
Abstract
Recent reports have showed that a proportion of patients with Coronavirus Disease 2019 (COVID-19) presented elevated leukocyte count. Clinical data about these patients is scarce. We aimed to evaluate the clinical findings of patients with COVID-19 who have increased leukocyte at admission. We retrospectively collected the clinical data on the 52 patients who have increased leukocyte count at admission from the 619 patients with confirmed COVID-19 who had pneumonia with abnormal features on chest CT scan in Renmin Hospital of Wuhan University in Wuhan, China, from February 3 to March 3, 2020. The mean age of the 52 patients with increased leukocyte count was 64.7 (SD 11.4) years, 32 (61.5%) were men and 47 (90.4%) had fever. Compared with the patients with non-increased leukocyte count, the patients with increased leukocyte count were significantly older (P < 0.01), were more likely to have underlying chronic diseases (P < 0.01), more likely to develop critically illness (P < 0.01), more likely to admit to an ICU (P < 0.01), more likely to receive mechanical ventilation (P < 0.01), had higher rate of death (P < 0.01) and the blood levels of neutrophil count and the serum concentrations of CRP and IL-6 were significantly increased, (P < 0.01). The older patients with COVID-19 who had underlying chronic disorders are more likely to develop leukocytosis. These patients are more likely to develop critical illness, with a high admission to an ICU and a high mortality rate.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Since December 2019, an outbreak of coronavirus disease 2019 (COVID-19), previously described as novel coronavirus (2019-nCoV)-infected pneumonia (NCIP) [1, 2], occurred in Wuhan, China [2]. COVID-19 is an acute resolved disorder but also lethal, with a 2% case mortality rate. Some studies have reported that the severity of some cases of COVID-19 mimicked that of severe acute respiratory syndrome (SARS) [2,3,4]. Thus, the World Health Organization (WHO) has declared the outbreak of COVID-19 a public health emergency of international concern [5].
The initial diagnosis for suspected COVID-19 was on the basis of the SARS and Middle East respiratory syndrome (MERS) case diagnosis, as recommended by the WHO in 2003 and 2012, respectively [6,7,8]. During the initial phase of the COVID-19 outbreak, the diagnosis of the disease was complicated by the diversity in symptoms and imaging findings and in the severity of disease at the time of presentation. Currently, normal or low white blood cell count or low lymphocyte count is one of the diagnostic criteria for a suspected COVID-19 case. However, recent reports have showed that a proportion of patients with COVID-19 presented elevated white blood cell count in peripheral blood [3, 9]. Previous studies have reported the general epidemiological findings, clinical features and clinical outcomes of patients with COVID-19 [2,3,4]. However, specific information about patients with COVID-19 who have elevated leukocyte count remains unclear. Given no effective treatments or vaccines for COVID-19, the information on the clinical characteristics and outcomes of these cases might help understand the pathogenesis of the disease and improve clinical protocols against COVID-19. In this study, we describe the clinical characteristics in 52 hospitalized patients with COVID-19 who have elevated leukocyte count and compare them with patients who have no elevated leukocyte count in peripheral blood.
