
Abstract
Schilder’s disease, or myelinoclastic diffuse sclerosis, is a rare disorder characterised by an inflammatory white matter plaque of demyelination. Clinical signs and symptoms might be atypical for early multiple sclerosis and at imaging the lesion is easily taken for a brain tumour. Regardless of the use of Poser’s criteria for clinical diagnosis of Schilder’s disease proposed in 1986, diagnostic difficulties are still present, as evidenced by the many reported cases in the English literature revised (Pubmed indexed, period 1998–2008). It clearly emerges that neuroradiological features, observable in additional magnetic resonance sequences are crucial, besides the consideration of Poser’s criteria, in differentiating between demyelinating lesions and brain tumours. A 29-year-old female patient is presented, where a careful evaluation of both the clinical and radiological features, which might have been at a first glance misleadingly suggestive for a brain tumour, allowed non-invasive diagnosis of Schilder’s disease.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Schilder’s myelinoclastic diffuse sclerosis is a rare acute or subacute demyelinating disorder diagnosed mainly in young patients [1]. Schilder first described the disease in 1912 as diffuse sclerosis [2]. For 80 years after this first report there has been nosological confusion on the use of this eponym. In 1986 Poser et al. [3] established restrictive diagnostic criteria for non-invasive diagnosis of Schilder’s disease. These criteria can be resumed as follows: (1) clinical symptoms and signs atypical for an early course of multiple sclerosis (MS)-like bilateral optic nerve involvement, signs of intracranial hypertension, aphasia, psychiatric manifestation, (2) a normal cerebrospinal fluid (CSF) or atypical for MS, (3) one or two symmetrical bilateral plaques measuring at least 3 × 2 cm and involving the centrum semiovale of the cerebral hemispheres on brain scans, (4) no fever, viral or mycoplasmal infection, or vaccination preceding the symptomatology; and (5) a normal serum concentration of very long-chain fatty acids.
Despite the Poser’s clinical criteria, the differential diagnosis with brain tumours of these large demyelinating brain lesions is often difficult [4, 5] and invasive procedures are still the gold standard for diagnosis. Unfortunately also biopsy is often unsuccessful: in 19% of the cases described in the revised literature, biopsies were not diagnostic.
Careful analysis of our patient and of other reported cases of Schilder’s disease, evidence the helpfulness of some specific neuroradiological considerations when getting through the differential diagnostics. The necessity, but also the feasibility of non-invasive diagnosis is discussed.
Literature review
English literature has been reviewed, published in the last 10 years, between 1998 and 2008. MEDLINE on the PubMed server was searched using the combination of the following terms: “Schilder’s disease OR myelinoclastic diffuse sclerosis OR tumefactive demyelination OR monofocal inflammatory demyelination OR pseudotumoral demyelination NOT alpers NOT balo NOT balo’s NOT pelizaeus merzbacher NOT canavan NOT alexander’s disease NOT alexander NOT cadasil NOT temporal lobe epilepsy NOT leukodystrophy NOT leukoencephalopathy NOT rasmussen NOT mitochondrial NOT muscular dystrophy NOT cerebrovascular disease NOT glial”. Of the 79 results, only those case reports were selected (selection was performed by two authors independently) where either the definition “Schilder’s disease” or at least 3 of Poser’s criteria were mentioned and fulfilled. Following these criteria, 25 papers [6–30] including a total of 33 patients with Schilder’s disease, 34 with the present reported case, were analysed for clinical and neuroradiological features, modality of diagnosis and outcome at follow-up.
The clinical and diagnostic aspects of the 34 described cases are summarised in Table 1, while Table 2 shows the described neuroradiological features of the same cases.
Analysis
Age, follow-up and clinical presentation
Amongst the 34 cases described the eponym “Schilder’s disease” was not used in eight cases, and the term “tumefactive demyelinating disease” or “monofocal inflammatory demyelination” was used by the authors. In the series analysed the average age of presentation was 23 ± 18 (SD) years, median 18 years and in 62% of the cases the patient was female. Follow-up data is not mentioned in 3 of 34 patients. In the remaining 31 cases, the average time is 24 ± 34 (SD) months, the median 12 months, but in 12 subjects follow-up is shorter than 7 months. In 9% of cases symptoms at presentation were not atypical for MS. However, this non-atypical clinical presentation was not a predictor for the progression of “Schilder’s disease” towards MS: in fact in all patients where follow-up documented a progression towards MS (5/34), clinical presentation had been atypical. Nevertheless, follow-up time in many presented cases is too short to document conversion towards MS.
