
Abstract
Breathing disturbances in Rett syndrome were reported almost entirely during wakefulness, with normal respiration during sleep. We studied a case of a proven MECP2 mutation in a girl, whose videopolygraphic and polysomnographic monitoring suggested the evidence of central apnoeas not only during awake, but also during sleep. Apart from prevalent awake respiratory dysfunction, central apnoeas in Rett syndrome may be also present during sleep.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Supportive clinical criteria necessary for diagnosing Rett syndrome (RTT) include breathing disturbances during awake [1], characterised by hypoventilation, apnoea, breath-holding spells, episodic hyperventilation, Valsalva manoeuvres, and air swallowing (bloating) [2, 3]. The abnormal cardiorespiratory center in the brainstem and involvement of the serotonergic system were demonstrated in RTT [2], and the breathing dysrhythmias during awake may suggest poor integration at higher centres such as the hypothalamus and the limbic cortex, where “wakefulness drive” of breathing is modulated [2]. Of seven patients with epilepsy and RTT with a proven MECP2 mutation, we report a case whose videopolygraphic and polysomnographic monitoring suggested the evidence of central apnoeas not only during awake, but also during sleep.
Case report
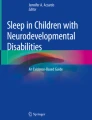
A case of a 3-year-old girl with psychomotor development normal until age 8 months, but then progress stagnated with a rapid loss of social interaction and communicative skills. She was diagnosed as having RTT with a truncating nonsense mutation in the MECP2 gene. At the age of 2, the girl was admitted to our Epilepsy Center because she experienced paroxysmal episodes of hyperventilation and apnoea misdiagnosed as epileptic seizures. Recording parameters of videopolygraphy included EEG (electrodes placed according to the 10–20 International system with bipolar montage); electromyogram from submental muscle, the right deltoid muscle, the right and left flexor and extensor muscles of the hand and both muscles tibialis anterior; EKG; oronasal (monitored with a thermistor), thoracic and abdominal respiration (monitored with a strain gauge); electrooculogram; oxygen saturation, heart rate and pulse. The AASM manual for the scoring of sleep and associated events has been used. Interictal EEG showed bilateral spikes or sharp waves discharged, more prominent during 2–3 NREM sleep. The transition from wakefulness to sleep included repetitive central sleep apnoeas with some awakenings that resulted in a 30-min period before consolidated sleep was achieved. She continued to have central apnoeas throughout the night, and not exclusively during transitions from wakefulness to sleep. No snoring was heard; daytime sleepiness and anatomical conditions causing upper airway obstruction (obesity or craniofacial abnormalities such as retrognathia or micrognathia) were ruled out. There were a total of 194 per respiratory events through the night with an apnoea plus hypopnea index of 40.1 events per hour of sleep, 40% of which were central apnoeas. The mean central apnoea duration was 14.2 s, while the longest central apnoea was 33.5 s. Oxygen desaturations occurred during sleep to a nadir of 89%, while oxygen desaturation index was 10.3. Brief paroxysmal episodes of central apnoea appeared also while awake, with a baseline waking oxygen saturation of 99% (see Fig. 1). Other types of respiratory disturbances were characterised by hypopneas. Brain MRI was normal.

