontamination of titanium implant surfaces.
Methodology
Study selection
The MEDLINE, Web of Knowledge and Embase electronic databases were used to search for articles relating to the use of lasers in the bacterial decontamination of titanium specimen surfaces. Four literature searches were carried out using the following key words:
-
1.
(peri-implantitis or periimplantitis or peri implantitis or periimplant or peri-implant or periimplant lesions or peri-implant lesions) and (laser or lasers)
-
2.
(contaminated or contamination or infected or infection) and (titanium or implant or implants) and (laser or lasers)
-
3.
(in vitro or model or trial) and (contaminated or contamination or infected or infection) and (titanium or implant or implants) and (laser or lasers)
-
4.
(in vitro or model or trial) and (decontaminated or decontamination or disinfected or disinfection) and (titanium or implant or implants) and (laser or lasers)
The search parameters included all studies reported in English, published within the past 20 years, current to 8 February 2012. Abstracts were read and in vitro studies investigating the effect of laser therapy in the bacterial decontamination of titanium specimens were selected. Clinical studies, case reports, case series, animal studies and review articles were excluded.
The search on both databases was carried out independently by MSK and AK. Using the search criteria, each author selected articles to be included in the review. The selections were cross-checked and any discrepancies were resolved by viewing the full text, reviewing the predetermined criteria and seeking the opinion of the third author, ATS. During the independent selection process, if uncertainty regarding the decision to include a paper was encountered, each of the authors was capable of gaining a second opinion via consulting ATS.
Data abstraction
Following the cross-checking of the selected studies, a Microsoft Excel spreadsheet to homogenise the data abstraction categories was formulated. Specimen data collected included titanium grade, geometric dimensions and surface type. Contamination protocol and laser settings including laser type, power, tip, irradiation distance, duration, angle and mechanism were recorded. Finally, the decontamination evaluation mechanism and outcomes as well as observed morphological alterations were recorded.
Independent data abstraction was carried out by MSK and AK followed by a cross-checking of the collated data. Any discrepancies or deficiencies in the data were resolved through combined reviewing of the article full text.
Data analysis
A qualitative comparison was carried out to examine the level of implant surface decontamination achieved by each laser.
Results
Initial search results gave a total of 419 articles through the MEDLINE database, 952 articles through the Web of knowledge database and 531 articles through the Embase database. Eighteen articles were selected for full-text analysis [6–23]. The potential of lasers to decontaminate titanium implant surfaces was confirmed by all the studies [6–20, 22, 23] except Block et al. [21].
The majority of the studies evaluated the decontamination outcome using either scanning electron microscopy (SEM) [9, 10, 14, 18, 19], counting the colony forming units (CFU) [6, 8, 12, 20–23] or a combination of these techniques [11]. Less common evaluation techniques included bacterial smears [7], light microscopy images to evaluate clean implant surface percentages [13, 15–17] and photometric XTT–formazan evaluations [19].
A variety of settings were investigated for the use of the Er:YAG laser in inducing surface decontamination (Table 1). Decontamination efficacy was dose-dependent with values ranging from 59 % following irradiation with 80 mJ/pulse at 5 Hz [20] to 99.94 % following irradiation with 120 mJ/pulse at 10 Hz [11]. Tosun et al. [20] demonstrated that using Er:YAG laser in the very short pulse (VSP) mode gave greater bactericidal activity at any given power than the short pulse (SP) mode but that 100 % bactericidal effects were only consistently achieved at 90 mJ/pulse at 10 Hz in SP mode.
Similarly, the CO2 laser showed dose-dependent decontamination efficacy with values ranging from 68 % following irradiation with 2–4 W (10 ms/pulse, 20 Hz) to 100 % following irradiation with 6 W (20 ms/pulse, 20 Hz) [20] (Table 2). Kato et al. [8] reported that Streptococcus sanguinis has more resistance to CO2 irradiation than Porphyromonas gingivalis when a range of energies from 15 to 40 J was examined; these findings were consistent with the other literature [22].
