
Abstract
Introduction
Kikuchi-Fujimoto disease (KFD) is a rare benign lymphadenitis that mainly involves cervical lymph nodes of young Asian women with unknown etiology. Recently, we experienced a case of KFD found with Torque teno virus/Torque teno-like mini virus (TTV/TTMV) from a 26-year-old woman. TTV/TTMV is a genus of Circoviridae that causes necrotizing lymphadenitis in pigs, which shares the key histologic finding of KFD. The purpose of this study is to investigate the pathogenic role of TTV/TTMV in KFD by quantitative polymerase chain reaction (qPCR) analysis.
Method
We performed two-step qPCR specific to TTV/TTMV with formalin-fixed paraffin-embedded tissue of sequentially selected 100 KFD patients and 50 randomly selected, matched normal controls. Consequent direct sequencing was done for confirmation with PCR products.
Results
PCR amplification of TTV and TTMV was found in a significantly higher proportion in KFDs than normal controls (TTV, 85% vs. 18%, p < 0.000; TTMV, 91% vs. 24%, p < 0.000). After the sequencing, KFD samples showed more sequence matching than control samples for TTMV (94% vs. 30%, p < 0.000).
Conclusion
This finding strongly suggests the possible implication of TTV/TTMV in the pathogenesis of KFD. Animal or in vivo experimental design should be followed in the future.
Key Points • Kikuchi-Fujimoto disease (KFD) is rare and its etiology is still unclear. • Torque teno/Torque teno-like minivirus (TTV/TTMV) is a recently introduced virus in the Circoviridae family that causes necrotizing lymphadenitis in pigs, histologically similar to KFD. • We discovered the significantly increased TTV/TTMV viral loads in the KFD patients than normal controls, which implicates TTV/TTMV in the pathogenesis of KFD. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Kikuchi-Fujimoto disease (KFD) is a relatively rare benign lymphadenitis that mainly involves the cervical lymph nodes of young Asian women, characterized by histologic feature of histiocytic necrotizing lymphadenitis [1, 2]. It was first described by Kikuchi and Fujimoto et al. independently in 1972 and its etiology has remained unknown [3, 4]. Because of the clinicopathologic features of KFD, febrile symptoms, and necrotizing histiocytosis, simulating infectious disease, the association of various infectious agents, such as Epstein–Barr virus (EBV), has been raised [5]. However, in our previous meta-analysis using 41 studies, none of the most pathogenic microorganisms in humans, including human herpesviruses (HHV) (herpes simplex virus types 1 and 2, varicella zoster virus, EBV, cytomegalovirus, HHV types 6, 7, and 8), human papillomavirus (HPV), parvovirus B19, hepatitis B virus (HBV), and human T-lymphotropic virus 1 (HTLV-1), were related to KFD [6].
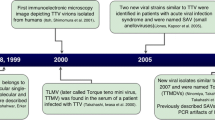
We hypothesized that if there were any microorganisms that can cause similar histologic features to that of KFD in another animal hosts, they would be also pathogenetically associated with KFD in humans. With this reasonable suspicion, we searched in the literature to find the potential agent. As a result, we found out that porcine circovirus (PCV), primarily known as a cause of postweaning multisystemic wasting syndrome (PMWS), can cause necrotizing lymphadenitis in pigs that are very similar to the histologic features of KFD [7, 8]. In addition, we found out that Torque teno virus/Torque teno-like minivirus (TTV/TTMV), first found in Japanese hepatitis patient (non-A to G) in 1997, is initially placed under the family Circoviridae that can infect human host [9, 10]. TTV/TTMV, also known as a transfusion-transmitted virus, is a single-stranded circular DNA virus that is being suspected to be pathogenetically associated to a few diseases such as hepatitis, idiopathic pulmonary fibrosis, idiopathic inflammatory myopathy, some cancers, and lupus erythematosus [9, 11,12,13]. However, very little is known about this virus, except that the prevalence in the serum of normal blood donors is considerably higher than would be expected, suggesting the possibility of persistent infection or coinfection with other microorganisms [9, 12]. There have been a number of studies conducted into the possible pathogenicity of TTV/TTMV in human diseases but more evidence for confirmation is still needed [9, 12, 13].