Methods
Study design and participants
In this retrospective, singlecentre study, all consecutive patients with confirmed COVID-19 admitted to Renmin Hospital of Wuhan University (Wuhan, China) from February 3 to March 3, 2020, were recruited. According to the assignments the Chinese Government, Renmin Hospital of Wuhan University is responsible for the treatments of adult patients with confirmed COVID-19 from the whole of Wuhan City. All patients with confirmed COVID-19 recruited in this study were diagnosed on the basis of WHO interim guidance [10]. Other respiratory viruses including influenza A virus (H1N1, H3N2, H7N9), influenza B virus, respiratory syncytial virus, parainfluenza virus and adenovirus were also examined with real-time reverse transcriptase polymerase chain reaction (RT-PCR). Sputum or endotracheal aspirates were obtained at admission for identification of possible causative bacteria, tuberculosis or fungi. The patients with coinfections such as other viruses, bacteria, tuberculosis and fungi were excluded. Additionally, the patients who received systemic corticosteroids and antibiotics for treatment before admission were ineligible. Critically ill patients were identified as those admitted to the intensive care unit (ICU) who needed mechanical ventilation or required a fraction of inspired oxygen (FiO2) of at least 60% or more [11,12,13]. According to complete blood cell count at the time of admission, the patients with confirmed COVID-19 whose leukocyte count was more than 11,000 per mm3 were defined as the patient with increased leukocyte count, as previously reported [14,15,16], and other patients with confirmed COVID-19 whose leukocyte count was less than or equal to 11,000 per mm3 were defined as the patient with non-increased leukocyte count. Acute respiratory distress syndrome (ARDS) and shock were defined according to WHO interim guidance [10]. Acute kidney injury was identified according to the Kidney Disease: Improving Global Outcomes definition [17]. Secondary infection was diagnosed according to Center for Disease Control (CDC) definitions for nosocomial infections in 1988 [18]. Systemic inflammatory response syndrome (SIRS) manifested by at least two of the following: (a) body temperature over 38 or under 36 degrees Celsius, (b) heart rate greater than 90 beats/min, (c) respiratory rate greater than 20 breaths/min or partial pressure of CO2 less than 32 mmHg or (d) leucocyte count greater than 12,000 or less than 4000/microliters or over 10% immature forms or bands [19, 20]. The study was approved by Renmin Hospital of Wuhan University Ethics Committee (No. WDRY2020-K143), and written informed consent was waived by the Ethics Commission.
Data collection
Demographic data, exposure history, clinical symptoms or signs, chronic medical histories and laboratory findings at admission, treatment and clinical outcomes were collected from electronic medical records. All data were checked by two physicians. A patient of confirmed COVID-19 was defined as at least two positive results on the basis of RT-PCR assay of pharyngeal and nasal swab samples. Laboratory confirmation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was performed in Renmin Hospital of Wuhan University, a certified tertiary care hospital. RT-PCR measurements were performed according to a standard procedure recommended by Hubei Provincial CDC. Only laboratory-confirmed patients were enrolled to further analyse. Laboratory findings at admission included a complete blood cell count, blood biochemical analysis (including liver and renal function, lactate dehydrogenase), coagulation function testing and C-reactive protein (CRP), procalcitonin, arterial blood gas analysis and plasma cytokines such as IL-6. Additionally, all patients were given chest computed tomography (CT), and chest CT findings were reviewed by two physicians who extracted the data.
Clinical outcomes
The primary endpoints were the incidence of critically ill case, the incidence of SIRS and the complications (development of organ function damage). The secondary endpoints were the rate of admission to an ICU, and the rate of death. Clinical outcomes were followed up till March 22, 2020.
Statistical analysis
We present continuous measurements as mean (SD) if they are normally distributed or median (IQR) if they are not, and categorical variables as count (%). For laboratory results, we also assessed whether the measurements were outside the normal range. Independent group t tests were used for the comparison of means for continuous variables that were normally distributed; conversely, the Mann-Whitney U test was used for continuous variables not normally distributed. Proportions for categorical variables were compared using the χ2 test or Fisher’s exact test. Two-sided P values of less than 0.05 were considered statistically significant. We used SPSS (version 26.0) for all analyses.