The GaAlAs diode laser yielded variable decontamination results with the efficacy increasing in a dose-dependent manner similar to the Er:YAG and CO2 lasers (Table 3). The decontamination capacity increased from 45 % at 0.5 W to 99.9 % at 2.5 W [12], but multiple studies reported that complete bacterial elimination is not possible [12, 19]. However, Tosun et al. [20] displayed 100 % decontamination at powers as low as 1 W; this was consistent with Sennhenn-Kirchner et al. [23] where mean bacterial reduction ranges were between 94.67 and 100 %. Enterococcus faecalis and S. sanguinis were more resistant to GaAlAs diode laser irradiation than P. gingivalis [6, 22]. This is similar to the CO2 laser where P. gingivalis was more susceptible to irradiation compared to other microbial species.
The Nd:YAG laser gave variable decontamination values with studies showing incomplete elimination of the microbial organisms for powers ranging from 0.3 to 3.0 W [16, 21]; meanwhile, Gonçalves et al. [6] showed 100 % bacterial elimination using 3.0 W (Table 4). In a similar manner to the CO2 and GaAlAs diode lasers, the Nd:YAG laser demonstrated variable decontamination of microbial organisms with E. faecalis having higher resistance to irradiation than P. gingivalis [6].
Discussion
This narrative review evaluated in vitro studies assessing the efficacy of lasers in the bacterial decontamination of dental implant surfaces.
Er:YAG lasers were the most consistent in inducing near-complete or complete bacterial decontamination over a wide range of powers (30–120 mJ/pulse, 10–30 Hz, SP mode). Both the CO2 and GaAlAs diode lasers demonstrated near-complete bacterial decontamination capacities with 4–7 W at 20–80 Hz and 3 W, respectively, yet the number of studies showing complete bacterial elimination was equivocal. Additionally, microbes demonstrated different levels of resistance when irradiated with these lasers, indicating a potentially lower irradiation efficacy against a combined bacterial biofilm such as that involved in the aetiology of peri-implant diseases. There was no clear consensus in the analysed literature on the capacity of Nd:YAG laser in inducing complete decontamination of infected titanium specimens. An optimal irradiation protocol could not be reached for the evaluated lasers due to researchers employing differing test specimens, contamination methodologies, irradiation settings and outcome measures, which limited study comparability.
The level of decontamination varied for different titanium surfaces within the same trial where all other variables were controlled [6, 7, 11, 12, 18]. As a specific example, Quaranta et al. [18] reported decontamination values of 76.2 % for machined, 90.9 % for TPS and 98.3 % for sandblasted or acid-etched surfaces when using the Er:YAG laser with matching irradiation protocols. Thus, surface-specific factors rendered a particular surface easier or more challenging to decontaminate compared to another. Similarly, specimen geometry modified the level of decontamination. Root form is more supportive of bacterial growth due to its multiple crevices and threads. Elimination of bacterial species may occur less readily on a root-form specimen due to lowered laser access. Combining the root-form's higher contamination surface area and the lower laser access will lead to lower decontamination potential of a laser. Therefore, baseline specimen geometry and surface properties can affect the observed outcome, which limits the study comparability.
The comparability of the studies' outcomes has been limited by the variable contamination protocols. Given the varying levels of resistance of single microbial biofilm to a constant laser irradiation protocol [6, 8, 22], it is unfeasible to compare decontamination trials which used an indeterminate mixture of microbiological species from an intra-oral environment [9, 10, 13–15, 17, 23]. Incorporation of more resistant organisms in the infection protocol will lend a less favourable decontamination result to the laser used compared to a single susceptible microbial biofilm. Furthermore, the use of species that are not implicated in peri-implant disease, such as Bacillus subtilis [21], will skew the decontamination results. Studies allowed variable contamination time for biofilm formation following bacterial contamination, ranging from 10 min [20] to 10 days [23]. While a short duration may result in a less stable biofilm due to insufficient maturation time, a longer duration produces a degenerate biofilm secondary to noxious product formation and reduced nutrient availability. An appropriate length of contamination allows the formation of a stable biofilm, the protective nature of which decreases the efficacy of decontamination with laser irradiation. Incomplete or degenerate inconsistent biofilms provide a more favourable decontamination result but make it difficult to assess whether the lack of residual biofilm is due to the laser irradiation or due to the contamination protocol itself.
