
Abstract
Iron plays a major role in the growth and virulence of ferrophilic organisms like Vibrio vulnificus. People who reside in the coastal areas with raw fish eating habits have a high risk of Vibrio infection and aggressive therapy can only reduce their mortality. We investigated the in vitro efficacy of ciprofloxacin, a bactericidal drug used in V. vulnificus patients, and the orally active iron chelator deferasirox against V. vulnificus infection. We performed in vitro time-kill studies on two ATCC strains and one clinical isolate of V. vulnificus collected from a patient admitted to Chosun University Hospital with either ciprofloxacin or iron chelator deferasirox alone and the two drugs in combination. The combination of an iron chelator plus an antibiotic creates a novel form of synergism at 24 h. The antimicrobial effect of deferasirox may be ascribed to its ability to deplete iron that would otherwise be used for bacterial growth. Combination therapy with ciprofloxacin plus deferasirox has potential clinical application by lowering the iron availability against a ferrophilic organism like V. vulnificus infections.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vibrio vulnificus, an opportunistic and emerging pathogen of humans, is a halophilic gram-negative, motile, curved marine bacterium that is endemic in warm coastal waters. V. vulnificus infection is extremely invasive and rapidly fatal [1], and the prognosis is directly linked to the speed and accuracy of the diagnostic and treatment measures [2]. Mortality rates increase by 33–53% if treatment is delayed by 24 h, and approach 100% in patients not treated within 72 h [2, 3]. Treatment involves the administration of highly active antimicrobial agents and, when necessary, surgical debridement. V. vulnificus infection is associated with a variety of clinical syndromes: primary septicemia with high fever and chills; wound infection caused by direct inoculation; and gastrointestinal, characterized by vomiting, diarrhea, and abdominal pain [4]. Persons who are immunocompromised or have elevated serum iron levels, typically due to chronic liver damage, long-term alcohol abuse, or hemochromatosis, are highly vulnerable to infection by V. vulnificus [4, 5].
Iron plays an essential and complex role in the growth and virulence of virtually all microbial pathogens [6]. The level of freely available iron in the body is too low to sustain the growth of bacteria [7]. However, some pathological conditions in the body increase the availability of iron as a result of the release of intracellular iron due to cell death, or a rise in transferrin iron saturation level; as a consequence, host susceptibility to a variety of ferrophilic pathogens, including V. vulnificus, is augmented [8, 9].
No time-kill study has been performed on V. vulnificus infections using a combination of an antimicrobial agent and the iron chelator deferasirox. Deferasirox (Exjade, DFS) is a tridentate iron chelator belonging to a new class of oral chelator available for routine use in the United States, Europe, and many parts of the world against transfusional iron overload in pediatric and adult patients. We have investigated the in vitro efficacy of ciprofloxacin, a bactericidal drug used in V. vulnificus patients, and the orally active iron chelator deferasirox. It appeared to be a matter of considerable interest to establish whether the potential antimicrobial action of deferasirox augmented the antimicrobial efficacy of antibiotics.
Materials and methods
Bacterial strains
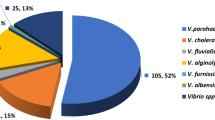
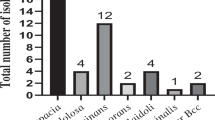
V. vulnificus ATCC 27562 was obtained form the American Type Culture Collection, ATCC 33815 was purchased from the Korean Collection for Type Cultures (KCTC) Center, and 14 clinical isolates of V. vulnificus for the susceptibility test were selected randomly from the samples collected from the patients admitted to Chosun University Hospital, Gwangju, South Korea, in the period 2006 to 2008. The two ATCC strains and one clinical isolate CUH 42-14 were used in the time-kill studies.
Reagents
The media used in this study were Mueller–Hinton broth and Mueller–Hinton agar (Difco Laboratories, Detroit, MI, USA). Standard ciprofloxacin powder was obtained from Bayer HealthCare, Korea, and deferasirox from Novartis Pharma, Basel, Switzerland. Both reagents were prepared as 2.048 mg/mL stock solutions, and the deferasirox was dissolved in dimethyl sulfoxide (DMSO; Amresco, Solon, OH, USA).
