
Αbstract
R1 and R2 blink reflex latencies were investigated blind in 55 patients with chronic tension-type headache, 55 patients with migraine, and 55 headache-free controls. Standard electrical stimulation of the supraorbital nerve was applied and the response was recorded from the ipsilateral orbicularis oculi muscles. There were no R1 or R2 latency differences between the three groups. During migraine attacks we observed a statistically significant reduction of R2 amplitude and area. The main finding of our study was the elicitation of the late R2” response at different interstimulus intervals in migraine patients compared to the tension-type headache and control groups. This could be considered an indication of habituation mechanism hyperexcitability, although further investigation is needed to confirm these findings and establish the neurophysiologic basis. This study suggests that blink reflex studies can be used routinely as a non-evasive and inexpensive method for the evaluation of headache patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Certain aspects of the pathophysiology underlying migraine and other primary headaches remain ominous. Over the years, extensive research has focused on neuroanatomical structures that are involved in the pathogenesis of various headache types [1].
Trigeminal system nociceptive input modulation and mechanisms of activation have been implicated as key-role factors of migraine [2]. Alterations of central and peripheral nervous system components may stimulate the trigeminovascular system in migraine, resulting in secondary vasomotor changes and pain [3]. Deficient endogenous pain control mechanisms due to either decreased activation or excessive inhibition of brain stem inhibitory interneuronal activity are also contributing factors, as it was shown regarding the pathogenesis of Tension-type headache (TTH) [4].
Blink reflex is an objective quantitative neurophysiological method used in the evaluation of trigeminal system function because the afferent part of the reflex arch is via the trigeminal nerve [5,6,7]. This reflex is obtained by stimulation of the supraorbital nerve on one side of the face, leading to two ipsilateral responses (R1 and R2) and one contralateral response (R2c). R1 indicates an oligosynaptic pathway involving the main sensory nucleus of the trigeminal nerve and the intermediate subnucleus of the facial nerve. The second response, R2, involves a pathway of descent to the spinal trigeminal tract. The contralateral response, R2c, reflects the bridge of the brainstem in the medulla and moving to the reticular formation to produce a response at the contralateral facial nucleus [5,6,7]. Blink reflex abnormalities have been reported in various neurological diseases that affect the brainstem, such as stroke, Parkinson’s disease and multiple system atrophy [8, 9]. BR alterations may reflect brainstem dysfunction due to destructive lesions or excitability changes in various types of headache [10].
Techniques utilizing the habituation of blink reflex responses (process of reduced responses to repetitive stimuli over time) have been established as important electrophysiological tools to detect alterations of trigeminal system function in cranial pain disorders such as migraine, TTH and cervicogenic headache [11]. Several studies concerning the subject have reported contradictory results possibly due to patient selection and methodology bias.
We studied conventional blink reflex and habituation of blink reflex at different interstimulus intervals in patients with migraine and TTH interictally and during spontaneous attacks, compared to habituation in normal subjects. Our aim was to prove the efficiency of this method as an easily applicable and reproducible procedure that could be routinely used in the differentiation of these common headache types.
Materials and methods
Subjects of both genders, aged 18–75 years, who suffered from TTH and episodic migraine (fewer than 15 days per month) according to International Headache Society guidelines were enrolled [12]. The patients were recruited once per week from the outpatient Headache Clinic at the Korgialenio Benakio Hospital of Athens from January 2014 to March 2015 and were given a complete physical and neurological examination. During the recruitment day, all patients who visited the outpatient clinic were asked to participate in the study after fulfilling the eligibility criteria and providing their informed consent. The main exclusion criteria were other primary or secondary headaches and severe psychiatric disorders. We excluded patients with prophylactic medication for headache, tricyclic antidepressants or benzodiazepines, as well as those that had a history of analgesic abuse. Patients with a history suggestive of ischemic heart disease, cardiac arrhythmia requiring medication, epilepsy, hypertension, impaired hepatic or renal function or both, pregnancy or breast-feeding, and other neurological diseases were excluded. In addition, healthy controls without any history of headache or other pain symptoms, nor medication taken, matched for sex and age were investigated. Informed consent was obtained from all participants. The study was approved by the Korgialenio Benakio Hospital Scientific and Ethics Committee and was consistent with the Declaration of Helsinki.
Migraine and TTH patients were examined twice; during pain and symptom-free periods, with a minimum time interval of 2 days from the previous headache attack. Headache intensity was scored on a verbal numerical rating scale from 0 to 3 (with 0 = no headache at all, 1 = very mild headache, 2 = medium headache severity and 3 = the worst possible headache). During pain, all patients scored 3 on the rating scale.
The recordings were performed by the same researcher throughout the study with standardized methodology. Nihon-Kohden Neuropack 8 EMG/EP equipment was used in all recordings.
