
Abstract
The investigation of pleural effusion has been greatly assisted by advancements in pleural fluid analysis. In the case of tuberculous pleural effusion, diagnosis traditionally requires the demonstration of acid fast bacilli in the pleural space using microbiological or histological techniques. In recent years, there has been progress in pleural fluid analysis in suspected tuberculous effusions, with particular interest in adenosine deaminase and interferon-γ. These individual tests are quite sensitive and specific; however, data are sparse on the benefits that multiple-parameter testing may have when analysed in combination. We reviewed the literature to investigate the evidence for multiple-parameter testing, both biochemical and clinical, in the evaluation of tuberculous effusion.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tuberculosis (TB) continues to be an important cause of morbidity and mortality in developing countries. Areas of high epidemiologic burden (annual incidence >25/100,000) include South Africa (480/100,000) and Swaziland (1,155/100,000), which contrast with the low burden areas of the United States and Monaco, where the annual incidence is 4.6 and 2/100,000, respectively [1, 2].
Mycobacterium tuberculosis-related pleural effusion results from the infiltration of the pleural space by M. tuberculosis antigens or bacilli. Traditional investigation involves microscopic examination for acid fast bacilli, fluid culture, cytological examination of fluid for inflammatory cells, and microbiological and histological examination of biopsied tissue.
With pleural fluid analysis, acid fast bacilli are detected in <5% of cases, whereas mycobacterial culture of fluid has a sensitivity of <60%, with waiting times of up to 2 months for culture results [3, 4].
Other methods traditionally used for TB lung infection also have disappointing diagnostic ability. The culture of spontaneous or induced sputum has a sensitivity of <30 and 52%, respectively, and approximately one-third of patients with tuberculous pleural effusion have a negative tuberculin skin test [5].
Histological analysis and mycobacterial culture of closed pleural biopsied tissue have traditionally been the gold standard methods of investigation, with sensitivities of 71–80 and 39–79%, respectively [6]. Combining both has a detection rate of 91.3% for TB [7]. The introduction of thoracoscopy has had a very important impact on diagnosis, which was particularly highlighted by Diacon et al. who performed a direct comparative study of the diagnostic tools used in tuberculous pleurisy and found that the sensitivity of histology, culture and combined histology/culture was 66, 48 and 79%, respectively, for closed-needle biopsy and 100, 76 and 100%, respectively, for thoracoscopy. Both were 100% specific [8]. Apart from achieving superior histological samples, the technique of thoracoscopically biopsying large areas of abnormal pleura also increases the likelihood of positive diagnosis, especially when macroscopic abnormalities such as “tapioca pleura” are observed. This macroscopic appearance combined with the microscopic appearance of granulomas often allows the commencement of therapy while culture results are awaited. Thoracoscopy, unlike other forms of pleural biopsy, also facilitates the removal of pleural fluid, thereby, relieving troublesome dyspnoea.
In more recent times, additional pleural fluid biomarkers have been discovered, including adenosine deaminase (ADA), which, reportedly, has a sensitivity of 88% and a specificity of 85.7%, and interferon-γ (IFN-γ), which has a sensitivity of 85.7% and a specificity of 97.1%. These studies were reported from an area where the prevalence was 59 per 100,000 population [6, 9]. A more recent meta-analysis of 63 studies found that ADA has a sensitivity and a specificity of 92 and 90%, respectively, and a meta-analysis of 22 studies found that IFN-γ has a sensitivity and a specificity of 89 and 97%, respectively [10, 11]. Acceptance of these tests for the diagnosis of pleural TB has not been universal and remains contentious in some countries, with their diagnostic performance being very variable between populations [12].
Used individually, the different cheap and easy-to-perform pleural fluid tests have a wide range of sensitivity and specificity. We hypothesised that these tests used in combination might improve the ability to diagnose this condition.
Methods
In this review, we searched for publications describing pleural fluid test combinations that may help with the diagnosis of tuberculous pleural effusion. Publications from a MEDLINE search and references from relevant articles were reviewed on the clinical investigation of tuberculous pleural effusion. All articles that adhered to the criteria of multiple tests or parameter combinations in the diagnosis of tuberculous effusions were included in this review. Papers were separately selected by author 1 (EMG) and author 2 (PA), with common papers included in the review. Papers found by only one author were assessed by both authors together for their suitability. Keywords searched were: tuberculous effusion, pleural fluid, diagnosis, ADA, IFN-γ, pleuritis and empyema
Results
As summarised in Table 1, 12 studies describing the use of combination fluid/clinical parameter analysis were found [6, 13–23]. Here, we describe and appraise these studies in chronological order.