Results
Demographic data and clinical characteristics
As of Mar 3, 2020, a total of 619 patients with confirmed COVID-19 were enrolled. All patients had pneumonia with abnormal findings on chest CT scan. The patients with confirmed COVID were categorized as elevated leukocyte count in 52 patients, and non-increased leukocyte count in 567 patients (52 (8.4%) patients showed elevated leukocyte count) according to complete blood cell count at the time of admission. The demographic data and clinical characteristics of all patients were outlined in Table 1 and Table 2. All patients were residents of Wuhan City. One hundred sixty-three (26.3%) had exposure to patients who had fever or respiratory symptoms. However, the exposure history between the two groups was similar. Compared with patients who had non-increased leukocyte count, patients who showed increased leukocyte count were significantly older (mean age, 64.7 years [SD, 11.4] vs 57.6 years [SD, 13.0]; P < 0.01) and were more likely to have underlying comorbidities (37 [71.2%] patients and 260 [45.9%] patients, respectively; P < 0.01), including hypertension (26 [50%] vs 139 [24.5%], diabetes (13 [25.0%] vs 72 [12.7%]), coronary heart disease (8 [15.4%] vs 37 [6.5%]) and cerebrovascular disease (2 [3.8%] vs 17 [3.0%]). The presence of fever was more common in patients with increased leukocyte count than those with non-increased leukocyte count at onset of illness (47 [90.4%] vs 425 [75.0%], P < 0.05]). Heart rate, respiratory rate and systolic pressure were significantly higher in patients with increased leukocyte count than those with non-increased leukocyte count on day of hospital admission (92 [IQR, 82–107.5], 23 [IQR, 20–26], 137.4 [SD, 20.6] and 80 [IQR, 76–89], 20 [IQR, 19–22], 125.6 [SD, 12.7] respectively; P < 0.01).
Radiologic and laboratory findings
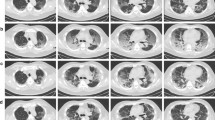
The radiologic and laboratory findings of all patients were shown in Table 3. All patients had unilateral or bilateral infiltrates on chest CT scan. However, radiologic findings did not differ between patients with increased leukocyte count and those with non-increased leukocyte count at the time of admission. Patients with increased leukocyte count had significantly prominent laboratory abnormalities than those with on-increased leukocyte count at admission. The blood levels of leukocyte count and neutrophil count, the serum concentrations of CRP and IL-6 were significantly increased in the patients with increased leukocyte count, compared with the patients with non-increased leukocyte count (11.96 [IQR, 11.39–13.15], 10.58 [IQR, 9.58–12.22], 78.7 [IQR, 46.3–153.3], 22.15 [IQR, 11.94–67.79] and 4.84 [IQR, 3.85–5.74], 3.18 [IQR, 2.35–4.15], 29.2 [IQR, 5.0–64.4] 8.40 [IQR, 3.60–17.2], respectively; P < 0.01). Interestingly, the blood levels of leukocyte count and neutrophil count and the serum concentrations of CRP and IL-6 were significantly increased in the patients with increased leukocyte count who have underlying chronic diseases, compared with the patients with increased leukocyte count who have no underlying chronic diseases (12.30 [IQR, 11.79–14.73], 10.86 [IQR, 9.92–13.31], 91.4 [IQR, 50.6–186.7], 35.40 [IQR, 15.94–83.00] and 11.40 [IQR, 11.22–12.54], 9.99 [IQR, 8.51–10.67], 45.1 [IQR, 6.8–107.7], 14.27 [IQR, 8.00–28.41], respectively; P < 0.05) (Table 4).
Treatment
All patients were treated in an isolation ward. The treatments of all patients were outlined in Table 2. The use of antiviral treatment did not differ between patients with increased leukocyte count and those with non-increased leukocyte count at data cutoff. The administration of antibiotic therapy and systemic glucocorticoids was a higher percentage among patients with increased leukocyte count than those with non-increased leukocyte count (45 [86.5%], 31 [59.6%] and 396 [69.8%], 188 [33.2%], respectively; P < 0.05). Oxygen therapy was administered in more patients with increased leukocyte count than in those with non-increased leukocyte count at data cutoff (51 [98.1%] and 287 [50.6%], respectively; P < 0.01). Compared with patients with non-increased leukocyte count, patients with increased leukocyte count were more likely to receive mechanical ventilation, either invasively or noninvasively (9 [17.3%] vs 6 [1.1%] and 12 [23.1%] vs 56 [9.9%], respectively; P < 0.01). Extracorporeal membrane oxygenation was performed in 2 patients (3.8%) with increased leukocyte count and in 1 patient (0.2%) with non-increased leukocyte count.
