
Abstract
The purpose of this in vitro investigation was to compare in primary molars, the validity of DIAGNOdent™ 2095 on occlusal caries diagnosis used either separately or in combination with direct and/or indirect visual examinations, based on histological examination as the reference method. In 24 extracted primary molars, 111 occlusal pits were examined for caries by one trained operator (intra-examiner reliability k > 0.80), using the following examination methods: direct visual (DV), indirect visual (IDV), radiographic (XR), and fluorescence (DD) with the DIAGNOdent™. The extent of caries was then determined histologically. Sensitivity, specificity, accuracy, and the area under the ROC curve (AUC) were calculated for each method separately as well as for the combination of DD with DV and/or IDV. The DD accuracy was found both for lesions into enamel and into dentin to be 0.70 while the accuracy of the DD combination with DV and IDV was found to be 0.89. The DD AUC for lesions into enamel and into dentin, 0.68, were not statistically significant different from the other methods (p > 0.5), however the AUC of the combination of DD with DV and IDV, found to be 0.82, was higher than all the other methods, and this was statistically significant for enamel lesions. The validity of DIAGNOdent™ for occlusal caries diagnosis in primary molars was much higher when the DD was used in combination with direct and indirect visual examination, than when used by itself.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
DIAGNOdent™ (KaVo, Bibberach, Germany) [1], is a portable laser fluorescence device used for early occlusal caries diagnosis in which fluorescence alterations of carious dental tissues are expressed as readings on a scale from 0 to 99. It has been proven to be relatively successful for the detection of occlusal caries in permanent teeth both in in vitro and in vivo studies [2–7]. For primary teeth [8–18] more specifically, the DIAGNOdent™ was found to be more sensitive in occlusal caries detection for dentin lesions than for enamel lesions, and when compared to direct visual examination, it was found to have higher sensitivity and lower specificity [10, 13, 18] for caries into dentin but for caries into enamel it was less sensitive and more specific [17]. Thus the DIAGNOdent™ was not found so suitable for detecting early caries lesions.
Despite the great number of reported studies comparing the examination methods individually for occlusal lesions detection, there is a limited number of studies investigating the occlusal caries detecting methods, when combined [19, 20]. A combination of direct visual examination with conventional [20] or digital radiographic examination [19] has been proven successful in improving the validity for detecting occlusal caries in permanent teeth. Regarding the DIAGNOdent™, its combination with visual and radiographic examinations has been recently investigated by three studies, all in ,permanent teeth and has been found successful, especially for enamel caries [21–23]. Two of these studies were in vitro [21, 22] with reference method the histological evaluation and one was in vivo with reference method pit and fissure opening [23]. A common finding of all studies was that the caries diagnostic validity improved when the DIAGNOdent™ was combined with visual and radiographic examinations. The validity of laser fluorescence occlusal caries diagnosis in primary molars differs from that in permanent molars [6], which is attributed mainly to differences in the enamel thickness and structure [24]. The validity of the DIAGNOdent™ combined diagnosis in primary teeth, however, has not been investigated.
Thus, the purpose of this in vitro investigation was to compare in primary molars, the validity of DIAGNOdent™ 2095 on occlusal caries diagnosis, used either separately or in combination with direct and/or indirect visual examinations, based on histological examination as the reference method.
Materials and methods
Sample description
The sample of this study consisted of 24 recently extracted second primary molars, kept in fresh tap water since the day of their extraction. Teeth with occlusal restorations, occlusal fissure sealants, extensive fissure staining, hypoplastic pits, and occlusal caries with cavitation were excluded. The sample teeth yielded a total of 111 examination sites, occlusally located.
Study design
Occlusal sites were evaluated by one examiner for caries detection and scoring using direct visual (DV), indirect visual (IDV), radiographic (XR), and laser fluorescence examinations with the DIAGNOdent™ (DD). The extent of caries was based on histological evaluation of the sites, which was the reference method. Caries were detected using examination methods either separately or in combination with DD. The DD was combined with DV and/or IDV examinations.
Examination methods
Direct visual examination (DV)
For the DV examination, all occlusal surfaces of the sample teeth were cleaned with a toothbrush and pumice-free toothpaste, as previously published [15–18]. All sites were then evaluated for caries under a dental operating light and classified into three categories (0 = sound, 1 = caries in enamel, 2 = caries in dentin), using the criteria proposed by Νytun et al. [25] and the DIAGNOdent manufacturer [1] (Table 1).