During the recording session, the subjects were supine in a quiet temperature controlled room, with the head slightly elevated and the eyes lightly closed. Surface-recording active electrodes were placed over the orbicularis oculi muscles bilaterally. Surface-recording reference electrodes were placed over the respective temples.
Blink reflex habituation was elicited according to the method described by Kimura [9]. Percutaneous pulses were delivered over the right supraorbital foramen with 5 mm diameter and 19.62 mm2 surface electrodes. A habituation program was used to deliver paired pulses of 0.1 ms duration with an interstimulus interval that progressively increased in a step-wise manner on successive separate recordings from 100 to 700 ms in 100 ms increments. The typical intensity stimulus to elicit a maximally stable R1 response was between 10 and 12 mA. A 50-s time interval was allowed between successive trials to minimize interaction (figure S1 supplemental material).
We chose to limit the study to a right-sided stimulation to avoid a lengthy, uncomfortable procedure. The first sweep of each block was excluded from further analysis to avoid contamination with a startle response.
We recorded the R1 and R2 ipsilateral response to the first stimuli of the paired pulse and also the ipsilateral late response to the second stimuli called R2”. The length of the interstimulus interval that was accompanied by elicitation of the R2” response (100, 200 ms, etc.) was used as a marker of the trigeminal system excitability level. R1, R2 and R2” recorded parameters were latency (ms), amplitude (mV), surface area (mV/ms) and the R2/R2” area ratio on each measurement. R2” responses were accepted if they displayed an R2”/R2 percentage ratio over 10%.
Statistical analysis
Continuous variables are presented with mean and standard deviation (SD). Quantitative variables are presented with absolute and relative frequencies. For the comparison of proportions of agents that respond at each point of time Chi-square and Fisher’s exact tests were used. For the comparison of Blink Reflex Components between the different group measurements analysis of variance (ANOVA) was used. Bonferroni correction was used in multiple comparisons to control for type I error. Kruskal–Wallis test was used for the comparison of time for R2” response. All p values reported are two-tailed. Statistical significance was set at 0.05 and analyses were conducted using SPSS statistical software (version 19.0).
Results
Sample consisted of 165 subjects: 55 in the migraine group 21 men and 34 women) with mean age 36.5 years (SD 11.6 years), 55 in the TTH group (18 men and 37 women) with mean age 35.6 years (SD 14.1 years) and 55 healthy volunteers (18 men and 37 women) with mean age 34.2 years (SD 13.4 years). The characteristics of patients and controls are presented in Table 1.
The groups were similar in terms of sex and age (p = 0.786 and p = 0.482, respectively).
Blink reflex R1 response latencies (p = 0.411), amplitude (p = 0.512) and area (p = 0.314) did not differ significantly between the study groups. Blink Reflex Components measurements in the controls, in subjects with migraine with and without pain and in TTH subjects with and without pain are shown in Table 2.
There were no significant differences in R2 latencies between the five measurements (p = 0.098). R2 area values were significantly lower in migraine with pain measurements as compared with other measurements including measurements in migraine without pain (p < 0.001; Fig. 1).

Error bars represent the ipsilateral R2 area of nociceptive blink reflexes as means with 95% confidence interval for each group (controls, TTH free of pain, TΤH with pain, Migraine free of pain, Migraine with pain). R2 area values were significantly lower in migraine with pain as compared with others groups. *Significant at p < 0.05
R2 amplitude was also significantly lower in migraine with pain measurements as compared with other measurements (p < 0.001 for all comparisons; Fig. 2).

Error bars of R2 represent the ipsilateral R2 amplitude of nociceptive blink reflexes as means with 95% confidence interval for each group (controls, TTH free of pain, TΤH with pain, Migraine free of pain, Migraine with pain). R2 amplitude was also significantly lower in migraine with pain as compared with other groups. *Significant at p < 0.05
TTH patients free of pain and control subjects showed similar R2 amplitude and area values (Figs. 1, 2).
During habituation studies we recorded the time interval between the stimuli of the paired pulse that was accompanied by elicitation of the R2” response. The parameters of the elicited R2” response in migraineurs (latency, amplitude, area) displayed a similar pattern as the R2 response of the conventional blink reflex presented in Table 2. Symptom-free periods were characterized by increased R2” amplitude and area (p < 0.001) in opposition to migraine attacks where amplitude and area values were significantly decreased compared to TTH patients and controls (p < 0.001). In healthy subjects and TTH patients, R2” response was elicited in similar interstimulus intervals.
We further analyzed the differences among the five group measurements regarding the time of response at R2” and the ratio R2”/R2 (Table 3).