Clinical outcomes
The clinical outcomes of all patients were outlined in Table 5. Compared with the patients with non-increased leukocyte count, the patients with increased leukocyte count were more likely to develop critically illness (26 [50.0%] patients and 74 [13.1%] patients, respectively; P < 0.01), more likely to develop organ function damage(38 [73.1%] patients and 99 [17.5%] patients, respectively; P < 0.01), especially ARDS (24 [46.2%] patients and 59 [10.4%] patients, respectively; P < 0.01), more likely to admitted to an ICU (24 [46.2%] patients and 67 [11.8%] patients, respectively; P < 0.01) and had a higher mortality rate (10 [19.2%] patients and 33 [5.8%] patients, respectively; P < 0.01) at data cutoff. By the end of March 22, 451 (72.9%) patients had been discharged and 125 (20.2%) patients were still in hospital. Additionally, compared with the patients with non-increased leukocyte count, the patients with increased leukocyte count were more likely to develop SIRS (35 [67.3%] patients and 99 [17.5%] patients, respectively; P < 0.01).
Discussion
The initial diagnostic criteria for suspected COVID-19 focused more on normal or low white blood cell count or low lymphocyte count of patients’ peripheral blood [9]. In this study, our data showed that lymphopenia was the most common laboratory abnormal finding in a cohort of 619 patients with confirmed COVID-19 who had pneumonia with abnormal features on chest CT scan, as previously reported [2,3,4]. However, 52 of 619 patients had increased leukocyte count at the time of admission in this study. Meanwhile, we found that the patients with increased leukocyte count were significantly older, and were more likely to have fever and underlying chronic diseases, thereby suggesting that the older patients with COVID-19 who had underlying chronic disorders are more likely to develop leukocytosis.
Studies of its effect on some body systems are important to the understanding of COVID-19. It is well known that SIRS is the systemic inflammatory response to a variety of severe clinical insults. Infection including virus infection is an important inducer of systemic inflammatory response [19, 20]. In this study, our data showed that the confirmed COVID-19 patients with increased leukocyte count were more likely to develop SIRS. Procalcitonin, IL-6 and CRP can be released in the acute phase of SIRS, as common biomarkers of SIRS [20,21,22]. Procalcitonin levels can mildly elevate in viral infection and significantly elevate in bacterial, fungal or parasitic infections [20]. Both IL-6 and CRP are useful in predicting the severity and outcomes of SIRS [22,23,24]. Our present data indicated that the confirmed COVID-19 patients with increased leukocyte count exhibited increased concentrations of procalcitonin, CRP and IL-6 in the serum when compared with the patients with non-increased leukocyte count. Thus, our results suggested that the confirmed COVID-19 patients with increased leukocyte count had significantly higher level of systemic inflammation response, which at least partially related to the development of critical illness, with a high admission to an ICU and a high mortality rate. Interestingly, we found the blood levels of leukocyte count and neutrophil count, the serum concentrations of CRP and IL-6 were significantly increased in the patients with increased leukocyte count who have underlying chronic diseases, compared with the patients with increased leukocyte count who have no underlying chronic diseases. Therefore, our findings suggested that the systemic inflammatory response in the confirmed COVID-19 patients who had comorbidities was significantly higher than the patients who have no comorbidities. A growing body of evidences has suggested that chronic low-grade systemic inflammation was found in patients with underlying chronic diseases, such as diabetes [25], cancer [26] and metabolic syndrome (including hypertension) [27]. Therefore, we speculated that the chronic low-grade systemic inflammation in confirmed COVID-19 patients who have underlying chronic diseases could promote systemic inflammatory response when SARS-CoV-2 infected.