Outcome and prognosis
From the literature, it emerges that the course of the disease is not always benign: 16/31 (52%) patients improved, one patient remained stable, in 8/31 (26%) some neurological symptoms persisted despite the improvement, further, one patient had two exacerbations, one had a rapid progression, in one case new lesions were detected afterwards, and one patient died (3%) because steroid therapy was complicated by sepsis. In five patients (16%), the disease progressed towards MS. The occurrence of seizures is mentioned in 5/31 cases (16%), where follow-up is notified.
Diagnosis I: Poser’s criteria
Not all reports exactly specify the fulfilment of each of Poser’s criteria for non-invasive diagnosis: atypical onset was present in 31/34 (91%) of patients, CSF analysis is reported for 27/34 (79%) and in one patient oligoclonal bands were detected. Further, the absence of infection is mentioned in 26/34 (76%) cases; one patient harboured TBC. Long fatty acids investigations are mentioned only for 19/56 (63%) of patients. Only in few cases (12%) normal adrenal function is explicitly mentioned, while in 34% normal blood tests are reported. The lesion (demyelinating plaque) was bilateral in 32% of cases, monolateral in the others—two of these patients had two lesions on the same side (detailed description of clinical features of the cases analysed is provided in Table 1).
Diagnosis II: Neuroradiology
Brain CT scans in the described cases of Schilder’s disease revealed subcortical, initially hypodense lesions, except for three patients, where the first CT scan was negative. On brain magnetic resonance (MR), lesions appeared hypodense on T1 sequence and hyperintense on T2. The presence of mass effect is usually inconsistent with the lesion size and has been shown or described in 9/34 (26%) patients. Contrast enhancement of the lesion margins is only present during the acute inflammatory stage in white matter inflammatory diseases. According to some authors, the open ring contrast enhancement is highly specific for brain demyelination [31]. In the series analysed, contrast enhancement is mentioned or shown in 30/34 cases. Amongst these, the classic open ring can clearly be recognised in 63%, although it was mentioned only in 20/34 (59%) of the cases. Further, in 5/30 (17%) the enhancement ring was more a patchy one, in 4/30 (13%) there was a patchy lesion. In only two patients (7%) there had been no enhancement and this might depend on the time point where imaging was performed.
In the revised literature seven cases of Schilder’s disease studied with magnetic resonance spectroscopy (MRS) are described in addition to ours [10, 16, 18, 21, 23, 24, 28]. The N-acetylaspartate (NAA) peak on MRS is always decreased or slightly decreased but present, as is the N-acetylaspartate/creatine (NAA/Cr) ratio, choline (Cho) and choline/creatine (Cho/Cr) ratio are always increased, lactate (Lac) is described as increased, and some lactate–lipid (Lac-Lip) complexes are mentioned.
Other described neuroradiological features are: increased signal on fluid attenuated inversion recovery (FLAIR) sequence, increased apparent diffusion coefficient (ADC), no thallium 201 uptake at SPECT and abnormal elevation of the glutamate/glutamine peaks at short-echo time MRS (detailed description of neuroradiological features of the cases analyses is provided in Table 2).
Diagnosis III: Neuropathology
Because Schilder’s disease is very rare and its neuroradiological features frequently mimic a brain tumour, diagnosis might become critical and relies on neuropathological analysis. In the revised literature, 65% of cases were in fact diagnosed by means of an invasive approach. Amongst these, 13 patients underwent biopsy; in two the procedure had to be repeated (the first diagnosis was of normal brain tissue in one case and of astrocytoma in the other case), in a further case the histology sections were revised recognising a demyelinating inflammatory disease after a first interpretation of glioblastoma, and even the initiation of chemotherapy. However, even a surgical specimen had been initially misinterpreted as glioblastoma. Out of 11 patients that underwent craniotomy, mass effect seemed to be present only in four. One patient underwent both biopsy and craniotomy.