We divided each group into subgroups according to the point of time of response to R2” and we examined how the percentage of agents that respond at each point of time differs from one group to the other. In control subjects, habituated R2” responses presented for the first time in 1.8, 3.6, 58.2, 32.7, 1.8 and 1.8% of the control group at 100, 200, 300, 400, 500 and 600 ms, respectively. Habituation correspondence values in TTH patients were not significantly different in comparison to controls (p = 0.489).
Migraine patients during symptom-free periods readily respond to the second stimulus of the paired pulse at a shorter interval. On the contrary, during migraine attacks point of time for R2” response was recorded after significantly longer time intervals (figure S2 supplemental material; p < 0.001).
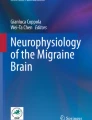
In migraines during pain particular R2” responses were absent at 100 and 200 ms and were usually recorded at 400, 500, 600 and 700 ms intervals (19.7, 26.6, 28.3 and 26.6%, respectively, Table 3). Figure 3 shows box plots for point of time of R2” Response for the different group measurements.

Box plot for point of time of R2” response for the different group measurements (controls, TTH free of pain, TΤH with pain, Migraine free of pain, Migraine with pain). The horizontal black line gives the median, the box the interquartile range (between upper and lower quartile). The whisker gives the maximum and the minimum. The cycles represents outliers of the data. During migraine attacks point of time for R2” response was recorded after significantly longer time intervals (p < 0.05 regarded as significant). TTH tension-type headache
Discussion
The main finding of our study was the elicitation of the late R2” response at different interstimulus intervals (ISI) in migraine patients compared to the ΤΤΗ and control groups. This alteration of the R2” recovery cycle reflects the highly variable functional status of habituation mechanisms. The R2” component was recorded in significantly shorter ISI during interictal measurements in migraineurs indicative of habituation failure. Early studies attributed this deficit of the habituative process in migraine patients to hyperexcitability of brainstem interneurons that are involved in the polysynaptic arc of the R2” response through the lateral reticular formation, the spinal trigeminal nucleus and the facial nucleus [9]. These theories are in concordance with the finding of increased brainstem activity during migraine attacks, as it was shown by Positron Emission Tomography studies [5].
Further investigations revealed that migraine patients display a more widespread habituation deficit that includes cortical polysynaptic activity. Contingent Negative Variation (CNV) studies, as well as cortical auditory and visually evoked potentials showed that global impairment of habituation may contribute to the susceptibility of migraine patients [13,14,15]. The habituation deficit at a cortical level has been proven to be a result of reduced, rather than increased excitability [16, 17], possibly due to low serotonin activity [18]. Interestingly, studies involving asymptomatic first-degree relatives of migraine patients also showed reduced habituation [19]. Thus, the habituation deficit could be a familial neurophysiologic abnormality that predisposes to migraine attacks.
It has been reported that interictal habituation failure in migraine patients is closely related to the length of time until the next attack [20]. In particular, reduced habituation was found in patients that suffered from a migraine attack after a short period of time from testing. The authors concluded that habituation deficiency is present mainly in the prodromal phase of migraine, possibly due to dopaminergic dysfunction.
Measurements during migraine attacks showed a reversal of the habituation deficit that was found interictally. These findings agree with results from previous studies [11]. A normalization of habituation during attacks has also been reported in CNV studies [13]. However, our results differ in the fact that in migraine patients R2” responses were recorded in significantly longer interstimulus intervals compared not only to migraineurs between attacks, but also in comparison to normal controls. This could be considered an indication of habituation mechanism hyperexcitability, although further investigation is needed to confirm these findings and establish the neurophysiologic basis.
In contrast to migraine, TTH evidently does not exhibit important alterations of the habituation process, as the patients shift from pain-free intervals to symptomatic periods. In general, TTH is often considered a condition that mainly involves the pericranial musculature [21], although a central inciting mechanism has been suspected in several cases. Exteroceptive suppression of temporalis muscle activity in TTH revealed dysfunction of brainstem inhibitory interneurons [22]. Our results did not show a similar defect, possibly due to different neuronal pathways involved. Previous studies typically reported normal blink reflex results, except for a headache duration-dependent prolongation of R1 that was noted in one case [10]. However, we could not confirm this finding. Normal habituation studies in TTH reflect unaltered brainstem function, although the existence of a central initiating process obviously cannot be excluded.
Using conventional blink reflex examination without habituation techniques could be useful in distinction of migraine from TTH, as we reported in our previous study [23]. During migraine attacks we observed a statistically significant reduction of R2 amplitude and area that was constant and reproducible. In perspective, heightened functionality of the habituation process during migraine attacks could be linked to brainstem interneuron suppression that results in decreased R2 responses. Our results did not confirm the presence of R2 latency abnormalities in migraine that were found in an earlier study [24].