In this study, our results showed that the confirmed COVID-19 patients with increased leukocyte count had a higher number of neutrophils in peripheral blood. As we discussed, the confirmed COVID-19 patients with leukocytosis had a higher level of systemic inflammatory response and IL-6 in the serum as comparison with the patients with non-increased leukocyte count. It has been reported that IL-6 can promote Th17 cells differentiation from naïve CD4 T cells [28,29,30], and Th17 cells can induce an inflammatory response through the production of IL-17A and IL-17F [31], which act as key cytokines for neutrophils migration, recruitment and activation [32, 33]. It has been reported that phagocytosis, release of granular contents and production of cytokines are major effector functions of activated neutrophils, suggesting a protective immune response against the virus [34]. However, excessive increased neutrophils can cause cytokine storm and tissue damage, leading to severe pneumonia and death [34], which had been observed in patients with SARS [35, 36] and MERS [37]. Therefore, it is possible that neutrophilia at least partially related to the development of critical illness, with a high admission to an ICU and a high mortality rate in the confirmed COVID-19 patients with increased leukocyte count. However, future studies to evaluate the mechanisms of these features may help us to understand this disorder.
In view of high level of inflammation-associated biomarkers, including neutrophil count and CRP in SARS-nCoV-2 infection, systemic glucocorticoids and antibiotics were frequently administrated for treatment of patients with COVID-19 in this study. However, our results showed that the confirmed COVID-19 patients with increased leukocyte count receiving antibiotics still had a considerable number of critical illness, with a high admission to an ICU and a high mortality rate. Therefore, antibiotic therapy and systemic glucocorticoids should not be routinely given for the confirmed COVID-19 patients with increased leucocyte count.
This study had several limitations, which might make some potential biases. First, it was a retrospective, single centre study and the sample size of confirmed COVID-19 patients with increased leukocyte count is small. It would be better for a multi-centre study including more patients to get a more comprehensive understanding of COVID-19. Second, among the 619 cases, 125 patients were still in hospital and the outcomes were unknown at data cutoff. Therefore, continued observations of the patients are needed. Third, some patients were given drug treatment before admission, which might affect laboratory findings. Despite that, our study demonstrated several novel clinical features in confirmed COVID-19 patients with increased leukocyte count.
In conclusion, leukocytosis is more likely to be observed in the older patients with COVID-19 who had underlying chronic disorders, and possibly result in critical illness, with a high admission to an ICU and a high mortality rate. Therefore, these patients need more intensive attention in the clinical practice.
Availability of data and material
The datasets analysed during the study are available from the corresponding author on reasonable request.
References
Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, Hu Y, Tao ZW, Tian JH, Pei YY, Yuan ML, Zhang YL, Dai FH, Liu Y, Wang QM, Zheng JJ, Xu L, Holmes EC, Zhang YZ (2020) A new coronavirus associated with human respiratory disease in China. Nature 579(7798):265–269. https://doi.org/10.1038/s41586-020-2008-3
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet (London, England) 395(10223):497–506. https://doi.org/10.1016/s0140-6736(20)30183-5
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet (London, England) 395(10223):507–513. https://doi.org/10.1016/s0140-6736(20)30211-7