Illustrative case
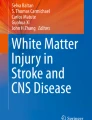
We here report the case of 29-year-old woman where non-invasive diagnosis of Schilder’s disease has been feasible by the neuroradiological analyisis. The patient had been admitted to an emergency ward for hypoesthesia, paresthesia and movement impairment, initially involving the lower left limb and successively also the upper left limb, the trunk and the left half of the face. These symptoms had evolved progressively during the 10 previous days. Clinical history was relevant for psoriasis and for an uncomplicated delivery a few months before. In the emergency ward, the brain CT evidenced an intraparenchymal right parietal hypodense lesion, with maximum diameters of 4.5 × 4 × 3 cm3 further characterised by hyperdense spots at the margins, little mass effect on the brain sulci, and signs of perilesional oedema towards the trigonal homolateral area. Successive CSF chemical-, physical-, microbiological analyses, oligoclonal bands and tumour cell search were all negative. Blood examination including very long fatty acid plasma concentration and adrenal function were normal. Further, an MRI was performed, using T1, T2, FLAIR sequences, DWI, MRS and T1 sequences after contrast administration (Figs. 1, 2a). In all sequences, an altered signal in the anterior and inferior portions of the lesion was detected. In the same region, a contrast enhancement (open ring sign) was evident after gadolinium administration. In the core of the lesion, ADC appeared increased. On multivoxel MRS (Fig. 3a) the lesion was throughout characterised by an increased Cho peak and by the absence of Lip. Cho and Cho/Cr ratio were particularly increased in the anterior, contrast-enhancing portion of the lesion; the NAA peak was reduced with an increase and inversion of the Cho/NAA ratio. In the spectrum obtained with single volume technique a Lac peak was evident (Fig. 3b). On the basis of these images, the neuroradiologist ruled out an abscess, an ischaemic lesion, and a metastatic tumour and the patient was treated with steroids. Owing to the suspicion of a brain tumour, a neurosurgical consult request was forwarded. After 2 weeks, while re-evaluating the patient prior to surgery, a brain MR was repeated (Fig. 2b) which showed the shrinkage of the cystic portion of the lesion and the almost complete fading of the ring enhancement.

MRI study in the acute phase: T2-weighted axial view (a), T1 contrast-enhanced, axial (b), sagittal (c) and coronal (d) views. The MRI study shows an intracranial subcortical lesion in the right parietal lobe, hypointense in T1, hyperintense in T2, associated with a relatively small amount of oedema

Comparison between the first (a) and the second MRI examination (b) taken 5 weeks later. Axial T1 contrast-enhanced, DWI double echo (PD and T2-weighted and FLAIR sequences (the FLAIR control scan was available only in the coronal view). The progressive reduction of the cystic portion of the lesion is detectable in the second examination

a Multivoxel proton magnetic resonance spectrometry (H-MRS). The lesion is characterised by an increase in choline to creatine ratio (Cho–Cr) and choline to N-acetylaspartate ratio (Cho-NAA). The Cho-NAA ratio is higher in portion of the lesion with signs of BBB breakdown. A reduction of N-acetylaspartate (NAA) peak is also detectable. b In the cystic portion of the lesion, a lactate peak is better seen with single voxel MRS (dotted circle). A peak in the glutamate/glutamine spectral region seems to be detectable (arrow) despite the MRS had been performed with a long echo time
Considering the fulfilment of Poser’s clinical criteria and imaging characteristics strongly suggestive for a large demyelinating plaque, Schilder’s disease was diagnosed and the patient was continued on corticosteroid therapy. After two or more weeks of treatment, the patient improved clinically (Fig. 4). Brain MR showed a reduction of contrast enhancement and the absence of mass effect. After 4 weeks, the cystic component was reduced and the lesion showed no contrast enhancement on brain MR (Figs. 2b, 4). During that time, the patient was asymptomatic. Steroids were maintained for a further month. At 18 months of follow-up, MR scans (Figs.2b, 4) showed the stability of the lesion and the clinical examination was negative for neurological findings. The good clinical and neuroradiological response to steroids at follow-up confirmed further the diagnosis of Schilder’s disease, however, histological analyses were not performed, and even in our case, diagnosis occurred not at the first MRI study, but at the second.