With this consequential reasoning, we performed quantitative polymerase chain reaction (qPCR) for TTV/TTMV in a 26-year-old woman with pathologically confirmed KFD using the formalin-fixed, paraffin-embedded tissue of the patient’s cervical lymph node. Surprisingly, there was PCR amplification in the sample and the subsequent DNA sequencing matched to the virus (under publication). Thus, we designed this study to investigate the TTV positivity in the lymph node samples of KFD patients, compare the rate with the matched normal controls, and discuss a possible relationship between TTV/TTMV and KFD.
Materials and methods
Samples
This study design was reviewed and approved by the Institutional Review Board of The Catholic University of Korea College of Medicine (SC14TISI0016). The formalin-fixed paraffin-embedded tissues of cervical lymph nodes of pathologically confirmed KFD patients, sequentially selected from the archive of Yeouido St. Mary’s Hospital from January 2005 to February 2013, were analyzed for TTV/TTMV qPCR. The 50 matched control samples of normal cervical lymph nodes were analyzed with the same methods to compare the amplification. Only cervical lymph nodes that were excised and confirmed as KFD were included to exclude the possibility of other kinds of viral or bacterial lymphadenitis. Needle biopsy or aspiration biopsy samples were excluded for the possibility of low DNA and poor amplification. Only the cases with negative results on the tuberculosis PCR or special staining for acid-fast bacilli were included to exclude the possibility of mycobacterial infection that is endemic in Korea. In all the cases, the possibility of fungal infection was excluded during the diagnosis process using periodic acid-Schiff (PAS) stain and methenamine silver stains if needed. Likewise, Warthin-Starry stain was used to exclude the possibility of Bartonella henselae infection, cat-scratch disease. Tissue Gram stain was used to exclude the possibility of bacterial infection; in situ hybridization for the EBV was used to exclude EBV infection if needed. For control samples, only excised cervical lymph nodes from the age-matched normal hosts without significant issues on the general health status, such as cancers, autoimmune diseases, infectious diseases, or other diseases that can affect general body system, were selected. The tissues were smaller than 0.3 cm or with extensive necrosis that can interfere with proper DNA extraction and subsequent qPCR were excluded. If there were several paraffin blocks in each case, all blocks were used for the DNA extraction.
Quantitative polymerase chain reaction and sequencing
For DNA extraction, at least three 10-μm-thick sections were cut from the formalin-fixed, paraffin-embedded tissue blocks and collected in a 1.5-mL microcentrifuge tube. DNA was extracted using Gentra® Puregene® Tissue kit (Qiagen, CA, USA) according to the manufacturer’s instructions. After deparaffinization with xylene, the tissues were homogenized using a pestle and incubated with proteinase K at 55 °C overnight. The extracted DNA sample was purified using MinElute® purification kit (Qiagen, CA, USA) according to the manufacturer’s instructions. The purified DNA was quantified using Nanodrop® 1000 spectrophotometer (Thermo Fisher Scientific, USA). The DNA was diluted to 50 ng/μL.
Two-step qPCR amplification was performed using TaKaRa SYBR® Premix EX Taq kit (cat. no. RR420A, TaKaRa Co., Japan) with Thermal Cycler Dice® Real-Time System TP800 (TaKaRa, Japan) according to the manufacturer’s instructions. The primers specific for the conserved region of TTV/TTMV used for qPCR amplification are shown in Table 1 [14].
qPCR conditions are shown in Table 2.
The PCR amplification was confirmed using gel electrophoresis with size standards.