MICs
The minimum inhibitory concentrations (MICs) of ciprofloxacin and deferasirox for all 14 clinical isolates and two ATCC strains were determined based on the Clinical and Laboratory Standards Institute (CLSI) guidelines for the micro-broth dilution procedure [10]. The MICs of ciprofloxacin readings were interpreted using the CLSI breakpoint criteria. The MIC was defined as the lowest concentration of a drug that completely inhibited visible growth of the organism.
Time-kill studies
Time-kill studies were performed to evaluate synergy, as previously described [11, 12]. Bacteria were diluted to a standard cell suspension of about 5.0 × 105 CFU/mL in 50 mL fresh Mueller–Hinton broth (MHB) containing 2% NaCl in a 250-mL conical flask and exposed to the drug. To evaluate the in vitro activities of the drugs, the 3/4 MICs of ciprofloxacin and 1.5 MIC of deferasirox were compared individually and in combination. Control growth was assessed in an additional conical flask without drugs. The flasks were incubated at 35°C in a shaking incubator at 200 rpm. Then, 2-, 4-, 8-, 12-, and 24-h aliquots of 100 µl were taken, diluted 10-fold in freshly prepared MHB containing 2% NaCl, and cultured overnight at 37°C on duplicate Muller–Hinton Agar (MHA) plates also containing 2% NaCl. Synergy is defined as a decrease of ≥2 log10 (100-fold drop) in CFU per milliliter in the drug combination compared to the most active single constituent [13]. Indifference and antagonism were defined at 24 h as a ± 1 log10 kill to <2 compared to the most efficient agent alone and >1 log10 growth compared with the less active single agent, respectively. All of the experiments were performed at least in duplicate.
Results
MICs
The MICs for ciprofloxacin and deferasirox against all 14 clinical isolates and two ATCC strains of V. vulnificus are shown in Table 1.
Time-kill studies
The time-kill study of ATCC 27562 revealed growth inhibition by 0.0225 µg/mL ciprofloxacin (3/4 MIC) and 12 µg/mL deferasirox (1.5 MIC) until 8 h and 12 h, respectively; the bacteria then began to regrow and increased to an extended level. In the combination regimen, ciprofloxacin (3/4 MIC) plus deferasirox (1.5 MIC) had an inhibitory effect up to 24 h and the mean reduction in bacterial counts was 3.79 ± 0.27 CFU/mL, and showed synergistic effect (Fig. 1a).

Time–kill kinetics of Vibrio vulnificus (a) ATCC 27562, (b) ATCC 33815, and (c) CUH 42-14 during incubation with 3/4 MIC ciprofloxacin, 1.5 MIC deferasirox, and the combination of 3/4 MIC ciprofloxacin and 1.5 MIC deferasirox. The initial inoculum of V. vulnificus was 5×105 CFU/mL
Similarly, with ATCC 33815, ciprofloxacin inhibited the growth of bacteria at 0.0469 µg/mL (3/4 MIC),and deferasirox at 12 µg/mL (1.5 MIC), up to 12 h and 2 h, respectively. A combination regimen of ciprofloxacin (3/4 MIC) plus deferasirox (1.5 MIC) also showed growth inhibition up to 12 h, with less killing of bacteria than ciprofloxacin monotherapy. Although bacteria in all three regimens started to proliferate after 12 h, the mean reduction of the bacterial counts in combination therapy was 5.15 ± 0.61 log CFU/mL as compared to a single active agent of ciprofloxacin at 24 h and indicating clear synergistic effect (Fig. 1b).
The time-kill study of clinical isolate CUH 42-14 revealed a growth inhibitory effect of ciprofloxacin at 0.0225 µg/mL (3/4 MIC) up to 8 h and of deferasirox at 12 µg/mL (1.5 MIC) up to 12 h. However, in a combination regimen of ciprofloxacin (3/4 MIC) and deferasirox (1.5 MIC), the growth inhibitory effect continues until 24 h and the mean reduction of bacterial counts was 2.17 ± 0.32 log CFU/mL as compared to the most active single agent of deferasirox and showed synergistic effect (Fig. 1c).