MRI follow-up: coronal T1 contrast-enhanced (a), and axial proton density (b), at different time points: before treatment, at 2 weeks of steroids, at 4 weeks of steroids and at follow-up after 18 months
Discussion
Despite the Poser’s [3] well-established criteria for non-invasive diagnosis of Schilder’s disease, diverse clinical cases have been reported afterwards, where diagnosis was only possible through neuropathological examination of brain biopsies. In fact, clinical and neuroradiological features of myelinoclastic diffuse sclerosis can be often misinterpreted leading to diagnose a brain tumour. A critical point is in fact that Poser’s diagnostic criteria for non-invasive diagnosis address to suspect Schilder’s disease, however, they cannot help to rule out a brain tumour. Therefore, a thorough analysis of neuroradiological features is of crucial support.
Considering the risks associated with craniotomy and the smaller but still existing risks associated with biopsy (3.5% symptomatic haemorrhage [32]) together with the possibility of a misleading diagnosis at biopsy (three cases in our review), it is worth to closer consider the potential of non-invasive diagnosis on the mere basis of clinical and neuroradiological features.
We suggest the following neuroradiological analysis for possibly avoiding invasive diagnostic manoeuvres in Schilder’s disease diagnostics. An increased ADC in the core of the lesion can help to rule out the presence of an abscess, because pus would give a reduced ADC signal and appear as hyperintensity on DWI [33] and the same is true for ischaemic lesions [34]. On MRS, the increased Cho peak is a sign of augmented cell density or turnover. The reduced NAA peak is attributable to a reduction in the number of normally functioning neurons and axons due to injury or substitution through infiltration. Despite evidence of injury on morphologic studies, a peak of NAA, even if reduced, is in favour of the non-metastatic nature of the cyst-like lesion, because non-encephalic tissue would not express NAA. Lac is a product of anaerobic glycolysis, and since an abscess could be ruled out as described above, this increase in Lac might be due to active macrophages attracted within a site of inflammation. At this point ischaemia, abscess and metastasis can be ruled out. The dilemma between primary brain tumour and demyelinating plaque remains, since, as discussed by other authors [18, 28, 35], MRS based on the Cho, Cr, NAA, Lac and Lipids seems not to be reliable to this purpose, given the overlap in increased Cho/Cr ratio, decreased NAA/Cr ratio and the non-specific presence of Lac and Lip both in both cases. Two further imaging techniques might support the process of differential diagnostics. As reminded by Tsui et al. [36] since, according to some authors [37] blood vessels in demyelination are normal, while neovascularisation phenomena are typically present in brain tumours, perfusion discriminates between these two entities: on perfusion-weighted imaging there is no increase in relative cerebral blood volume (rCBV) in demyelination. This was also the case in our patient, as we noticed by retrospectively reviewing MR studies (perfusion shown in Fig. 5). A further interesting imaging tool for this final differential diagnostics has been recently presented by Cianfoni et al. [28]: tumefactive lesions present in contrast to neoplasms an abnormal elevation of the glutamate/glutamine peak using short-echo time proton MRS. In our case, despite MRS had been performed with a long echo time, it may be retrospectively possible to identify a peak in the spectral region of glutamate/glutamine (Fig. 3b). This peak has never been described in patients with lymphoma so far.

At perfusion-weighted imaging (PWI), the lesion was markedly hypoperfused, compared with the contralateral unaffected white matter
On the basis of these revised literature cases, we would like to propose non-invasive diagnosis for a demyelinating tumour-like plaque when following conditions are fulfilled: no signs of intracranial hypertension, presence of one or two subcortical cyst-like lesions with eventually open ring sign at CT/MR, exclusion of ischaemia, abscess and metastasis by classical neuroradiological means and further of primary neoplasm by means of perfusion MR and consideration of abnormal glutamate/glutamine elevation on short-echo time MRS. Schilder’s disease can be defined at this point if Poser’s diagnostic criteria are fulfilled.
Because cases of Schilder’s disease are rare, we would like to coordinate a multicentric case collection by inviting you to send following data on your patients to the corresponding author’s address: all items mentioned in Tables 1 and 2 should be addressed, further the following images in jpeg might be enclosed: T1 with and without contrast, T2, FLAIR, DWI, perfusion and MRS, possibly indicating the glutamate/glutamine peak, and finally the follow-up a month after steroids and at 18 months. Histopathological consult, where diagnosis occurred invasively might also be included.
