
Abstract
We studied factors associated with quality of life (QOL) among myasthenia gravis (MG) patients in two university hospitals in Thailand: Thammasat University (TU) and Khon Kaen University (KKU). Consecutive MG patients from an outpatient neurology clinic of both sites were enrolled and their clinical variables and QOL by the Short-Form 36 questionnaire were assessed. There were 31 and 40 subjects enrolled at TU and KKU, respectively. The mean values of the SF-36 score in seven dimensions were higher at the TU site. The significant factors between both sites were mean age, and numbers of participants with myasthenic symptoms and steroid treatment. The frequency of MG symptoms was the only factor associated with the SF-36 score (correlation coefficient −0.66, p value < 0.01). In conclusion, the frequency of MG symptoms might be the main factor that lowers QOL in MG patients in both physical and mental aspects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Myasthenia gravis (MG) is an autoimmune neuromuscular disease which can cause ocular or generalized weakness or even respiratory failure. There are some factors that might affect patients’ quality of life (QOL) both physically and mentally such as residual myasthenic symptoms, types of MG, and methods of treatment [1–4]. However, factors associated with poor QOL are still being debated.
The Short-Form 36-item questionnaire for health survey (SF-36) has been widely used to assess subjects’ quality of life. The tool has 36 questions that cover eight specific categories of physical and emotional domains [physical functioning (PF); physical role (RP); bodily pain (BP); general health (GH); vitality (VT); social functioning (SF); emotional role (RE); and mental health (MH)]. The first four categories are physical domain and the rest belongs to mental component. The SF-36 (version 2.0) has been translated to Thai version and validated to assess the QOL in Thai patients [5–7].
We conducted a prospective study to assess QOL among MG patients using the Thai version of SF-36 in an outpatient neurology clinic of two university hospitals in Thailand. The aim was to study the factors that correlated with QOL in MG patients in these two areas.
Materials and methods
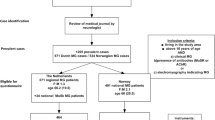
The study was conducted between 1 December 2006 and 31 May 2007, at Thammasat University (TU) Hospital, Pathumtani and Khon Kaen University (KKU), Khon Kaen. Patients were recruited from the outpatient neurology clinics of both hospitals. TU hospital provides both primary care and tertiary care to inhabitants in the lower central region of Thailand including Bangkok’s northern suburban area. KKU’s Srinagarind Hospital is a referral university hospital for the upper part of the Northeast of the country. The study protocol was approved by the institutional review board in both sites. Written informed consent was obtained from all patients.
Myasthenia gravis was diagnosed by patients’ clinical characteristics, positive results on the prostigmine test or the repetitive nerve stimulation test. The patient had to be at least 15 years of age and had no chronic diseases that may impact QOL such as diabetes mellitus, hypertension, heart disease, stroke, renal failure, chronic obstructive pulmonary disease or asthma.
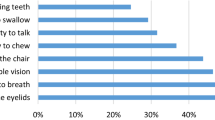
The patients were consecutively enrolled in the study from the clinics during the study period. We recorded the baseline characteristics and the QOL of all patients. Baseline characteristics included gender, age, marital status, education level, employment status, average income, type of MG, history of respiratory failure, history of hyperthyroidism, history of MG symptoms, and treatment. The history of MG symptoms indicated how often the patients experienced worsening of MG symptoms from baseline or had impact upon their daily routine. This factor was categorized as none, less than or more than or equal four times in the past month.
To obtain patient’s quality of life, a trained physician in each site conducted face-to-face interviews by using the Thai version SF-36 questionnaire. Patient data were entered into a prospective database for analysis. Statistical analyses were performed using SPSS version 10.0. The student t test and Fisher exact test were used to compare differences in the numbers and proportions between the two sites. Nonparametric analysis of correlation was conducted using Spearman’s rank correlation coefficient technique to assess the correlation between variables and the SF-36 score by site of enrollment. All significant and possible variables were included in the correlation analysis.
Results
There were 31 and 40 consecutive subjects enrolled at TU and KKU, respectively. The baseline characteristics at both sites were similar except the KKU site had more younger subjects and a higher number of myasthenic symptoms (Table 1). The mean values of the SF-36 score in seven categories, except ‘emotional well-being’ were higher at the TU site. All dimensions except ‘vitality’ were statistically different between sites (Table 2).