San José et al. analysed the use of serum and pleural ADA and lysozyme in tuberculous pleurisy in 271 patients in Spain, of which 53 had TB. They found that pleural ADA had a sensitivity of 100% and a specificity of 93% for the diagnosis of TB, and that combining the use of pleural ADA and total protein in the form of a ratio increased the specificity to 95% at the expense of a reduction in sensitivity to 93%. Using a ratio involving pleural fluid ADA and lysozyme also increased the specificity to 95%, with a sensitivity of 80%. A ratio of pleural fluid lysozyme to total protein had a sensitivity of 60% and a specificity of 42% [13]. While these combinations improved the specificity, it was at the expense of a reduction in the sensitivity. This was a retrospective study involving a small number of TB cases. The authors used robust statistics but failed to describe parameters such as age and sex. There is also little information given regarding the diagnostic methods used in the tuberculous effusion group. The cases appear to be a mix of microbiological/histological and clinical diagnosis, the latter having not been proven. The ADA cut-off was different to the other studies described at 43 U/l (units per litre).
Muranishi et al. investigated the simultaneous measurement of ADA activity and tuberculostearic acid (TSA) in pleural effusions for the diagnosis of tuberculous pleuritis. Pleural effusions from 18 patients with tuberculous pleuritis, 16 patients with suspected tuberculous pleuritis, 14 patients with malignant effusions, six patients with parapneumonic effusions, five patients with cardiac failure-related effusions, three patients with collagen disease-related effusions and five patients with miscellaneous effusions were studied. They found that, when they analysed pleural fluid ADA and TSA in combination, the sensitivity increased from 56% (ADA alone) to 83%. The specificity remained at 76% [14]. The authors felt that the simultaneous measurement of both of these parameters was useful in the diagnosis of pleural effusions. There were a number of weaknesses with this study. It was a very small study and the sensitivity and specificity were relatively low when compared to the more recent data. It was retrospective and included cases where definitive proof of TB was absent, relying solely on high clinical suspicion. Therefore, some of the suspected TB cases will have been due to other aetiologies. They used an ADA cut-off level of 50 U/l, which differs from many of the other studies and did not describe the study population adequately (age/sex).
In 1993 in Brazil, De Oliveira et al. studied the usefulness of pleural fluid ADA in combination with pleural fluid lymphocyte proportion in 276 patients, of which 54 had TB. They found that using these tests in combination resulted in a sensitivity of 90.7% and a specificity of 97.7%. They concluded that the use of these tests in combination was a highly efficient diagnostic strategy of low cost that merits wider use [15]. While this study benefited from its prospective nature, there were a number of important weaknesses. Only 48% of the TB cases included in the study were actually proven either by microbiology or histology. Cardiac failure and very small effusions were excluded from this study, which has implications on the interpretation of the results. Only 61% of the neoplastic effusions had positive cytological or histological evidence of malignancy. The balance was made up of presumed malignancy. The ADA cut-off level was different to many other previous studies at 40 U/l. Finally, the statistical analysis was not well explained.
Villena et al. measured the concentration of pleural ADA and the ratio of pleural lysozyme (PL) to serum lysozyme (SL) in consecutive patients (49 tuberculous and 179 non-tuberculous) [16]. Using sensitivity and specificity curves, they established cut-off values at 33 U/l for ADA and 1.7 for the PL/SL ratio. The sensitivity of ADA activity for tuberculous effusion was 90%, with a specificity of 85%. Combining ADA with the PL/SL ratio enhanced the specificity to 99% [16]. However, they concluded that these markers should only suggest a diagnosis and point the clinician in the direction of pleural biopsy and pleural fluid cultures, and that values for ADA and lysozyme ratios are not, alone or in combination, sensitive or specific enough to replace pleural biopsy or culture of pleural fluid for the diagnosis of tuberculous empyema. This work had a number of good qualities. It was prospective and all patients followed the exact same diagnostic algorithm, with difficult cases discussed in a blinded manner by a multi-disciplinary panel. However, on the negative side, this study included cases where definitive histology or microbiology was not forthcoming and clinical suspicion alone was used. The non-tuberculous group was approximately 3.5 times the size of the tuberculous group. The findings were only relevant when diagnosing TB cases from a mix that includes parapneumonic, neoplastic and transudative effusions only. The ADA cut-off level of 33 U/l was again different to other studies. The analysis of pleural fluid lysozyme is also a contentious issue, with discrepancies in the results noted in previous work, possibly attributed to the method of analysis (turbidimetric vs. lysoplate). In this work, the sensitivity of lysozyme was reported to be much higher than previous reports. Again, in this study, there was inadequate description of the study population. Statistical analysis was robust and explained.