References
Lhemitte F, Escourolle R, Haw J, Gray F, Serdaru M, Lyon-Caen D (1981) Les formes cavitaires de la sclérose en plaques et de la maladie de Schilder. Rev Neurol 137:589–600
Schilder P (1912) Zur Kenntnis der sogenannten diffusen Sklerose. Z Ges Neurol Psychiat 10:1–60
Poser CM, Goutières F, Carpentier MA, Aicardi J (1986) Schilder’s myelinoclastic diffuse sclerosis. Pediatrics 77:107–112
Kaylan-Raman UP, Garwaki DJ, Elwood PW (1987) Demyelinating disease of corpus callosum presenting as glioma on magnetic resonance scan: a case documented with pathological findings. Neurosurgery 21:247–250
Rieth KG, Di Chiro G, Cromwell LD, Mc Keever PE, Kornblith PL, Kufta CV, Pleet AB (1981) Primary demyelinating disease simulating glioma of corpus callosum. J Neurosurg 55:620–624
Pretorius ML, Loock DB, Ravenscroft A, Schoenab JF (1998) Demyelinating disease of Schilder type in three young South African children: dramatic response to corticosteroids. J Child Neurol 13:197–201
Garell PC, Menezes AH, Baumbach G, Moore SA, Nelson G, Mathews K, Afifi AK (1998) Presentation, management and follow-up of Schilder’s disease. Pediatr Neurosurg 29:86–91
Leuzzi V, Lyon G, Cilio MR, Pedespan JM, Fontan D, Chateil JF, Vital A (1999) Childhood demyelinating diseases with a prolonged remitting course and their relation to Schilder’s disease: report of two cases. J Neurol Neurosurg Psychiatry 66:407–408
Fitzgerald MJ, Coleman LT (2000) Recurrent myelinoclastic diffuse sclerosis: a case report of a child with Schilder’s variant of multiple sclerosis. Pediatr Radiol 30:861–865
Iñiguez C, Pascual LF, Ramón y Cajal S, Fayed N, Morales-Asín F (2000) Transitional multiple sclerosis (Schilder’s disease): a case report. J Neurol 247:974–976
Afifi AK, Follett KA, Greenlee J, Scott WE, Moore SA (2001) Optic neuritis: a novel presentation of Schilder’s disease. J Child Neurol 16:693–696
Censori B, Agostinis C, Partziguian T, Gazzaniga G, Biroli F, Mamoli A (2001) Large demyelinating brain lesion mimicking a herniating tumor. Neurol Sci 22:325–329
Heyman D, Delhaye M, Fournier D, Mercier P, Rousselet MC, Menei P (2001) Pseudotumoral demyelination: a diagnosis pitfall (report of three cases). J Neurooncol 54:71–76
Kiernan MC, Vonau M, Bullitt PR, Tohver E, Milder DG (2001) Butterfly lesion of the corpus callosum due to Schilder’s disease. J Clin Neurosci 8:367–369
Gutrecht JA, Berger JR, Jones RH Jr, Mancall AC (2002) Monofocal acute inflammatory demyelination (MAID): a unique disorder simulating brain neoplasm. South Med J 95:1180–1186
Khoshyomn S, Braff SP, Penar PL (2002) Tumefactive multiple sclerosis plaque. J Neurol Neurosurg Psychiatry 73:85
Kotil K, Kalayci M, Koseoglu T, Tugrul A (2002) Myelinoclastic diffuse sclerosis (Schilder’s disease) report of a case and review of the literature. Br J Neurosurg 16:516–519
Law M, Meltzer DE, Cha S (2002) Spectroscopic magnetic resonance imaging of a tumefactive demyelinating lesion. Neuroradiology 44:986–989
Nejat F, Eftekhar B (2002) Decompressive aspiration in myelinoclastic diffuse sclerosis of Schilder disease. J Neurosurg 97:1447–1449
Kurul S, Cakmakçi H, Dirik E, Kovanlikaya A (2003) Schilder’s disease: case study with serial neuroimaging. J Child Neurol 18:58–61
Obara S, Takeshima H, Awa R, Yonezawa H, Oyoshi T, Nagayama T, Hirano H, Niiro M, Kuratsu J (2003) Tumefactive myelinoclastic diffuse sclerosis: case report. Neurol Med Chir (Tokyo) 43:563–566