Subsequent DNA sequencing with forward and reverse primer was done for TTV and TTMV using Genetic Analyzer 3130xl (Applied Biosystems, USA). The obtained sequence was searched in the BLAST databases (https://blast.ncbi.nlm.nih.gov/Blast.cgi) for matching sequence.
Statistics
All analysis included were performed using R (version 3.2.3 via http://web-r.org/). Performed statistical analyses include the Mann-Whitney test for continuous variables and Fisher’s exact test or chi-square tests for categorical variables.
Results
Patients and sample characteristics
The characteristics of the KFD patients and the normal hosts included in this study are summarized in Table 3. The male and female KFD patients were 29 and 71, respectively, and showed a ratio of 1 to 1.4. Included normal hosts were 19 males and 31 females with a ratio of 1 to 1.6. The mean age of the KFD patients was 23.5 years (range 3 to 61), while the mean age of normal hosts was 42.4 years (range 1 to 85). The pathologic subtypes of KFD were 54 lymphohistiocytic, 21 phagocytic, 19 necrotic, 4 foamy histiocytic types, and 2 types with extensive old hemorrhage. Histologically, the lymph nodes of normal hosts were all reactive lymphoid hyperplasia.
qPCR and DNA sequencing results
The qPCR results are summarized in Table 4.
The average paraffin blocks used for analysis were 1.4 ± 1.0 for KFD and 1.0 ± 0 for normal hosts. The extracted DNA quantities are 164.1 ng/μL ± 181.1 for KFD samples and 210.0 ng/μL ± 284.4 for normal host samples. PCR band were observed in 85 out of 100 cases (85%) in KFD samples and 9 out of 50 cases (18%) in normal controls for TTV, and 91 out of 100 cases (91%) in KFD samples and 12 out of 50 cases (24%) in normal controls for TTMV, which is significantly higher in KFD samples than normal controls. Average Ct value were 36.5 ± 1.7 in KFD samples and 38.2 ± 1.2 in normal controls for TTV, and 31.0 ± 0.8 in KFD samples and 33.1 ± 3.6 in normal controls for TTMV. Consequential sequencing was successful in 72 out of 85 cases of KFD samples (85%) and 8 out of 9 cases of normal controls (89%) for TTV, and 54 out of 91 cases of KFD samples (59%) and 10 out of 12 of normal controls (77%) for TTMV. The sequence was matched in 7 out of 72 cases of KFD samples (9.7%) and 5 out of 8 cases of normal controls (63%) for TTV, and 51 out of 54 cases of KFD samples (94%) and 3 out of 10 cases of normal controls (30%) for TTMV, which is significantly different between KFD samples and normal controls. Overall, in TTV, 7 out of 100 KFD cases (7%) and 5 out of 50 normal controls (10%) showed a matched sequence, which is similar between the two groups. In TTMV, however, 51 out of 100 cases of KFD samples (51%) showed matched sequence, while only 3 out of 50 cases of normal controls (6%) showed matched sequence, which is significantly different between the groups. There was no specific association between other variables including age, sex, and pathologic subtypes and TTV or TTMV amplification.
Discussion
In this study, we first found the increased positivity of TTMV in the cervical lymph nodes of KFD patients than the normal controls (94% vs. 30%/51% vs. 6%, p < 0.0000) by qPCR. The findings of this study are meaningful for two reasons. First, the findings of this study implicate a possible pathogenic role of TTV/TTMV in KFD. Second, it calls attention to the requirement for further exploration into the potential pathogenicity of TTV/TTMV in various human diseases.
The results of this study imply a potential role of TTV/TTMV in the pathogenesis of KFD. Despite the relatively well-established clinicopathologic features of KFD, the etiology of this disease has remained unknown nearly for 50 years since its first recognition [1]. Because of the benign nature and the limited presentation in Asian young adults of KFD, it has not been drawing the researchers’ attention enough so far. Unlike the previous fact that it is a rare disease of young Asian population limited in Japan, Korea, and Taiwan, an increasing number of studies have been reported outside Asia recently including Europe, Middle Asia, North and South America, and Africa [15,16,17,18,19,20].