Burgess et al. analysed the differential cell counts and ADA on 303 of 472 consecutive pleural fluid samples after hemothorax, transudate and unsuitable samples were excluded. They found that, when ADA levels were combined with the lymphocyte/neutrophil ratio results, the accuracy of identifying TB increased compared with isolated ADA analysis [17]. When a positive ADA result was combined with a lymphocyte neutrophil ratio of 0.75 or greater, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy for the identification of TB were calculated to be 88, 95, 95, 88 and 92%, respectively [17]. The authors concluded that pleural fluid which met these criteria was very suggestive of TB. The good qualities of this work included the fact that it was a prospective study with a higher number of TB cases that were evenly distributed between men and women. The ADA detection method followed the well established Giusti method (used by all but one of the listed studies), although the cut-off used was 50 U/l [18]. The main problems with the work include the inclusion of suspected rather than definitive (microbiology or histology) cases. Transudates were excluded from the study, affecting its sensitivity and specificity when compared with other studies. Conclusions can only be drawn on exudative effusions. The study population was 68% mixed race, with a low number of Caucasian patients (16%); therefore, the findings may not be as relevant in the Caucasian population. The statistics used were not well described.
Villegas et al. evaluated the individual use of ADA, IFN-γ levels and polymerase chain reaction (PCR) in the diagnosis of tuberculous effusion in 140 cases of pleural effusion. They found that these tests had a sensitivity between 73–88% when used alone, but that the sensitivity and specificity increased when all three were used in combination [6]. Incidentally, they also found that a lower age and fever was associated with TB-related effusion. Pleural biopsy was also performed and had a sensitivity of 64.3 and a specificity of 98%. The authors concluded that their findings supported the use of new and more efficient diagnostic strategies in the management of pleural TB. This was a prospective study with a good male/female balance and a good mix of TB and non-TB cases. The ADA was analysed in a standardised fashion (Giusti); however, like the previous studies described, the cut-off level was not standardised, with a cut-off level of 45.3 U/l. Only 42 patients had confirmed TB; the rest were included due to high clinical suspicion. There was a significant frequency of false-negative PCR results in the study (26%). This is most likely attributable to the inefficient recovery of genomic DNA and the extraction of DNA from frozen samples. Nonetheless, this will have had a significant effect on the results of this study. Statistical analysis was robust and well explained.
Porcel and Vives retrospectively reviewed 106 patients with tuberculous effusions and 286 patients with malignant effusions over a 9-year period. They used two scoring systems, using clinical and laboratory variables where the main difference was the inclusion (model 2) or exclusion (model 1) of ADA [19]. They found that, using the scoring system from model 1, which was calculated by attributing scores to the results of measured variables, including an ADA ≥ 40 U/l (5 points), age <35 years [2], temperature ≥37.8 °C [2] and pleural fluid red blood cell count <5 × 109/L [1].
Model 2 involved a scoring system based on model 1 (excluding ADA) plus the following: no history of malignancy [3], pleural protein ≥50 g/L [1] and pleural fluid to serum lactate dehydrogenase ratio ≥2.2 [1]. Total scores ≥5 in model 1 and ≥6 in model 2 resulted in a sensitivity and specificity of 95 and 94, and 97 and 91, respectively, in the discrimination of tuberculous from malignant effusions [19]. This work, while involving larger numbers, was retrospective and again included cases of high clinical suspicion rather than exclusively involving confirmed cases. The other important weakness with this work was that their diagnostic tree method was not validated by the authors.