We found a significant correlation between the SF-36 score and frequency of myasthenic gravis symptoms (correlation coefficient −0.66, p value < 0.01) by subgroup analysis (TU site). Age, steroid treatment, immunosuppressive treatment, and thymectomy were included in the correlation analysis and found no significant correlation with QOL (p value > 0.05).
Discussion
Even though both study sites had different cultures and economic status, baseline characteristics of participating patients were mostly comparable. The SF-36 scores in almost all dimensions were significantly different between the two sites, except for ‘vitality’. This might be due to differences in the studied populations; subjects at the KKU site were younger and had more frequent MG symptoms (Table 1). Older individuals were known to have lower QOL. The lower QOL score of KKU site might be due to more frequent MG symptoms.
In the subgroup analysis at TU site, the frequency of MG symptoms was also shown to be the only factor that significantly correlated to the SF-36 score. The correlation coefficient of −0.66 indicates a negative correlation with good discrimination. Even though both groups had different mean age and numbers of patients with steroid therapy, both factors were not associated with QOL score.
The SF-36 values from KKU site were similar to previous data reported by Padua [2]. Most patients in the Padua study [2] were admitted due to a worsening of symptoms. These findings emphasized that the frequency of MG symptoms lowered QOL in MG patients in both physical and mental components.
Compared to other diseases, such as epilepsy and diabetes [8], MG patients tend to have a lower QOL in the physical dimension. Table 2 also showed that most scores in emotional dimension of participated subjects were lower than normal Thai subjects [9]. At the KKU site, both ‘physical’ and ‘emotional role’ scores were very low. By definition, both of these dimensions indicate the extent to which physical and emotional problems interfere with routine daily activities such as work, household chores, or school. From the patients’ perspective, myasthenia gravis symptoms have a huge impact on their physical and emotional functionality, probably related to culture and socioeconomic status.
In conclusion, the frequency of myasthenia gravis symptoms is the main factor that lowers QOL in MG patients.
References
Busch C, Machens A, Pichlmeier U, Emskötter T, Izbicki JR (1996) Long-term outcome and quality of life after thymectomy for myasthenia gravis. Ann Surg 224:225–232
Padua L, Evoli A, Aprile I, Caliandro P, Mazza S, Padua R, Tonali P (2001) Health related quality of life in patients with myasthenia gravis and the relationship between patient-oriented assessment and conventional measurements. Neurol Sci 22:363–369
Paul RH, Nash JM, Cohen RA, Gilchrist JM, Goldstein JM (2000) Quality of life and well-being of patients with myasthenia gravis. Muscle Nerve 24:512–516
Rostedt A, Padua L, Stalberg EV (2006) Correlation between regional myasthenic weakness and mental aspects of quality of life. Eur J Neurol 13:191–193
Tiamkao S, Sawanyawisuth K, Towanabut S, Visudhipun P, Thai QOL Epilepsy Investigators (2009) Seizure attacks while driving: quality of life in persons with epilepsy. Can J Neurol Sci 36:475–479
Lertwanich P, Praphruetkit T, Keyurapan E, Lamsam C, Kulthanan T (2008) Validity and reliability of Thai version of the International Knee Documentation Committee Subjective Knee Form. J Med Assoc Thai 91:1218–1225
Krittayaphong R, Bhuripanyo K, Raungratanaamporn O, Chotinaiwatarakul C, Chaowalit N, Punlee K, Kangkagate C, Chaithiraphan S (2000) Reliability of Thai version of SF-36 questionnaire for the evaluation of quality of life in cardiac patients. J Med Assoc Thai 83(S2):S130–S136
Hermann BP, Vickrey B, Hays RD, Cramer J, Devinsky O, Meador K, Perrine K, Myers LW, Ellison GW (1996) A comparison of health-related quality of life in patients with epilepsy, diabetes and multiple sclerosis. Epilepsy Res 25:113–118
Lim LL, Seubsman SA, Sleigh A (2008) Thai SF-36 health survey: tests of data quality, scaling assumptions, reliability and validity in healthy men and women. Health Qual Life Outcomes 6:52
Acknowledgments
We thank Thammasat University Hospital and Khon Kaen University Srinagarind Hospital for their support and Mr. Bryan Roderick Hamman for assistance with the English-language presentation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kulkantrakorn, K., Sawanyawisuth, K. & Tiamkao, S. Factors correlating quality of life in patients with myasthenia gravis. Neurol Sci 31, 571–573 (2010). https://doi.org/10.1007/s10072-010-0285-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-010-0285-6