Exposure to the laser light energy gives phototoxic effects through inducing reactive oxygen species (ROS) production by the bacteria [24]. The amount of ROS production depends on the wavelength, hence the variable lasers' decontamination potential. Power settings dictate the actual rate of energy transfer to the surface per unit time and are directly proportional to the level of ROS production and the level of expected bacterial kill. Various powers were employed in the included studies ranging from 30 to 200 mJ/pulse (5–30 Hz) in Er:YAG, from 1.2 to 7 W in CO2, from 0.25 to 3 W in GaAlAs diode and from 0.3 to 3 W in Nd:YAG. Furthermore, power is determined by both the amount of energy per pulse as well as the frequency of pulses; alterations to these two key determinants can give a different true amount of energy experienced by the specimen per unit area. Studies did not always fully define the settings with respect to these two variables, hence limiting comparability.
Choices of tip type, distance between tip and specimen, irradiation time, mode and mechanism all influence the true amount of energy that the specimen receives which is different to the initial predetermined power. Schwarz et al. [15] demonstrated the reduction of the power of the Er:YAG laser from 100 mJ/pulse at 10 Hz as the base setting to 85 mJ/pulse at 10 Hz delivered to the titanium specimen using the cone-shaped glass fibre tip. Distances ranged from 0.5 mm [11, 13, 19, 22] to 30 mm [14]. As the distance between the tip and the irradiated specimen increases, the true energy experienced by the specimen will be reduced and the decontamination outcome will be less favourable. Likewise, the wide irradiation angle variation from 13° [13] to 90° [6, 22] gave variable decontamination because smaller irradiation angles give stronger waves. Irradiation times ranged from 3–4 s [16] to 336 s [15]; meanwhile, other studies did not report on this value [10, 21]. The time elapsed defines the total amount of energy delivered to the surface. The use of different mechanisms such as sweeping motion [13], apex-crown motions [18], manual scanning of disc surfaces [20], parallel irradiation in contact mode [15], successively enhanced concentric circles [11] and bilateral irradiation [19] will result in variable lengths of unit area exposure to the laser irradiation within a fixed time frame. Thus, the variable setting combinations make it difficult to correlate the reported power values to the actual decontamination outcomes and disable accurate comparisons between the studies.
Laser power output can be either continuous over the irradiation time or pulsed at a given frequency. The pulsed mode has been used in periodontal applications because the small volume of contaminated material and bacterial plaque on the implant surface can be evaporated if it is heated for a very short period of time [25]. However, a continuous mode supplies the energy gradually and allows for the heat to be absorbed into the bulk of the implant without attaining a sufficiently high temperature to evaporate the debris, resulting in lower surface decontamination [25]. The use of GaAlAs diode laser in a continuous wave mode resulted in equivocal evidence on the likelihood of complete bacterial decontamination.
Finally, different analytical techniques were used to measure the decontamination outcomes at different levels. While light microscopy examines bacterial biofilm presence at the macroscopic level at relatively lower magnification, SEM carries out this analysis at a much higher magnification, which may entail more sensitivity and higher accuracy on reporting bacterial presence. However, these qualitative examinations provide no assessment of the viability of the residual bacterial plaque biofilm. CFU and bacterial smear tests examine the presence of viable species by assessing regrowth following an irradiation episode. However, variation has been observed in the carrying out of the CFU analysis and the different results can be the product of the utilisation of various dilutions. The analytical techniques measure various qualities at the macroscopic and microscopic level. This renders it substantially difficult to compare the different methods, the sensitivity of which can be questionable.