Discussion
V. vulnificus is a halophilic gram-negative bacillus that causes life-threatening skin and soft tissue infections. Chuang et al. [11] reported synergism between cefotaxime and minocycline by inhibiting V. vulnificus in vitro, and fluoroquinolones alone have been shown to be as effective as the combination of cefotaxime plus minocycline in vitro and in vivo [14]. Many combinations of antimicrobial agents have been studied for treating V. vulnificus infections [1, 4, 11, 14], but few effective combinations to reduce mortality effectively have been identified.
Elevated serum iron levels may play an important role in the pathogenesis of V. vulnificus infections [9]. The standard iron chelating agent, deferoxamine, a hydroxamate siderophore derived from streptomyces species, can accelerate the in vitro growth of many ferrophilic organisms, such as V. vulnificus, Yersinia enterocolitica, and Mucorales. These organisms bind specifically to deferoxamine iron complexes and strip the iron from the chelator via an energy-dependent reductive process, so facilitating iron uptake [15]. V. vulnificus is known to bind deferoxamine (Desferal) via the specific receptor DesA [16]. Hence, in some patients treated with iron chelator such as deferoxamine in whom yersiniosis or mucormycosis was promoted, the drug may have enhanced the growth of a microbial or neoplastic cell invader by acting as a siderophore instead of assisting the host [17]. Indeed, Neupane and Kim showed recently that the growth of V. vulnificus was stimulated by deferoxamine, whereas two other oral chelators, deferasirox and deferiprone, had an inhibitory effect on growth [18]. Hence, deferasirox and deferiprone are not only useful for the treatment of iron overload, but also function as antimicrobial agents with the potential to act synergistically with various antibiotics [19].
Kim et al. suggested that iron chelation therapy may be an effective means for preventing the growth of V. vulnificus in susceptible patients [9]. Therefore, we investigated the in vitro efficacy of the combination of ciprofloxacin plus deferasirox compared to monotherapy with ciprofloxacin against V. vulnificus. When ciprofloxacin at 3/4 MICs was combined with deferasirox at 1.5 MICs, the inhibition of bacterial growth persisted in vitro in all strains for at least 24 h, and the combination was superior to ciprofloxacin alone. The antimicrobial effect of deferasirox may be ascribed to its ability to deplete iron that would otherwise be used for bacterial growth. The combination of an iron chelator plus an antibiotic creates a novel form of synergism. It is possible that the quinolone antibiotic interferes with DNA gyrase and that the microbe, therefore, becomes more sensitive to iron deprivation [19]. Based on our time-kill studies, it would appear that ciprofloxacin plus deferasirox is more active combination than ciprofloxacin alone against V. vulnificus. Even though ciprofloxacin plus deferasirox had a synergistic effect against V. vulnificus, it should be noted that, at early times, ciprofloxacin alone appeared to be more active than the combination treatment. In other experiments, we have found that the higher the ciprofloxacin concentration, the more effective it was at inhibiting the proliferation of micro-organisms (data not shown). Therefore, a high dose of ciprofloxacin may be required to overcome the suboptimal effect of ciprofloxacin plus deferasirox at early times. It will be important to test for the in vivo synergism of this combination to establish the clinical relevance of our findings.
In conclusion, our in vitro time-kill results show that ciprofloxacin plus deferasirox is superior to ciprofloxacin alone. Iron chelators such as deferasirox may, therefore, have clinical utility in combination with antibiotics such as ciprofloxacin on account of their ability to exploit the ferrophilic characteristics of V. vulnificus.