The clinical symptoms such as self-limiting fever, upper respiratory prodrome, atypical lymphocytosis, and elevated erythrocyte sedimentation rate strongly suggest the possibility of infectious cause especially viral. In addition, no response to antibiotic therapy, rare recurrence, the proliferation of immunoblasts, predominance of CD8+ T cells, and presence of necrotic foci localized to T cell areas are another evidence favoring infectious etiology. However, most human pathogens have been found not to be associated with KFD. In our previous meta-analysis covering over 2491 studies analyzing the association of KFD to infectious pathogens, none of the most common human pathogens, including all types of HHV, HPV, parvovirus B19, HBV, and HTLV-1, are found to be associated to KFD with a relevant statistical significance [6]. The most suspected pathogen, EBV, was confirmed not to be associated with KFD than controls. Although HHV8 was found to be associated with KFD than controls with an odds ratio of 8.24, overall positivity of HHV8 in KFD was only 4.8%, which is insufficient to explain the main role of HHV8 in the pathogenesis of KFD, especially considering the fact that the number of studies used for meta-analysis on HHV8 was limited (only 4 studies). Although the relationship of HHV6, 7, and parvovirus B19 and KFD was not completely excluded by the meta-analysis due to the limited number of included studies, the level of association seems to be all negative and the level of the evidence of the included studies was low because of limited number of samples, poor study design, and case and matched control selection.
This study is meaningful because we first conducted a meta-analysis before this case-control study to exclude any kinds of possible bias from the study design. We chose the putative pathogen, TTV/TTMV, because of the histologic similarity of necrotizing lymphadenitis in pigs caused by circovirus and KFD in human potentially by TTV/TTMV based on the extensive literature review; TTV/TTMV and circovirus also shares a lot in common that TTV/TTMV was initially classified as a member of the Circoviridae family [21]; both viruses are structurally similar, a single-stranded circular DNA virus with no envelope that mainly infect mammals, including pigs and dogs, and can cause fever, neutropenia, weight loss, and hemorrhagic diarrhea, and show necrotizing vasculitis and granulomatous inflammation; necrotizing lymphadenitis with brisk apoptotic bodies, characteristic for KFD in humans, has also been described in pigs with PMWS [7]. We carefully selected pathologically confirmed KFD cases after exclusion of other possible lymphadenitis caused by tuberculosis, cat-scratch disease, EBV infection, systemic lupus erythematosus, histoplasmosis, leprosy, and syphilis. For the accurate molecular tests, we chose the cases with sufficient amount of paraffin tissue (only excised samples). We carefully chose the matched normal controls enough to show the proper answer that has statistical power. Finally, we chose to use the paraffin blocks instead of blood samples to know the TTV/TTMV status in the lesion where the pathologic process is being held not in the blood of the normal population that might reflect asymptomatic infection. As a result, TTMV positivity was found significantly higher in KFD than normal controls (51% vs. 6%, p < 0.0000). Although the presence of the higher viral load in the analyzed samples of KFD cannot explain everything about the pathogenetic role of TTV/TTMV in KFD while the pathogenicity of TTV/TTMMV in human disease is not fully elucidated, this finding might be considered as a prerequisite or precursory finding that is significantly associated to the pathogenesis of KFD.