Indirect visual examination (IDV)
For the IDV, all occlusal surfaces were photographed with a digital camera (Coolpix 990/ Nikon Corporation, Japan) using a 2x magnification and viewed on a computer screen at a magnification of 5x (final magnification 10x). These photographs were used to map the examination sites and to evaluate them for caries with IDV examination using the same criteria as for the DV examination (Table 1).
Radiographic examination (XR)
Bitewing radiographs (Kodak Insight, Carestream Health Inc., Rochester, NY) were taken for all teeth using the Endo Ray film holder and were developed in a Durr X-Ray Film Processor - XR 04 (Durr Dental GmbH & Co. KG, Bissinger, Germany) to ensure standardized conditions. All radiographs were viewed on a light box with a 2x magnifying lens and evaluated according to the criteria presented in Table 1.
DIAGNOdent readings (DD)
For the fluorescence examination of the study sites, the DIAGNOdent 2095 device was used with tip A, according to the manufacturer's instructions by calibrating it on every single tooth and as previously suggested [15].
In order to be able to compare DD findings with histological examination, the original DD readings were converted from its 0–99 scale to the 0, 1, and 2 scoring scale, applied for all other methods. DD estimation of cut-off points for enamel or dentin involvement was based on the best inter-method agreement between the converted DD readings to the histological findings, using Cohen’s kappa coefficient, as presented in Fig. 1. The kappa coefficient took its highest value when DD readings were 3 for enamel and 40 for dentin lesions and these are the cut-offs used in this study.

Kappa statistic values for the agreement of HIS and modified DD scale at different cut-offs for enamel (lines) and dentin (X-axis) scores
Combined examination (CE)
The reference method to test the validity of the DD combined diagnosis with DV and/or IDV examinations was histological examination, as was also for all other examination methods.
The diagnostic decision for the combined evaluation was based on the best agreement of the combined methods with the histological examination. The caries score was decided mostly based on the visual examination score, as shown in Table 2. A score of 0 was given to the site when all three examination methods indicated 0; a score of 1 was given to the site if any of the three examinations indicated 1 or one indicated 0 and the others 1; a score of 2 was given to the site when the DD indicated 1 and both visual examination methods 2 or when the DD and any of the other two methods indicated 2.
Histological examination (HIS)
Suitable specimens for histological evaluation were produced, as previously published [18]. The grounded surfaces were then evaluated under the microscope (Leitz Elvar, Esselte Leitz GmbH & Co KG, Stuttgart, Germany) at a magnification of 12.5x and photographed using a digital camera (Coolpix 990, Nikon Corporation, Japan). The evaluation of the carious lesion was assessed according to the extent of the demineralization zone (rough or colored) into the enamel or dentin and all examination sites were classified with the same three-grade caries-scoring scale applied to all previously used methods (Table 1).
Examiner’s calibration and reliability
Examiner’s calibration was based on repeated blind evaluations of occlusal sites in primary molars according to Table 1 criteria. Intra-examiner reliability was evaluated using Cohen’s kappa statistics by having the examiner classify blindly three times, 18 randomly selected occlusal sites, photographs, radiographs, and histological sections as seen in Table 3.
Statistical analysis
Validation of each diagnostic method and the combination of DD with DV or/and IDV was based on comparison of their sensitivity, specificity, and accuracy using histological examination as the reference method. Receiver operating characteristics curves (ROC) were plotted and the area under the curve (AUC) was estimated using MedCalc v.9.0.1.1 statistical package (MedCalc Software, Mariakerke, Belgium). Significant differences between examination methods and DD combinations were estimated by pairwise comparisons using also MedCalc v.9.0.1.1, at a 0.05 level of significance (Table 3).
Results
Sample distribution
Table 4 presents the disease level of the 111 evaluated examination sites, for each examination method separately and for the DD combination with DV and/or IDV.
Validity of the examination methods
Sensitivity, specificity, and accuracy of the examination methods and their combination were based on histological evaluation as the reference method and results are presented in Table 5 separately for enamel and dentin caries.