Conclusion
This study showed for first time the elicitation of the late R2” response at different interstimulus intervals in migraine patients compared to the TTH and control groups. This could be considered an indication of habituation mechanism hyperexcitability, although further investigation need to confirm these findings and establish the neurophysiologic basis. Blink reflex studies can be used routinely as a non-evasive and inexpensive method for the evaluation of headache patients.
References
Bartsch T, Goadsby MD (2005) Anatomy and physiology of pain referral patterns in primary and cervicogenic headache disorders. Headache Curr 2(2):42–48
Moskowitz MA (1993) Neurogenic inflammation in the pathophysiology and treatment of migraine. Neurology 43(6 Suppl 3):S16–S20
Bolay H, Reuter U, Dunn AK et al (2002) Intrinsic brain activity triggers trigeminal meningeal afferents in a migraine model. Nat Med 8(2):136–142
Aktekin B, Yaltkaya K, Ozkaynak S et al (2001) Recovery cycle of the blink reflex and exteroceptive suppression of temporalis muscle activity in migraine and tension-type headache. Headache 41(2):142–149
Weiller C, May A, Limmroth V et al (1995) Brain stem activation in spontaneous human migraine attacks. Nat Med 1(7):658–660
Sandrini G, Proietti Cecchini A, Milanov I et al (2002) Electrophysiological evidence for trigeminal neuron sensitization in patients with migraine. Neurosci Lett 317(3):135–138
Shahani BT, Young RR (1972) Human orbicularis oculi reflexes. Neurology 22(2):149–154
Kimura J, Lyon LW (1972) Orbicularis oculi reflex in the Wallenberg syndrome: alteration of the late reflex by lesions of the spinal tract and nucleus of the trigeminal nerve. J Neurol Neurosurg Psychiatry 35(2):228–233
Kimura J (1973) Disorder of interneurons in Parkinsonism. The orbicularis oculi reflex to paired stimuli. Brain 96(1):87–96
Sand T, Zwart JA (1994) The blink reflex in chronic tension-type headache, migraine, and cervicogenic headache. Cephalalgia 14(6):447–450
Katsarava Z, Giffin N, Diener HC et al (2003) Abnormal habituation of ‘nociceptive’ blink reflex in migraine—evidence for increased excitability of trigeminal nociception. Cephalalgia 23(8):814–819
Headache Classification Committee of the International Headache Society (IHS) (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33:629–808
Kropp P, Gerber WD (1995) Contingent negative variation during migraine attack and interval: evidence for normalization of slow cortical potentials during the attack. Cephalalgia 15(2):123–128
Wang W, Timsit-Berthier M, Schoenen J (1996) Intensity dependence of auditory evoked potentials is pronounced in migraine: an indication of cortical potentiation and low serotonergic neurotransmission? Neurology 46(5):1404–1409
Afra J, Cecchini AP, De Pasqua V et al (1998) Visual evoked potentials during long periods of pattern-reversal stimulation in migraine. Brain 121(Pt 2):233–241
Bohotin V, Fumal A, Vandenheede M et al (2002) Effects of repetitive transcranial magnetic stimulation on visual evoked potentials in migraine. Brain 125(Pt 4):912–922
Coppola G, Vandenheede M, Di Clemente L et al (2005) Somatosensory evoked high-frequency oscillations reflecting thalamo-cortical activity are decreased in migraine patients between attacks. Brain 128(Pt 1):98–103
Ferrari MD, Saxena RR (1993) On serotonin and migraine: a clinical and pharmacological review. Cephalagia 13(3):151–165
Di Clemente L, Coppola G, Magis D et al (2007) Interictal habituation deficit of the nociceptive blink reflex: an endophenotypic marker for presymptomatic migraine? Brain 130(Pt 3):765–770
De Marinis M, Pujia A, Natale L et al (2003) Decreased habituation of the R2 component of the blink reflex in migraine patients. Clin Neurophysiol 114(5):889–893
Aaseth K, Grande RB, Lundqvist C et al (2014) Pericranial tenderness in chronic tension-type headache: the Akershus population based study of chronic headache. J Headache Pain 5(15):58
Schoenen J (1993) Exteroceptive suppression of temporalis muscle activity: methodological and physiological aspects. Cephalalgia 13:3–10
Avramidis TG, Podicoglou Anastasopoulos IE et al (1998) Blink reflex in migraine and tension-type headache. Headache 38(9):691–696
Bánk J, Bense E, Király C (1992) The blink reflex in migraine. Cephalalgia 12(5):289–292
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Avramidis, T., Bougea, A., Hadjigeorgiou, G. et al. Blink reflex habituation in migraine and chronic tension-type headache. Neurol Sci 38, 993–998 (2017). https://doi.org/10.1007/s10072-017-2885-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-017-2885-x