Ghanei et al. investigated the combination of pleural fluid ADA, LDH and lymphocyte to neutrophil ratio. In the combination of the three methods, with a positive result by either three of the methods considered to be indicative of a positive diagnosis of pleural TB, ADA activity plus LDH levels plus lymphocyte to neutrophil ratio in the pleural fluid yielded a sensitivity of 100%. This combination requiring all three methods to be positive in order for diagnosis to be made was 100% specific for pleural TB. They also found that using a combination of pleural fluid ADA and LDH yielded a sensitivity of 91.4% and a specificity of 100% [20]. This was a very small study where only 17 patients had a tuberculous effusion. They concluded that using these parameter combinations could lead to a diagnosis of pleural TB with an acceptable degree of confidence. While this was a prospective study with a good male/female balance and well-described robust statistical methods, the main criticism with this work is the small number of confirmed TB cases which were compared to a non-TB group that was approximately 3.5 times its size [17]. The ADA detection method was as per Giusti but, again, the cut-off level was different to other studies at 47 U/l.
Neves et al. prospectively analysed 215 patients with pleural effusions from 1997–2001, of which 104 were tuberculous, and found that the analysis of ADA, total serum leukocytes, percentile of lymphocytes, protein and duration of disease combined yielded a sensitivity and a specificity of >95% [21]. This was a retrospective study which excluded a large proportion of cases due to inadequate specimen collection or inappropriate handling of ADA specimens. ADA detection was as per Giusti, with a cut-off of 39 U/l. Of the TB cases included in the study, less than 10% of pleural fluid cultures and 58% of biopsy cultures were positive for TB. Acid fast staining was negative in all cases. Like Porcel and Vives’s work from 2003, the main weakness of this study was that the authors did not validate their predictive model. The statistics were well described and there was a good balance between TB and non-TB cases in the study.
Daniil et al. investigated the measurement of ADA, IFN-γ, C-reactive protein (CRP), carcinoembryonic antigen, interleukin-6, tumour necrosis factor-α and vascular endothelial growth factor concentration in pleural fluid and found that the combination of ADA and CRP increased the percentage of correctly classified individuals as having tuberculous rather than malignant or parapneumonic effusions in 92% of cases [22]. The study involved 72 patients, of which only 12 were tuberculous. The authors recommended further and larger studies in this area. While this was a prospective study using robust statistical methods, it was extremely small. ADA detection was again as per Giusti, with a cut-off of 42.2 U/l. The study involved twice as many males as females. The non-TB group was approximately 4.5 times the size of the TB group and the non-TB malignant group was highlighted by the unusual absence of lymphomatous effusions, which will have had an impact on the sensitivity and specificity.
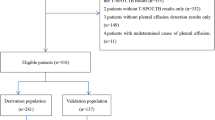
In 2008, Porcel et al., having already published in this area in 2003, described a decision tree for differentiating tuberculous from malignant effusions. They retrospectively compared clinical and pleural features of 238 adults with pleural effusion who satisfied diagnostic criteria for TB or malignancy [23]. They found that the combination of age >35 years, pleural fluid ADA >38 U/l, temperature ≥37.8°C and a pleural fluid LDH >320 U/l yielded a sensitivity of 92.2% and a specificity of 98.3%, allowing them to conclude that the use of this decision tree could help in the differential diagnosis of malignant and tuberculous effusions, but not of other forms of effusions [23]. This was a good sized retrospective study which only involved confirmed TB cases and not suspected ones. Importantly, it included a derivation cohort followed by a validation cohort. The limitations of this work are few but involve the important fact that this model is only useful in differentiating TB from malignancy and not from other forms of effusions. The ADA detection system was not like those of the previous studies described and the cut-off used with the detection system was 38 U/l. While it is limited by its retrospective nature, the study involved only objective clinical characteristics and laboratory parameters strengthening the data. The authors’ model is only relevant in areas of high prevalence and could lead to very different findings if used in the USA, for example, where prevalence is 3.4/100,000.
Lastly, Küpeli et al. have recently examined concurrent measurement of ADA and dipeptidyl peptidase (DPP) IV (T-cell-associated enzyme) activity in the diagnosis of tuberculous pleural effusion [24]. They found that using both of these markers together improved the sensitivity, specificity and diagnostic accuracy (77, 94 and 91%, respectively) when compared to analysing these markers separately [24]. This study involved 87 patients, of which 18 had TB. Apart from the small number of patients involved, Küpeli et al. included known transudates in their study, thus, increasing the diagnostic yield of the test. They concluded that, in an area of high prevalence, ADA levels in combination with that of DPP can be useful in the diagnosis of tuberculous pleural effusion with high specificity and accuracy. The strengths of this study include its prospective nature, robust statistics and its focus on definite TB cases only. Like many of the previous studies, it is limited by its extremely small number of TB cases [19]. The ADA analysis method was also different to other studies, as was the ADA cut-off level of 40 U/l. While this work was performed in an area of high prevalence, the age of the TB group was young, ranging from 17 to 30 years, and the male to female ratio was 3:1. Another limitation of the work is that parameter testing of each case occurred depending on the clinical scenario, rather than blindly testing all cases similarly.