Sastre-Garriga J, Rovira A, Río J, Tintoré M, Grivé E, Montalban X (2003) Clinically definite multiple sclerosis after radiological Schilder-like onset. J Neurol 250:871–873
Tan HM, Chan LL, Chuah KL, Goh NS, Tang KK (2004) Monophasic, solitary tumefactive demyelinating lesion: neuroimaging features and neuropathological diagnosis. Br J Radiol 77:153–156
Anderson RC, Connolly ES Jr, Komotar RJ, Mack WJ, McKhann GM, Van Orman CB, Hedlund G, Proctor KA, Townsend JJ, Walker ML (2005) Clinicopathological review: tumefactive demyelination in a 12-year-old girl. Neurosurgery 56:1051–1057
Akimoto J, Nakajima N, Saida A, Haraoka J, Kudo M (2006) Monofocal acute inflammatory demyelination manifesting as open ring sign: case report. Neurol Med Chir (Tokyo) 46:353–357
Miyamoto N, Kagohashi M, Nishioka K, Fujishima K, Kitada T, Tomita Y, Mori K, Maeda M, Wada R, Matsumoto M, Mori H, Mizuno Y, Okuma Y (2006) An autopsy case of Schilder’s variant of multiple sclerosis (Schilder’s disease). Eur Neurol 55:103–107
Ragel BT, Fassett DR, Baringer JR, Browd SR, Dailey AT (2006) Decompressive hemicraniectomy for tumefactive demyelination with transtentorial herniation: observation. Surg Neurol 65:582–583
Cianfoni A, Niku S, Imbesi SG (2007) Metabolite findings in tumefactive demyelinating lesions utilizing short echo time proton magnetic resonance spectroscopy. AJNR Am J Neuroradiol 28:272–277
Yilmaz Y, Kocaman C, Karabagli H, Ozek M (2008) Is the brain biopsy obligatory or not for the diagnosis of Schilder’s disease? Review of the literature. Childs Nerv Syst 24:3–6
Riva D, Chiapparini L, Pollo B, Balestrini MR, Massimino M, Milani N (2008) A case of pediatric tumefactive demyelinating lesion misdiagnosed and treated as glioblastoma. J Child Neurol 23:944–947
Masdeu JC, Quinto C, Olivera C, Tenner M, Leslie D, Visintainer P (2000) Open-ring imaging sign: highly specific for atypical brain demyelination. Neurology 54:1427–1433
Grossman R, Sadetzki S, Spiegelmann R, Ram Z (2005) Haemorrhagic complications and the incidence of asymptomatic bleeding associated with stereotactic brain biopsies. Acta Neurochir (Wien) 147:627–631
Reddy JS, Mishra AM, Behari S, Husain M, Gupta V, Rastogi M, Gupta RK (2006) The role of diffusion-weighted imaging in the differential diagnosis of intracranial cystic mass lesions: a report of 147 lesions. Surg Neurol 66:246–250
van Everdingen KJ, van der Grond J, Kappelle LJ, Ramos LM, Mali WP (1998) Diffusion-weighted magnetic resonance imaging in acute stroke. Stroke 29:1783–1790
Saindane AM, Cha S, Law M, Xue X, Knopp EA, Zagzag D (2002) Proton MR spectroscopy of tumefactive demyelinating lesions. AJNR Am J Neuroradiol 23:1378–1386
Tsui EY, Leung WH, Chan JH, Cheung YK, Ng SH (2002) Tumefactive demyelinating lesions by combined perfusion-weighted and diffusion weighted imaging. Comput Med Imaging Graph 26:343–346
Cha S, Pierce S, Knopp EA, Johnson G, Yang C, Ton A, Litt AW, Zagzag D (2001) Dynamic contrast-enhanced T2*-weighted MR imaging of tumefactive demyelinating lesions. AJNR Am J Neuroradiol 22:1109–1116
Acknowledgments
Thanks to Marco Bacigaluppi M.D. for insightful advice and suggestions during the development of this paper and thanks all colleagues who have contributed to the care of our patient.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bacigaluppi, S., Polonara, G., Zavanone, M.L. et al. Schilder’s disease: non-invasive diagnosis?. Neurol Sci 30, 421–430 (2009). https://doi.org/10.1007/s10072-009-0113-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-009-0113-z