Energy transfer to a titanium surface to induce decontamination is associated with the development of surface colour changes and morphological damage. As the temperature surpasses the metallic melting and boiling thresholds of the surface, slip-line formation, ripple patterns, flat melting, crater-like formation and boiling occur [26]. It is unclear whether surface alterations will occur as a result of laser irradiation as variable results have been reported in the examined studies depending on the laser type and settings as well as the analytical mechanisms.
The comparability of the studies has been limited, and it was difficult to assess the extent to which the validity of the irradiation protocol conclusions has been affected by the wide variety in study design and outcome measures. This presents a clear need for devising a standardised irradiation protocol that is safe for in vivo use, is efficacious in bacterial decontamination and causes minimal surface alteration.
References
Lindhe J, Meyle J (2008) Peri-implant diseases: consensus report of the sixth European workshop on periodontology. J Clin Periodontol 35:282–285. doi:10.1111/j.1600-051X.2008.01283.x
Mombelli A, Décaillet F (2011) The characteristics of biofilms in peri-implant disease. J Clin Periodontol 38:203–213. doi:10.1111/j.1600-051X.2010.01666.x
Roos-Jansaker AM, Lindahl C, Renvert H, Renvert S (2006) Nine to fourteen year follow up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol 33:290–295
Koldsland OC, Scheie AA, Aass AM (2010) Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol 81(2):231–238. doi:10.1902/jop.2009.090269
Schwarz F, John G, Mainusch S, Sahm N, Becker J (2012) Combined surgical therapy of peri-implantitis evaluating two methods of surface debridement and decontamination. A two-year clinical follow up report. J Clin Periodontol 39:789–797. doi:10.1111/j.1600-051X.2012.01867.x
Gonçalves F, Zanetti AL, Zanetti RV, Martelli FS, Avila-Campos MJ, Tomazinho LF, Granjeiro JM (2010) Effectiveness of 980-nm diode and 1064-nm extra-long-pulse neodymium-doped yttrium aluminum garnet lasers in implant disinfection. Photomed Laser Surg 28:273–280. doi:10.1089/pho.2009.2496
Haas R, Dörtbudak O, Mensdorff-Pouilly N, Mailath G (1997) Elimination of bacteria on different implant surfaces through photosensitization and soft laser. Clin Oral Impl Res 8:249–254
Kato T, Kusakari H, Hoshino E (1998) Bactericidal efficacy of carbon dioxide laser against bacteria-contaminated titanium implant and subsequent cellular adhesion to irradiated area. Laser Surg Med 23:299–309
Mouhyi J, Sennerby L, Pireau JJ, Dourov N, Nammour S, van Reck J (1998) An XPS and SEM evaluation of six chemical and physical techniques for cleaning of contaminated titanium implants. Clin Oral Impl Res 9:185–194
Mouhyi J, Sennerby L, Wennerberg A, Louette P, Dourov N, van Reck J (2000) Re-establishment of the atomic composition and the oxide structure of contaminated titanium surfaces by means of carbon dioxide laser and hydrogen peroxide: an in vitro study. Clin Implant Dent Relat Res 2:190–202
Kreisler M, Kohnen W, Marinello C, Götz H, Duschner H, Jansen B, d’Hoedt B (2002) Bactericidal effect of the Er:YAG laser on dental implant surfaces: an in vitro study. Periodontol 73:1292–1298. doi:10.1902/jop.2002.73.11.1292
Kreisler M, Kohnen W, Marinello C, Schoof J, Langnau E, Jansen B, Nat R, d’Hoedt B (2003) Antimicrobial efficacy of semiconductor laser irradiation on implant surfaces. Int J Oral Maxillofac Implants 18:706–711
Matsuyama T, Aoki A, Oda S, Yoneyama T, Ishikawa I (2003) Effects of the Er:YAG laser irradiation on titanium implant materials and contaminated implant abutment surfaces. J Clin Laser Med Surg 21:7–17