Validating each method separately, the DD for enamel caries exhibited the highest sensitivity as also the IDV (0.87) and the highest specificity (0.38) for dentin caries. However, the DD examination had the lowest sensitivity, 0.39. Accuracy for enamel caries (0.70) was almost identical as for dentin caries (0.71).
Validating the DD in combination with the visual methods DV and/or IDV improved the diagnostic accuracy both for enamel and dentin lesions. The highest accuracy, 0.89, was found when all three methods DD + DV + IDV were combined both for enamel and dentin lesions, Table 5.

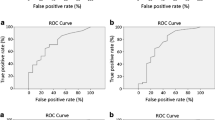
ROC curves of the diagnostic methods separately or in combination for lesions into enamel
ROC curves and AUC
Relevant receiver operating curves (ROC) curves for the above examination methods and their combinations are presented in Fig. 2 for enamel lesions and Fig. 3 for lesions into dentin, while their AUC values along with their significant differences are shown in Table 6. Among the individual examination methods used, the DD had the highest AUC for enamel lesions while for dentin lesions the IDV.

ROC curves of the diagnostic methods separately or in combination for lesions into dentin
Among the combined methods, the highest AUC was found for the combination DD with DV and IDV, both for enamel (0.836) and for dentin lesions (0.825) and this was statistically significant different from the other methods only for enamel caries (p < 0.05). The smallest AUC was found for the radiographic examination.
Discussion
In the present in vitro study in primary molars, the DD device was validated for occlusal caries detection either used separately or in combination with visual examination methods having histological examination as the reference method. When only the DD was used, no statistical significance was found with the other methods either in detecting enamel or dentin lesions. However, when used in combination with both visual examinations DV and IDV, the highest accuracy was achieved, and this was statistically significant different only for enamel lesions.
In order to estimate the DD sensitivity, specificity, and accuracy, the DD values were converted into the same three grade caries scale as used for visual, radiographic, or histological examination, as previously [8, 11, 13, 26]. This new scale highly correlated with the original values.
DD cut-off limits used in this study for enamel caries were similar to the values used in previous in-vitro studies, in which histological examination was also used as the reference method [8, 9, 12, 14]. DD cut-offs for caries into dentin limits, however, were much higher than those used previously in primary teeth in-vitro [9–11, 15]. This may be attributed to the different cut-off estimation statistical methods applied, Cronbach previously [18], Cohens Kappa currently. It may be also attributed to differences in the distribution of enamel or dentin lesions in the sample, in the storage medium, pit remnants, and drying time before each measurement [27]. These all need more attention in future research. The cut-off limits estimation method chosen in this study, Cohen’s kappa statistics, was used to compare the agreement of the two ordered scales in different cut-offs for enamel and dentin levels, as previously reported [27]. This method allowed the measurements of the device to be expressed in values closer to the findings from the histological examination [8, 11, 13, 26].
In the present study, when validating the examination methods separately, the highest sensitivity, specificity, and accuracy for lesions into enamel was found with the DD, as previously found in primary teeth, in vitro [8–18]. However, for lesions into dentin, the IDV was found to have the highest accuracy as previously in vitro [18]. Comparing IDV to DV, the IDV showed higher accuracy both for enamel and dentin lesions, suggesting that the use of an intraoral digital camera may be a useful clinical adjunct in the clinic for primary teeth early caries diagnosis.
According to the principles of DD operation, DD measures fluorescence changes occurring in the organic matrix of carious lesions [31] rather than measuring adequately mineral changes [13], thus the device is considered and has been found [6, 16] more sensitive for dentin than for enamel lesions. Results of the present study, however, have found the DD to have higher sensitivity for enamel lesions while higher specificity for dentin lesions as also indicated by others for primary [28] as well as for permanent teeth [29, 30]. A possible explanation for these controversial findings is that although the DD readings are not correlated with mineral changes, the DD may detect small initial demineralization changes in the enamel lesion subsurface, like the microporosities that are filled with organic material, enhancing the emitted fluorescence. If a significant number of such initial lesions exist in the sample as in the present study, then this would result in higher sensitivity for enamel lesions.