Polygraphy during wakefulness (left) and sleep (right) (EEG. EMG: R., L. Delt right and left deltoid muscles, R., L. Flex. right and left flexor muscles of the hand, R., L. Ext. right and left extensor muscles of the hand, R, L. Tib. Ant. right and left muscles tibialis anterior. EKG. Flow: oronasal respiration, Thorax thoracic respiration, Abd abdominal respiration, SaO2 oxygen saturation, HR heart frequency, Pulse). During wakefulness (left), brief central apnoea without desaturation. During 1–2 NREM sleep, central apnoea with oxygen desaturation (also 89%); concomitant bilateral spikes and sharp waves discharged and erratic myoclonia
Discussion
Breathing disturbances in RTT were reported almost entirely during wakefulness [4–6], with normal respiration during sleep. Recently, Rodin et al. [3] monitored cardiorespiratory function in 12 RTT girls in their home environment for a week and all patients exhibited respiratory dysfunction in the form of apnoea, hypoventilation or shallow breathing in wakefulness, but also sleep (the type of apnoea—central, obstructive, mixed—was not specified). Similarly, Weese-Mayer et al. [7] determined that, although the breathing and heart rate appeared more regular during the night compared with the day, 47 girls with RTT in their home environment demonstrated apparent nocturnal irregularities. Although these patients were studied by means of electrodes that recorded only the depth and frequency of respiratory movements, nevertheless it was evident that the breathing disturbances were not restricted to awake. Videopolygraphic–polysomnographic monitoring is essential when a breathing disturbances is suspected, and the type of apnoea can be differentiated, as well as the degree of hypoxemia and sleep disturbance assessed. Our case exemplify the interface between awake and sleep breathing disturbances in RTT and showed that, apart from prevalent awake respiratory dysfunction, there are also rare cases with central apnoea or other disturbances during sleep. In our case, the breathing dysrhythmias from the wake–sleep transition (persisting throughout the sleep) may suggest a instability of central respiratory drive with a congenital dysfunction of central chemoreceptors or respiratory integrative systems of the brainstem, such as in idiopathic central sleep apnoea. In fact, under normal physiological control, respiration is stimulated when the PaCO2 level increases, and, while sleeping, a higher level of CO2 must accumulate before the respiratory drive is stimulated. At sleep onset, breathing ceases for a few seconds until enough CO2 accumulates to stimulate the respiratory drive, at which point breathing resumes. Normally, when sleep is maintained, the PaCO2 remains at a higher level required to stimulate respiratory drive during sleep. However, when there are multiple shifts between wakefulness and sleep, the result is periodic breathing due to the central apnoea, which occurs with each new episode of sleep onset. Central apnoea/periodic breathing at wake–sleep transition is common in paediatric polysomnograms, but also in normal subjects of all ages, due to the differences in apnoeic threshold between wakefulness and sleep. However, these normal events rarely reach 10 s in length, and only one breath or two breaths are inhibited. Owing to the short duration, physiological oxygen stores are not exhausted, and oxygen saturation is minimally affected [8]. In contrast, in our patient the mean central apnoea duration was 14.2 s (while the longest central apnoea was 33.5 s) with concomitant oxygen desaturations; there were pathological central apnoeas at wake–sleep transition and throughout the night. Finally, central apnoeas, usually pathological, are sometimes seen as a secondary finding in patients with obstructive sleep apnoea, but its exclusion in our RTT patient may strengthen the evidence that the central apnoeas were secondary to RTT, such as in patients with other cerebral neurological disease [9]. Although we report only a single case, nevertheless, the information of central sleep apnoea, unusual but critical aspect, may contribute to characterise some consequences of disease and, therefore, central sleep apnoea in RRT should be confirmed in larger series by means of continuous videopolygraphic, polysomnographic monitoring.
References
Moser SJ, Weber P, Lutschg J (2007) Rett syndrome: clinical and electrophysiologic aspects. Pediatr Neurol 36:95–100
Julu POO et al (2001) Characterisation of breathing and associated central autonomic dysfunction in the Rett disorder. Arch Dis Child 85:29–37
Rodin M, Fernell E, Eriksson M, Albage M, Lagercrantz H, Katz-Salomon M (2007) Disturbances in cardiorespiratory function during day and night in Rett syndrome. Pediatr Neurol 37:338–344
Glaze DG, Frost JD, Zoghbi HY, Percy AK (1987) Rett syndrome: characterization of respiratory patterns and sleep. Ann Neurol 21:377–382
Marcus CL et al (1994) Polysomnographic characteristics of patients with Rett syndrome. J Pediatr 125:218–224
Schluter B, Aguigah G, Buschatz D, Trowitzsch E, Aksu F (1995) Polysomnographic recordings of respiratory disturbances in Rett syndrome. J Sleep Res 4:203–207
De Weese-Mayer, Lieske SP, Boothby CM, Kenny AS, Bennett HL, Ramirez JM (2008) Autonomic dysregulation in young girls with Rett syndrome during night time in-home recordings. Pediatr Pulmonol 43(11):1045–1060
Sullivan CE (1981) Breathing in sleep. In: Orem J, Barnes CD (eds) Physiology in sleep. Academic Press, New York
Banno K, Kryger MH (2007) Sleep apnoea: clinical investigations in humans. Sleep Med 8:400–426
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
d’Orsi, G., Demaio, V., Scarpelli, F. et al. Central sleep apnoea in Rett syndrome. Neurol Sci 30, 389–391 (2009). https://doi.org/10.1007/s10072-009-0108-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-009-0108-9