Conclusion
The combination of tests and biomarkers to diagnose tuberculous pleural effusion in endemic areas where resources are limited or in cases where traditional investigation is negative but suspicion is high certainly has merit. Even in cases where ADA is unavailable, the use of clinical and demographic information in combination with a cell differential count, in high-incidence settings, can yield a diagnosis of TB with a high predictive value [25]. This concept has been further advanced, with a number of groups recommending the use of pleural fluid and clinical parameter combinations in the diagnosis of tuberculous pleural effusions, which we described in this review.
We believe that there are a number of advantages to using such scoring systems. They are cheap to perform (ADA costs $1.28 per test; Bio-Quant Inc., San Diego, CA, USA), due to not requiring clinical expertise (e.g. thoracoscopist), are associated with minimal morbidity, give a speedy result and are beneficial in areas of poor resources or in investigating elderly frail patients who are not suitable for more invasive procedures. If positive, anti-tuberculous therapy may be started straight away in areas of high prevalence as culture ± histology results are awaited.
They are also useful in those highly suspicious few patients that do not yield a definitive diagnosis after closed pleural biopsy or fluid analysis and culture.
While the advantages described above might appear obvious, it is also important to highlight a number of disadvantages with these tests. Firstly, the specificity of ADA is relatively low when compared to, for example, thoracoscopy and, therefore, it is important to remember that ADA in lymphocyte-rich effusions has been described in rheumatoid arthritis, mesothelioma, psittacosis, brucellosis, histoplasmosis, coccidioidomycosis, bronchoalveolar carcinoma, chlamydia and mycoplasma pneumonia, Mediterranean fever and in the majority of patients with empyema [26–29].
The benefits described in the studies in Table 1 have, in the majority of cases, been performed in areas where TB prevalence is high and data is, therefore, lacking from countries with lower prevalence. As ADA makes up part of the combination in all of the studies reviewed, it is important to highlight that ADA is less sensitive in countries of low TB prevalence and may lead to an under-diagnosis of pleural TB (however, TB may be excluded, particularly if ADA is negative and suspicion is moderate or low), which can lead to further organ spread in 65% of patients [30]. It is also possible that false-positive cases will be commenced on anti-tuberculous therapy, resulting in significant drug-related adverse effects. Importantly, the Infectious Diseases Society of America (IDSA) recommends the demonstration of M. tuberculosis in the sputum, pleural fluid or pleural biopsy specimen as their gold standard in diagnosing the condition and clearly do not recommend the replacement or substitution of this standard by pleural fluid and clinical combination tests [31]. Additionally, one of the most important disadvantages of using these combinations alone in the diagnosis of pleural TB is the fact that these combinations bypass the culture of fluid or tissue and, therefore, drug susceptibility testing is not performed in an era when drug-resistant TB is increasing. In the USA, Baumann et al. described resistance to a first-line treatment drug in 9.9% of pleural TB patients from 1993–2003 [32]. This can lead to treatment failure and clinical deterioration. Certainly, the use of combination tests may allow the commencement of four-drug therapy while pleural fluid culture is awaited, but if this is non-diagnostic, pleural biopsy will still be required, especially in those groups who have a higher rate of drug resistance [32].
Also, the process of testing for these markers does not offer any immediate therapeutic benefit, unlike thoracoscopy, which is not only diagnostic, but allows the removal of large pleural fluid collections, giving immediate relief to the patient. Other advantages highlighted earlier included the microscopic and macroscopic examination of tissue, leading to early drug testing prior to culture results and drug susceptibility testing on biopsied tissue.
While the studies listed here appear to demonstrate a benefit of combination (particularly those involving ADA) over single-parameter testing, the authors feel that there is currently insufficient evidence available to conclude whether the use of clinical and biochemical parameter combinations should be routinely used to diagnose tuberculous effusions. Studies have involved low numbers of patients and all have recommended the use of different parameters, thus, lacking consensus. Other problems with the studies include the variable prevalence rates associated with the different countries where the research took place, the different ADA detection methods and cut-off levels used, the variable study design (retrospective versus prospective), the regular inclusion of unproven TB cases in the studies, as well as the lack of gold-standard controls in all but one study.