Besides the virologic and pathologic similarity of TTV/TTMV to circovirus, there are a lot more things that cannot be neglected regarding the epidemiologic feature of TTV and KFDs. The TTV occurrence was reported to be the highest in the normal population of Japan as 92.0%, whereas it varies but quite low from 2.6 to 54.0% in other regions of the world as the KFD is most prevalent in East Asian countries such as Japan and Korea [22]. Although the occurrence rate of overall TTV was reported to increase with age, a certain type (genogroup 2) of TTV was the highest in the youngest age group as 80%, followed by subadult group as 60.3%, and the lowest in adults as 58.3% that can be a reasonable explanation about the highest prevalence of KFD in young adults [22]. Likewise, genogroup 2 TTV was found higher in females as 74.2% than in males as 57.0% as KFD is more prevalent in female than male hosts [22]. It can be dangerous to jump to the conclusion with only these facts that TTMV is the cause of KFD, but it probably should not be neglected understanding that TTMV and TTV share a lot of similarity about viral structure and epidemiology. One more thing, we still do not know whether TTV/TTMV infection alone can be a major player in KFD pathogenesis yet but there must be a chance that it can be a part of co-infection as it is in the relationship between human immunodeficiency virus (HIV) and HHV8 in many of human diseases. Interestingly, higher TTV/TTMV infections were reported in the patients with HIV and hepatitis C virus co-infection, raising this suspicion [23]. In our previous meta-analysis, HHV8 was statistically associated with KFD although the overall positivity was quite low [6]. Considering the fact that HHV8 is closely related to HIV and so does TTV as TTV titer also increases as the HIV infection progresses, there might be a hidden relationship between TTV and other viruses such as HHV8 in the pathogenesis of KFD.
Therefore, the results of this study also demand more attention to TTV/TTMV in terms of the pathogenic role in human diseases. After its first discovery by Mayumi et al. (1997) in a Japanese patient with non-A to G post-transfusion hepatitis, the pathogenicity of TTV/TTMV in human diseases, such as a dozen of hepatic, pulmonary diseases, hematologic disorders, autoimmune disorders, and even cancers, has been anecdotally raised [9, 11,12,13, 24]. Remarkably, Tokita et al. suggested that TTV infection might cause more hepatic cellular carcinoma in hepatitis C virus patients in 2002 [25]. More recently, Bando et al. claimed that TTV/TTMV infection in idiopathic pulmonary fibrosis (IPF) can cause lung cancer more than control as a complication by presenting the results that TTV/TTMV DNA titer was significantly higher in the lung cancer patients with prior IPF than the patients either with only lung cancers or IPF [13]. In the study that first identified TTMV in the brain tissue with metastatic melanoma of a 57-year-old male patient using viral metagenomics, Ng et al. indicated the potential implication of the indirect carcinogenic effects of TTMV by modulating T cell immune responses. They suggested that TTMV might play a role in the carcinogenesis of some cancers by expressing specific miRNAs that inhibit the interferon signaling [26].
In 2008, Maggi et al. reported that higher serum TTV viral loads correlate with lower circulating CD4+ helper T cells and higher circulating CD8+ T cells and CD19+ B cells. They found higher TTV viral loads in the children with bronchopneumonia than in the children with milder form of acute respiratory diseases, and they suggested that florid TTV replication might contribute to lymphocyte imbalance (high CD8+ and low CD4+ T cells) and possibly temporal immunosuppressive effects as animal circoviruses are markedly immunosuppressive in their respective animal host species [27, 28]. It is very interesting to be considered as just a coincidence that KFD also shows predominance of CD8+ T cells, proliferation of CD19+ immunoblasts, and upper respiratory prodrome in young patients.
In summary, KFD or histiocytic necrotizing lymphadenitis is a rare, benign, self-limiting disorder with clinicopathological features of viral infection. This is the first clinical study to demonstrate the statistically higher TTV viral loads in KFD than normal controls, which implies a potential pathogenic role of TTMV in KFD. Further investigation with molecular techniques based and animal experimental study should be followed in the future.