Validation of the DD in combination with visual examination methods DV and IDV was presently investigated since it simulates diagnostic decisions taken by the clinicians in the everyday clinical practice when using the DD as an adjunct to visual examination. Such combination proved previously to be successful in permanent teeth [21, 22], however, has not been validated in primary teeth. Results of the present study found this combination to greatly improve the accuracy for occlusal caries diagnosis as measures of validity suggested. The highest diagnostic accuracy (0.89) was obtained when both visual methods, DV and IDV were used, suggesting the importance of using all three methods in the clinical setting. The validity of the combined examination methods may be influenced by the diagnostic decision taken when evaluating a site, considering all three methods. In previous studies this combination of diagnostic methods [19–23] was investigated, but it has not been clarified how these decisions were taken. So this area needs further research in order to apply the combined examination methods in the everyday clinical practice.
Radiographic examination was found to have a very low accuracy for enamel caries, as already previously reported [9], while its high sensitivity for dentin lesions is misleading since it comes from studying only one observation, that determined histologically. Thus, XR was not combined in the present study with the DD or the visual examination. Results of a previous study in permanent molars have shown higher validity when the DD was combined with the DV than when combined with radiographic examination [21]. Furthermore, results from another study [22] showed that direct visual examination and the DD complemented each other, correcting each other’s false-positive or false-negative decisions.
In conclusion, the findings of the present study suggest that the DD device is a useful adjunct tool to visual clinical examination for early occlusal caries detection in primary molars. Its high sensitivity for enamel lesion makes the device more useful for the detection of early caries in primary teeth, especially if it is combined with direct and/or indirect visual examination due to their higher specificity. For more advanced lesions into dentin, the DD device is as useful as the other methods, but due to its low sensitivity and high specificity, it must be combined with the visual examination methods DV and/or IDV, which presented the best sensitivity for dentin lesions. Such combined examination also needs to be tested in-vivo in order for clinicians to achieve the best possible diagnosis in clinical situations.
The DD device can be used for the detection of enamel and dentin caries in primary molars but for optimum validity, it must be combined with visual examinations, especially if an operative intervention is to be decided.
Conclusions
-
1.
The DD when used individually was not found to be statistically significantly different than the other methods in primary molar occlusal caries diagnosis.
-
2.
The combination of DD with the visual methods improved the accuracy in occlusal caries diagnosis.
-
3.
The DD when used in combination with visual examinations direct and/or indirect was found to be statistically significantly different from the other methods only for enamel lesions.
References
KaVo (2002) Clinical Guidelines Biberach : KaVo, German Issue II
Lussi A, Hibst R, Paulus R (2004) DIAGNOdent: an optical method for caries detection. J Dent Res 83 Spec No C:C80–83
Burin C, Burin C, Longuercio AD, Grande RH, Reis A (2005) Occlusal caries detection: a comparison of a laser fluorescence system and conventional methods. Pediatr Dent 27(4):307–312
Reis A, Mendes FM, Angnes V, Angnes G, Grande RH, Longuercio AD (2006) Performance of methods of occlusal caries detection in permanent teeth under clinical and laboratory conditions. J Dent 34(2):89–96
Olmez A, Tuna D, Oznurban F (2006) Clinical evaluation of DIAGNOdent in detection of occlusal caries in children. J Clin Pediatr Dent 30(4):287–291
Bader JD, Shugars DA (2004) A systematic review of the performance of a laser fluorescence device for detecting caries. J Am Dent Assoc 135(14):1413–1426
Ricketts D (2005) The eyes have it. How good is DIAGNOdent at detecting caries? J Am Dent Assoc 135(10):1413–1426
Attrill DC, Ashley PF (2001) Occlusal caries detection in primary teeth: a comparison of DIAGNOdent with conventional methods. Br Dent J 190(8):440–443