Shibli JA, Theodoro LH, Haypek P, Garcia VG, Marcantonio E (2004) The effect of CO2 laser irradiation on failed implant surfaces. Implant Dent 13:342–348
Schwarz F, Sculean A, Romanos G, Herten M, Horn N, Scherbaum W, Becker J (2005) Influence of different treatment approaches on the removal of early plaque biofilms and the viability of SAOS2 osteoblasts grown on titanium implants. Clin Oral Invest 9:111–117. doi:10.1007/s00784-005-0305-8
Giannini R, Vassalli M, Chellini F, Polidori L, Dei R, Giannelli M (2006) Neodymium:yttrium aluminum garnet laser irradiation with low pulse energy: a potential tool for the treatment of peri-implant disease. Clin Oral Impl Res 17:638–643. doi:10.1111/j.1600-0501.2006.01278.x
Schwarz F, Nuesry E, Bieling K, Herten M, Becker J (2006) Influence of an erbium, chromium-doped yttrium, scandium, gallium, and garnet (Er, Cr:YSGG) laser on the reestablishment of the biocompatibility of contaminated titanium implant surfaces. J Periodontol 77:1820–1827. doi:10.1902/jop.2006.050456
Quaranta A, Maida C, Scrascia A, Campus G, Quaranta M (2009) Er:YAG laser application on titanium implant surfaces contaminated by Porphyromonas gingivalis: an histomorphometric evaluation. Minerva Stomatol 58:317–330
Sennhenn-Kirchner S, Schwarz P, Schliephake H, Konietschke F, Brunner E, Zepelin MB (2009) Decontamination efficacy of erbium:yttrium-aluminium-garnet and diode laser light on oral Candida albicans isolates of a 5-day in vitro biofilm model. Lasers Med Sci 24:313–320. doi:10.1007/s10103-008-0561-3
Tosun E, Tasar F, Strauss R, Kwanc DG, Ungor C (2012) Comparative evaluation of antimicrobial effects of Er:YAG, diode, and CO2 lasers on titanium discs: an experimental study. J Oral Maxillofac Surg 70(5):1064–1069. doi:10.1016/j.joms.2011.11.021
Block CM, Mayo JA, Evans GH (1992) Effects of the Nd:YAG dental laser on plasma-sprayed and hydroxyapatite-coated titanium dental implants: surface alteration and attempted sterilization. Int J Oral Maxillofac Implants 7:441–449
Hauser-Gerspach I, Stübinger S, Meyer J (2010) Bactericidal effects of different laser systems on bacteria adhered to dental implant surfaces: an in vitro study comparing zirconia with titanium. Clin Oral Impl Res 21:277–283. doi:10.1111/j.1600-0501.2009.01835.x
Sennhenn-Kirchner S, Klaue S, Wolff N, Mergeryan H, Borg von Zepelin M, Jacobs H (2007) Decontamination of rough titanium surfaces with diode lasers: microbiological findings on in vivo grown biofilms. Clin Oral Impl Res 18:126–132. doi:10.1111/j.1600-0501.2006.01298.x
Lipovsky A, Nitzan Y, Gedanken A, Lubart R (2010) Visible light-induced killing of bacteria as a function of wavelength: implication for wound healing. Lasers Surg Med 42:467–472. doi:10.1002/lsm.20948
Ishikawa I, Aoki A, Takasaki A, Mizutani K, Sasaki K, Izumi Y (2009) Application of lasers in periodontics: true innovation or myth? Perio 50:90–126. doi:10.1111/j.1600-0757.2008.00283.x
Jee Y, Becker MF, Walser RM (1988) Laser-induced damage on single-crystal metal surfaces. J Opt Soc Am B 5:648–659
Acknowledgments
The support of the Sir John Walsh Research Institute was acknowledged.
Conflict of interest
The authors declare that there are no conflicts of interest in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kamel, M.S., Khosa, A., Tawse-Smith, A. et al. The use of laser therapy for dental implant surface decontamination: a narrative review of in vitro studies. Lasers Med Sci 29, 1977–1985 (2014). https://doi.org/10.1007/s10103-013-1396-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-013-1396-0