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. Jama 323(11):1061–1069. https://doi.org/10.1001/jama.2020.1585
WHO (2020) Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov). Accessed 1 April 2020
WHO (2017) Middle East respiratory syndrome coronavirus: case definition for reporting to WHO. http://www.who.int/csr/disease/coronavirus_infections/case_definition/en/. Accessed 1 April 2020
WHO (2004) WHO guidelines for the global surveillance of severe acute respiratory syndrome (SARS): updated recommendations. Global Alert Response. doi:/entity/csr/resources/publications/ WHO_CDS_CSR_ARO_2004_1/en/ind
Azhar EI, El-Kafrawy SA, Farraj SA, Hassan AM, Al-Saeed MS, Hashem AM, Madani TA (2014) Evidence for camel-to-human transmission of MERS coronavirus. N Engl J Med 370(26):2499–2505. https://doi.org/10.1056/NEJMoa1401505
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382(18):1708–1720. https://doi.org/10.1056/NEJMoa2002032
WHO (2020) Clinical management of severe acute respiratory infection when novel coronavirus (2019-nCoV) infection is suspected: interim guidance, 28 January 2020. https://extranet.who.int/iris/restricted/handle/10665/330893. Accessed 1 April 2020
Domínguez-Cherit G, Lapinsky SE, Macias AE, Pinto R, Espinosa-Perez L, de la Torre A, Poblano-Morales M, Baltazar-Torres JA, Bautista E, Martinez A, Martinez MA, Rivero E, Valdez R, Ruiz-Palacios G, Hernández M, Stewart TE, Fowler RA (2009) Critically ill patients with 2009 influenza A(H1N1) in Mexico. Jama 302(17):1880–1887. https://doi.org/10.1001/jama.2009.1536
Kumar A, Zarychanski R, Pinto R, Cook DJ, Marshall J, Lacroix J, Stelfox T, Bagshaw S, Choong K, Lamontagne F, Turgeon AF, Lapinsky S, Ahern SP, Smith O, Siddiqui F, Jouvet P, Khwaja K, McIntyre L, Menon K, Hutchison J, Hornstein D, Joffe A, Lauzier F, Singh J, Karachi T, Wiebe K, Olafson K, Ramsey C, Sharma S, Dodek P, Meade M, Hall R, Fowler RA (2009) Critically ill patients with 2009 influenza A(H1N1) infection in Canada. Jama 302(17):1872–1879. https://doi.org/10.1001/jama.2009.1496
Fowler RA, Lapinsky SE, Hallett D, Detsky AS, Sibbald WJ, Slutsky AS, Stewart TE (2003) Critically ill patients with severe acute respiratory syndrome. Jama 290(3):367–373. https://doi.org/10.1001/jama.290.3.367
Riley LK, Rupert J (2015) Evaluation of patients with leukocytosis. Am Fam Physician 92(11):1004–1011
Shapiro MF, Greenfield S (1987) The complete blood count and leukocyte differential count. An approach to their rational application. Ann Intern Med 106(1):65–74. https://doi.org/10.7326/0003-4819-106-1-65
Abramson N, Melton B (2000) Leukocytosis: basics of clinical assessment. Am Fam Physician 62(9):2053–2060
Khwaja A (2012) KDIGO clinical practice guidelines for acute kidney injury. Nephron Clinical Pract 120(4):c179–c184. https://doi.org/10.1159/000339789
(1989) CDC definitions for nosocomial infections. Am J Infect Control 17(1):42–43. https://doi.org/10.1016/s0196-6553(89)80013-6
(1992) American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 20(6):864–874
Chakraborty RK, Burns B (2020) Systemic inflammatory response syndrome. In: StatPearls. StatPearls Publishing LLC, Treasure Island (FL)
Staubli SM, Schäfer J, Rosenthal R, Zeindler J, Oertli D, Nebiker CA (2019) The role of CRP and Pentraxin 3 in the prediction of systemic inflammatory response syndrome and death in acute pancreatitis. Sci Rep 9(1):18340. https://doi.org/10.1038/s41598-019-54910-8
Pepys MB, Hirschfield GM (2003) C-reactive protein: a critical update. J Clin Invest 111(12):1805–1812. https://doi.org/10.1172/jci18921
Mokart D, Merlin M, Sannini A, Brun JP, Delpero JR, Houvenaeghel G, Moutardier V, Blache JL (2005) Procalcitonin, interleukin 6 and systemic inflammatory response syndrome (SIRS): early markers of postoperative sepsis after major surgery. Br J Anaesth 94(6):767–773. https://doi.org/10.1093/bja/aei143