References
Bosch X, Guilabert A, Miquel R, Campo E (2004) Enigmatic Kikuchi-Fujimoto disease: a comprehensive review. Am J Clin Pathol 122:141–152. https://doi.org/10.1309/yf08-1l4t-kywv-yvpq
Ioachim HL, Medeiros LJ (2009) Ioachim’s lymph node pathology, 4th edn. Wolters Kluwer/Lippincott Williams & Wilkins, Philadelphia
Kikuchi M (1972) Lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytes: a clinicopathological study. Nihon Ketsueki Gakkai Zasshi 35:379–380
Fujimoto Y, Kozima Y, Yamaguchi K (1972) Cervical subacute necrotizing lymphadenitis: a new clinicopathologic entity. Naika 20:920–927
Hudnall SD (2000) Kikuchi-Fujimoto disease. Is Epstein-Barr virus the culprit? Am J Clin Pathol 113:761–764. https://doi.org/10.1309/n4e2-78v9-qtfh-x4ff
Chong Y, Kang CS (2014) Causative agents of Kikuchi-Fujimoto disease (histiocytic necrotizing lymphadenitis): a meta-analysis. Int J Pediatr Otorhinolaryngol 78:1890–1897. https://doi.org/10.1016/j.ijporl.2014.08.019
Galindo-Cardiel I, Grau-Roma L, Pérez-Maillo M, Segalés J (2011) Characterization of necrotizing lymphadenitis associated with porcine circovirus type 2 infection. J Comp Pathol 144:63–69. https://doi.org/10.1016/j.jcpa.2010.06.003
Segalés J, Allan GM, Domingo M (2007) Porcine circovirus diseases. Anim Health Res Rev 6:119–142. https://doi.org/10.1079/ahr2005106
Hino S, Miyata H (2007) Torque teno virus (TTV): current status. Rev Med Virol 17:45–57. https://doi.org/10.1002/rmv.524
Thom K, Morrison C, Lewis JC, Simmonds P (2003) Distribution of TT virus (TTV), TTV-like minivirus, and related viruses in humans and nonhuman primates. Virology 306:324–333. https://doi.org/10.1016/s0042-6822(02)00049-1
Nishizawa T, Okamoto H, Konishi K, Yoshizawa H, Miyakawa Y, Mayumi M (1997) A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochem Biophys Res Commun 241:92–97. https://doi.org/10.1006/bbrc.1997.7765
Cossart Y (2000) TTV-a virus searching for a disease. J Clin Virol 17:1–3
Bando M, Takahashi M, Ohno S, Hosono T, Hironaka M, Okamoto H, Sugiyama Y (2008) Torque teno virus DNA titre elevated in idiopathic pulmonary fibrosis with primary lung cancer. Respirology 13:263–269. https://doi.org/10.1111/j.1440-1843.2007.01217.x
Moen EM, Sleboda J, Grinde B (2002) Real-time PCR methods for independent quantitation of TTV and TLMV. J Virol Methods 104:59–67
Ifeacho S, Aung T, Akinsola M (2008) Kikuchi-Fujimoto disease: a case report and review of the literature. Cases J 1:187. https://doi.org/10.1186/1757-1626-1-187
Deaver D, Naghashpour M, Sokol L (2014) Kikuchi-fujimoto disease in the United States: three case reports and review of the literature [corrected]. Mediterr J Hematol Infect Dis 6:e2014001. https://doi.org/10.4084/MJHID.2014.001
D’Introno A, Perrone A, Schilardi A, Gentile A, Sabba C, Napoli N (2017) Kikuchi-Fujimoto disease in an old Italian woman: case report and review of the literature. Case Rep Med 2017:7257902. https://doi.org/10.1155/2017/7257902
Lame CA, Loum B, Fall AK, Cucherousset J, Ndiaye AR (2017) Kikuchi-Fujimoto disease, a rare cause of lymphadenopathy in Africa. Description of the first case in Senegal and review of the literature. Eur Ann Otorhinolaryngol Head Neck Dis 134:347–349. https://doi.org/10.1016/j.anorl.2017.02.007