Further large studies are required to validate their use and studies in areas of low TB prevalence are also warranted in order to investigate the suitable use of these combination tests in these areas. In particular, the study by Porcel et al. in 2008 would benefit from validation in an area of low prevalence, as it was one of the stronger studies performed by a world-recognised research group with a good demographic distribution, robust statistics and large study size. Studies which intend to include ADA might benefit from using the more specific ADA2 isoenzyme, which may increase the sensitivity and specificity further. Furthermore, while at best these combinations may strongly suggest a diagnosis in endemic areas warranting the commencement of drug therapy, their use as a replacement to the demonstration of M. tuberculosis in culture or histology will require randomised control trials comparing these parameters with the gold standard of thoracoscopic biopsy for microbiology and histology. If they performed well in these trials, their regular use may be validated; however, the problem still arises regarding susceptibility testing in areas of high drug resistance.
While we await these studies, we believe that combination tests may be used in current practice in areas of high prevalence to steer the physician towards a diagnosis, allowing therapy to start and continue or be adjusted once definitive proof has been achieved with culture or histology. They may also be useful in endemic areas with poor resources, such as the Sub-Saharan region, where diagnosis is often made clinically or empirically, as no other resources are available [33].
Clearly, the use of a combination of parameters to diagnose tuberculous effusions has great potential for both physicians and patients involved. The benefits in the acute setting, in patients with negative initial results despite high clinical suspicion, in frail patients unable to undergo pleural biopsy combined with their cheap cost, are considerable in regions where TB is endemic. Their use in areas where the incidence of TB is low is less valid. As a result, further clinical assessment of these combinations through larger studies and randomised trials may validate their general and routine use in medical practice and, in particular, identify a robust combination that yields the highest sensitivity and specificity.
References
Porcel JM (2009) Tuberculous pleural effusion. Lung 187(5):263–270
World Health Organization (WHO) (2008) Global tuberculosis control: surveillance, planning, financing. WHO, Geneva, Switzerland
Escudero Bueno C, García Clemente M, Cuesta Castro B, Molinos Martín L, Rodríguez Ramos S, González Panizo A et al (1990) Cytologic and bacteriologic analysis of fluid and pleural biopsy specimens with Cope’s needle. Study of 414 patients. Arch Intern Med 150(6):1190–1194
Seibert AF, Haynes J Jr, Middleton R, Bass JB Jr (1991) Tuberculous pleural effusion. Twenty-year experience. Chest 99(4):883–886
Chakrabarti B, Davies PD (2006) Pleural tuberculosis. Monaldi Arch Chest Dis 65(1):26–33
Villegas MV, Labrada LA, Saravia NG (2000) Evaluation of polymerase chain reaction, adenosine deaminase, and interferon-gamma in pleural fluid for the differential diagnosis of pleural tuberculosis. Chest 118(5):1355–1364
Valdés L, Alvarez D, San José E, Penela P, Valle JM, García-Pazos JM et al (1998) Tuberculous pleurisy: a study of 254 patients. Arch Intern Med 158(18):2017–2021
Diacon AH, Van de Wal BW, Wyser C, Smedema JP, Bezuidenhout J, Bolliger CT et al (2003) Diagnostic tools in tuberculous pleurisy: a direct comparative study. Eur Respir J 22:589–591
World Health Organization. Global TB Database
Liang QL, Shi HZ, Wang K, Qin SM, Qin XJ (2008) Diagnostic accuracy of adenosine deaminase in tuberculous pleurisy: a meta-analysis. Respir Med 102(5):744–754
Jiang J, Shi HZ, Liang QL, Qin SM, Qin XJ (2007) Diagnostic value of interferon-gamma in tuberculous pleurisy: a metaanalysis. Chest 131(4):1133–1141