References
Kim DM, Lym Y, Jang SJ, Han H, Kim YG, Chung CH et al (2005) In vitro efficacy of the combination of ciprofloxacin and cefotaxime against Vibrio vulnificus. Antimicrob Agents Chemother 49:3489–3491
Bross MH, Soch K, Morales R, Mitchell RB (2007) Vibrio vulnificus infection: diagnosis and treatment. Am Fam Physician 76(4):539–544
Klontz KC, Lieb S, Schreiber M, Janowski HT, Baldy LM, Gunn RA (1988) Syndromes of Vibrio vulnificus infections. Clinical and epidemiologic features in Florida cases, 1981–1987. Ann Interm Med 109:318–323
Chiang SR, Chuang YC (2003) Vibrio vulnificus infection: clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect 36:81–88
Simpson LM, Oliver JD (1983) Siderophore production by Vibrio vulnificus. Infect Immun 41:644–649
Lankford CE (1973) Bacterial assimilation of iron. CRC Crit Rev Microbiol 2:273–331
Kushner JP (1988) Hypochronic anemias. In: Wyngaarden JB, Smith LH (eds) Cecil textbook of medicine, vol 1, 18th edn. WB Saunders, Philadelphia, PA, pp 892–900
Bullen JJ, Rogers HJ, Spalding PB, Ward CG (2005) Iron and Infection: the heart of the matter. FEMS Immunol Med Microbiol 43:325–330
Kim CM, Park RY, Choi MH, Sun HY, Shin SH (2007) Ferrophilic characteristics of Vibrio vulnificus and potential usefulness of iron chelation therapy. J Infect Dis 195:90–98
Clinical and Laboratory Standards Institute (CLSI) (2008) Performance standards for antimicrobial susceptibility testing; eighteenth informational supplement, vol 28, no 1. Document no. M100–S18. CLSI, Wayne, PA
Chuang YC, Liu JW, Ko WC, Lin KY, Wu JJ, Huang KY (1997) In vitro synergism between cefotaxime and minocycline against Vibrio vulnificus. Antimicrob Agents Chemother 41:2214–2217
Kim DM, Yun NR, Chung JH, Ryu HH (2008) Time kill studies of antibiotics against a nalidixic acid resistant Salmonella enterica serotype Typhi. Infect Chemother 40:207–211
Moland ES, Craft DW, Hong Sg, Kim SY, Hachmeister L, Sayed SD et al (2008) In vitro activity of tigecycline against multidrug-resistant Acinetobacter baumannii and selection of tigecycline–amikacin synergy. Antimicrob Agents Chemother 52:2940–2942
Tang HJ, Chang MC, Ko WC, Huang KY, Lee CL, Chuang YC (2002) In vitro and in vivo activities of newer fluoroquinolones against Vibrio vulnificus. Antimicrob Agents Chemother 46:3580–3584
Kim DM, Cho HS, Kang JI, Kim HS, Park CY (2008) Deferasirox plus ciprofloxacin combination therapy after rapid diagnosis of Vibrio vulnificus sepsis using real-time polymerase chain reaction. J Infection 57:489–492
Kim CM, Park YJ, Shin SH (2007) A widespread deferoxamine-mediated iron-uptake system in Vibrio vulnificus. J Infect Dis 196(10):1537–1545
Kontoghiorghes GJ, Weinberg ED (1995) Iron: mammalian defense systems, mechanisms of disease, and chelation therapy approaches. Blood Rev 9(1):33–45
Neupane GP, Kim DM (2009) Comparison of the effects of deferasirox, deferiprone, and deferoxamine on the growth and virulence of Vibrio vulnificus. Transfusion 49:1762–1769
van Asbeck BS, Marcelis JH, van Kats JH, Jaarsma EY, Verhoef J (1983) Synergy between the iron chelator deferoxamine and the antimicrobial agents gentamicin, chloramphenicol, cefalothin, cefotiam and cefsulodin. Eur J Clin Microbiol 2:432–438
Acknowledgments
The authors do not have any commercial interest or other association that might pose a conflict of interest.
This study was supported by research funds from Chosun University, 2009.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Neupane, G.P., Kim, DM. In vitro time-kill activities of ciprofloxacin alone and in combination with the iron chelator deferasirox against Vibrio vulnificus . Eur J Clin Microbiol Infect Dis 29, 407–410 (2010). https://doi.org/10.1007/s10096-010-0875-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-010-0875-5