Youssef A, Ali R, Ali K, AlShehabi Z (2017, 2017) Kikuchi-Fujimoto disease: a case report of a multi-drug resistant, grueling disease. Oxf Med Case Rep:omx024. https://doi.org/10.1093/omcr/omx024
Sousa Ade A, Soares JM, Sa Santos MH, Martins MP, Salles JM (2010) Kikuchi-Fujimoto disease: three case reports. Sao Paulo Med J 128:232–235
Chae C (2005) A review of porcine circovirus 2-associated syndromes and diseases. Vet J 169:326–336. https://doi.org/10.1016/j.tvjl.2004.01.012
Bostan N, Amen NE, Bokhari H (2013) Current and future prospects of torque teno virus. J Vaccines Vaccin S1:004. https://doi.org/10.4172/2157-7560.s1-004
Garcia-Alvarez M, Berenguer J, Alvarez E, Guzman-Fulgencio M, Cosin J, Miralles P, Catalan P, Lopez JC, Rodriguez JM, Micheloud D, Munoz-Fernandez MA, Resino S (2013) Association of torque teno virus (TTV) and torque teno mini virus (TTMV) with liver disease among patients coinfected with human immunodeficiency virus and hepatitis C virus. Eur J Clin Microbiol Infect Dis 32:289–297. https://doi.org/10.1007/s10096-012-1744-1
Ruaro B, Sulli A, Alessandri E, Fraternali-Orcioni G, Cutolo M (2014) Kikuchi-Fujimoto’s disease associated with systemic lupus erythematous: difficult case report and literature review. Lupus 23:939–944. https://doi.org/10.1177/0961203314530794
Tokita H, Murai S, Kamitsukasa H, Yagura M, Harada H, Takahashi M, Okamoto H (2002) High TT virus load as an independent factor associated with the occurrence of hepatocellular carcinoma among patients with hepatitis C virus-related chronic liver disease. J Med Virol 67:501–509. https://doi.org/10.1002/jmv.10129
Ng TFF, Dill JA, Camus AC, Delwart E, Van Meir EG (2017) Two new species of betatorqueviruses identified in a human melanoma that metastasized to the brain. Oncotarget 8:105800–105808. https://doi.org/10.18632/oncotarget.22400
Maggi F, Pifferi M, Tempestini E, Fornai C, Lanini L, Andreoli E, Vatteroni M, Presciuttini S, Pietrobelli A, Boner A, Pistello M, Bendinelli M (2003) TT virus loads and lymphocyte subpopulations in children with acute respiratory diseases. J Virol 77:9081–9083. https://doi.org/10.1128/jvi.77.16.9081-9083.2003
Maggi F, Ricci V, Bendinelli M, Nelli LC, Focosi D, Papineschi F, Petrini M, Paumgardhen E, Ghimenti M (2008) Changes In CD8+ 57+ T lymphocyte expansions after autologous hematopoietic stem cell transplantation correlate with changes in torquetenovirus viremia. Transplantation 85:1867–1868. https://doi.org/10.1097/TP.0b013e31817615e6
Acknowledgments
I appreciate Seung Bum Hong, M.S., at the Division of DNA Analysis, Department of Forensic Medicine, Scientific Investigation Laboratory, Criminal Investigation Command, Ministry of National Defense, Seoul, Republic of Korea for analyzing and reviewing DNA sequencing. I appreciate Mr. Young Dong Seo for reviewing the manuscript style.
Funding
This study was partly funded by a research grant from the Institute of Clinical Medicine Research, Catholic University of Korea, Yeouido St. Mary’s Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chong, Y., Lee, J.Y., Thakur, N. et al. Strong association of Torque teno virus/Torque teno-like minivirus to Kikuchi-Fujimoto lymphadenitis (histiocytic necrotizing lymphadenitis) on quantitative analysis. Clin Rheumatol 39, 925–931 (2020). https://doi.org/10.1007/s10067-019-04851-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-019-04851-4