Oda S, Hirasawa H, Shiga H, Nakanishi K, Matsuda K, Nakamua M (2005) Sequential measurement of IL-6 blood levels in patients with systemic inflammatory response syndrome (SIRS)/sepsis. Cytokine 29(4):169–175. https://doi.org/10.1016/j.cyto.2004.10.010
Brooks-Worrell BM, Palmer JP (2019) Setting the stage for islet autoimmunity in type 2 diabetes: obesity-associated chronic systemic inflammation and endoplasmic reticulum (ER) stress. Diabetes Care 42(12):2338–2346. https://doi.org/10.2337/dc19-0475
Singh R, Mishra MK, Aggarwal H (2017) Inflammation, immunity, and cancer. Mediat Inflamm 2017:6027305. https://doi.org/10.1155/2017/6027305
Monteiro R, Azevedo I (2010) Chronic inflammation in obesity and the metabolic syndrome. Mediat Inflamm 2010. https://doi.org/10.1155/2010/289645
McGeachy MJ, Cua DJ (2008) Th17 cell differentiation: the long and winding road. Immunity 28(4):445–453. https://doi.org/10.1016/j.immuni.2008.03.001
Sandquist I, Kolls J (2018) Update on regulation and effector functions of Th17 cells. F1000Res 7:205. https://doi.org/10.12688/f1000research.13020.1
Yosef N, Shalek AK, Gaublomme JT, Jin H, Lee Y, Awasthi A, Wu C, Karwacz K, Xiao S, Jorgolli M, Gennert D, Satija R, Shakya A, Lu DY, Trombetta JJ, Pillai MR, Ratcliffe PJ, Coleman ML, Bix M, Tantin D, Park H, Kuchroo VK, Regev A (2013) Dynamic regulatory network controlling TH17 cell differentiation. Nature 496(7446):461–468. https://doi.org/10.1038/nature11981
Miossec P, Kolls JK (2012) Targeting IL-17 and TH17 cells in chronic inflammation. Nat Rev Drug Discov 11(10):763–776. https://doi.org/10.1038/nrd3794
Deng J, Yu XQ, Wang PH (2019) Inflammasome activation and Th17 responses. Mol Immunol 107:142–164. https://doi.org/10.1016/j.molimm.2018.12.024
Rathore JS, Wang Y (2016) Protective role of Th17 cells in pulmonary infection. Vaccine 34(13):1504–1514. https://doi.org/10.1016/j.vaccine.2016.02.021
Lamichhane PP, Samarasinghe AE (2019) The role of innate leukocytes during influenza virus infection. J Immunol Res 2019:8028725. https://doi.org/10.1155/2019/8028725
Wong CK, Lam CW, Wu AK, Ip WK, Lee NL, Chan IH, Lit LC, Hui DS, Chan MH, Chung SS, Sung JJ (2004) Plasma inflammatory cytokines and chemokines in severe acute respiratory syndrome. Clin Exp Immunol 136(1):95–103. https://doi.org/10.1111/j.1365-2249.2004.02415.x
Wong RS, Wu A, To KF, Lee N, Lam CW, Wong CK, Chan PK, Ng MH, Yu LM, Hui DS, Tam JS, Cheng G, Sung JJ (2003) Haematological manifestations in patients with severe acute respiratory syndrome: retrospective analysis. BMJ (Clinical research ed) 326(7403):1358–1362. https://doi.org/10.1136/bmj.326.7403.1358
Mahallawi WH, Khabour OF, Zhang Q, Makhdoum HM, Suliman BA (2018) MERS-CoV infection in humans is associated with a pro-inflammatory Th1 and Th17 cytokine profile. Cytokine 104:8–13. https://doi.org/10.1016/j.cyto.2018.01.025
Funding
This study was funded by a Key Project of Science and Technology on COVID-19 of Hubei Province (No. 2020FCA002).
Author information
Authors and Affiliations
Contributions
HN and XD contributed to the study conception and design. Data collection were performed by RL, XW, YZ and TW. Statistical analyses were performed by RL and KZ. The first draft of the manuscript was written by HN and KZ. ZZ and SZ were responsible for writing–review and editing. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by Renmin Hospital of Wuhan University Ethics Committee (No. WDRY2020-K143).
Consent to participate
This study was an observational study and written informed consent was waived by the Ethics Commission.
Consent for publication
Not applicable.
Code availability
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhao, K., Li, R., Wu, X. et al. Clinical features in 52 patients with COVID-19 who have increased leukocyte count: a retrospective analysis. Eur J Clin Microbiol Infect Dis 39, 2279–2287 (2020). https://doi.org/10.1007/s10096-020-03976-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-020-03976-8