Rocha RO, Ardenghi TM, Oliveira LB, Rodrigues CRMD, Ciamponi AL (2003) In vivo effectiveness of laser fluorescence compared to visual inspection and radiography for the detection of occlusal caries in primary teeth. Caries Res 37(6):437–441
Antonnen V, Seppa L, Hausen H (2003) Clinical study of the use of the laser fluorescence device DIAGNOdent for the detection of occlusal caries in children. Caries Res 37(1):17–23
Lussi A, Francescut P (2003) Performance of conventional and new methods for the detection of occlusal caries in deciduous teeth. Caries Res 37(1):2–7
Bengtson AL, Gomes AC, Mendes FM, Cichello LR, Bengtson NG, Pinheiro SL (2005) Influence of examiner’s clinical experience in detecting occlusal caries lesions in primary teeth. Pediatr Dent 27(3):238–243
Mendes FM, Ganzerla E, Nunes AF, Puig AV, Imparato JC (2006) Use of high-powered magnification to detect occlusal caries in primary teeth. Am J Dent 19(1):19–22
Costa AM, Bezzera ACB, Fuks AB (2007) Assessment of the accuracy of visual examination, bite-wing radiographs and DIAGNOdent on the diagnosis of occlusal caries. Eur Arch Paediatr Dent 8(2):118–122
Kavvadia K, Lagouvardos P (2008) Clinical performance of DIAGNOdent for the detection of occlusal caries in primary teeth. Int J Paediatr Dent 18(3):197–204
Braga M, Nicolau J, Rodrigues CR, Imparato JC, Mendes FM (2008) Laser fluorescence device does not perform well in detection of early caries lesions in primary teeth: an in vitro study. Oral Health Prev Dent 6(2):165–169
Rodrigues J, Diniz M, Josgrillberg CR (2009) In vitro comparison of laser fluorescence performance with visual examination for detection of occlusal caries in permanent and primary molars. Lasers Med Sci 24(4):501–6
Apostolopoulou D, Lagouvardos P, Kavvadia K, Papagiannoulis L (2009) Histological validation of a laser fluorescence device for occlusal caries detection in primary molars. Eur Arch Paediatr Dent 10(Suppl 1):11–15
Wenzel A, Fejerskov O (1992) Validity of diagnosis of questionable caries lesions in occlusal surfaces of extracted third molars. Caries Res 26(3):188–194
Ketley CE, Holt RD (1993) Visual and radiographic diagnosis of occlusal caries in first permanent molars. Br Dent J 174:364–370
Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG (2006) Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res 40(3):194–201
Valera FB, Pessan JP, Valera RC, Mondelli J, Percinoto C (2008) Comparison of visual inspection radiographic examination laser fluorescence and their combinations on treatment decisions for occlusal surfaces. Am J Dent 21(1):25–29
Chu CH, Lo CM, You DSH (2010) Clinical diagnosis of fissure caries with conventional and laser-induced fluorescence techniques. Lasers Med Sci 25:355–362
De Menezes Oliveira MA, Torres CP, Gomes-Silva JM, Chinelatti MA, De Menezes FC, Palma-Dibb RG, Borsatto MC (2010) Microstructure and mineral composition of dental enamel of permanent and deciduous teeth. Microsc Res Tech 73(5):572–7
Nytun RB, Raadal M, Espelid I (1992) Diagnosis of dentin involvement in occlusal caries based on visual and radiographic examination of the teeth. Scand J Dent Res 100(3):144–148
Francescut P, Lussi A (2003) Correlation between fissure discoloration, DIAGNOdent measurements and caries depth: an in vitro study. Pediatr Dent 25(6):559–564
Heinrich-Weltzien Kuhnisch J, Oehme T, Zieche A, Stosser L, Garcia-Godoy F (2003) Comparison of different DIAGNOdent cut-off limits for in vivo detection of occlusal caries. Oper Dent 28(6):672–680
Mendes FM, Siqueira WL, Mazzitelli JF, Pinheiro SL, Bengtson AL (2005) Performance for detection and quantification of smooth-surface caries in primary teeth. J Dent 33(1):79–84
Huth KC, Neuhaus KW, Gyrax M, Bucher K, Crispin A, Paschos E, Hickel R, Lussi A (2008) Clinical performance of a new laser fluorescence device for the detection of occlusal caries in permanent molars. J Dent 36(12):1033–1040
Plasschaert Alwas-Danowska HM, Suliborski AJ, Verdonschot EH S (2002) Reliability and validity issues of laser fluorescence measurements in occlusal caries diagnosis. J Dent 30(4):129–134
Shi X-Q, Walander U, Angmar-Mansson B (2000) Occlusal caries detection with KaVo DIAGNOdent and radiographic examination: an in vitro comparison. Caries Res 34(2):151–158
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kavvadia, K., Lagouvardos, P. & Apostolopoulou, D. Combined validity of DIAGNOdent™ and visual examination for in vitro detection of occlusal caries in primary molars. Lasers Med Sci 27, 313–319 (2012). https://doi.org/10.1007/s10103-010-0877-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-010-0877-7