Hooper CE, Lee YC, Maskell NA (2009) Interferon-gamma release assays for the diagnosis of TB pleural effusions: hype or real hope? Curr Opin Pulm Med 15(4):358–365
San José E, Valdés L, Sarandeses A, Alvarez D, Chomon B (1992) Diagnostic value of adenosine deaminase and lysozyme in tuberculous pleurisy. Clin Chim Acta 31(1–2):73–81
Muranishi H, Nakashima M, Hirano H, Saitoh T, Takahashi H, Tanaka K et al (1992) Simultaneous measurements of adenosine deaminase activity and tuberculostearic acid in pleural effusions for the diagnosis of tuberculous pleuritis. Intern Med 31(6):752–755
De Oliveira HG, Rossatto ER, Prolla JC (1994) Pleural fluid adenosine deaminase and lymphocyte proportion: clinical usefulness in the diagnosis of tuberculosis. Cytopathology 5(1):27–32
Villena V, Navarro-Gonzálvez JA, García-Benayas C, Manzanos JA, Echave J, López-Encuentra A et al (1996) Rapid automated determination of adenosine deaminase and lysozyme for differentiating tuberculous and nontuberculous pleural effusions. Clin Chem 42(2):218–221
Burgess LJ, Maritz FJ, Le Roux I, Taljaard JJ (1996) Combined use of pleural adenosine deaminase with lymphocyte/neutrophil ratio. Increased specificity for the diagnosis of tuberculous pleuritis. Chest 109(2):414–419
Giusti G (1974) Adenosine deaminase. In: Bergmeyer HU (ed) Methods of enzymatic analysis. Academic Press, New York, pp 1092–1096
Porcel JM, Vives M (2003) Differentiating tuberculous from malignant pleural effusions: a scoring model. Med Sci Monit 9(5):CR175–CR180
Ghanei M, Aslani J, Bahrami H, Adhami H (2004) Simple method for rapid diagnosis of tuberculosis pleuritis: a statistical approach. Asian Cardiovasc Thorac Ann 12(1):23–29
Neves DD, Dias RM, Cunha AJ (2007) Predictive model for the diagnosis of tuberculous pleural effusion. Braz J Infect Dis 11(1):83–88
Daniil ZD, Zintzaras E, Kiropoulos T, Papaioannou AI, Koutsokera A, Kastanis A et al (2007) Discrimination of exudative pleural effusions based on multiple biological parameters. Eur Respir J 30(5):957–964
Porcel JM, Alemán C, Bielsa S, Sarrapio J, Fernández de Sevilla T, Esquerda A (2008) A decision tree for differentiating tuberculous from malignant pleural effusions. Respir Med 102(8):1159–1164
Küpeli E, Karnak D, Elgün S, Argüder E, Kayacan O (2009) Concurrent measurement of adenosine deaminase and dipeptidyl peptidase IV activity in the diagnosis of tuberculous pleural effusion. Diagn Microbiol Infect Dis 65(4):365–371
Trajman A, Pai M, Dheda K, van Zyl Smit R, Zwerling AA, Joshi R et al (2008) Novel tests for diagnosing tuberculous pleural effusion: what works and what does not? Eur Respir J 31(5):1098–1106
Light RW (2001) Tuberculous pleural effusions. In: Light RW (ed) Pleural diseases, 4th edn. Williams and Wilkins, Philadelphia, PA
Ferrer J (1997) Pleural tuberculosis. Eur Respir J 10:942–947
Sharma SK, Mohan A (1996) Adenosine deaminase in the diagnosis of tuberculosis pleural effusion. Indian J Chest Dis Allied Sci 38:69–71
Laniado-Laborín R (2005) Adenosine deaminase in the diagnosis of tuberculous pleural effusion: is it really an ideal test? A word of caution. Chest 127:417–418
Roper WH, Waring JJ (1955) Primary serofibrinous pleural effusion in military personnel. Am Rev Tuberc 71:616–634
Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN et al (2003) American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med 167:603–662
Baumann MH, Nolan R, Petrini M, Lee YC, Light RW, Schneider E (2007) Pleural tuberculosis in the United States: incidence and drug resistance. Chest 131(4):1125–1132
Reuter H (2008) Tuberculous pericarditis and HIV infection in Africa. S Afr Med J 98:29–30
Author information
Authors and Affiliations
Corresponding author
Additional information
We have no financial or conflict of interests.
Rights and permissions
About this article
Cite this article
McGrath, E.E., Anderson, P.B. Diagnostic tests for tuberculous pleural effusion. Eur J Clin Microbiol Infect Dis 29, 1187–1193 (2010). https://doi.org/10.1007/s10096-010-0986-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-010-0986-z