
Abstract
Giant cell arteritis (GCA) is the most common vasculitis in adults aged ≥ 50 years in Europe. Recently, colour Doppler ultrasonography (CDS) and positron emission tomography-computed tomography (PET/CT) have improved the diagnostic sensitivity. The aim of our study was to determine the incidence of GCA in a well-defined Slovenian region, supported by the temporal artery (TA) biopsy (TAB) or CDS or PET/CT. This prospective study was conducted at the University Medical Centre Ljubljana, the only secondary/tertiary centre in the region, serving a population of 323,297 residents aged ≥ 50 years. Patients with suspected GCA are referred either to the Department of Rheumatology, or in case of severe visual disturbances, to the Department of Ophthalmology. We included all GCA cases diagnosed between 1 January 2012 and 31 December 2017. We diagnosed cranial GCA (c-GCA) using the American College of Rheumatology (ACR) 1990 classification criteria and a positive TAB or TA-CDS. Large vessel GCA (lv-GCA) was diagnosed using CDS or PET/CT. During the 6-year observation, we identified 169 incipient GCA cases (66.3% female, median (IQR) age of 75.1 (68.6–80.0) years). Forty-two (24.8%) patients had lv-GCA, and the others had c-GCA. The estimated annual incidence rates of GCA were overall 8.7 (95% CI 7.5–10.1), c-GCA 6.5 (95% CI 5.5–7.8) and lv-GCA 2.2 (95%CI 1.6–2.9) per 100,000 aged ≥ 50 years. GCA is the most common vasculitis in adults aged ≥ 50 years, with an annual incidence rate of 8.7 per 100,000.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Giant cell arteritis (GCA) is a vasculitis of the large and medium sized arteries, affecting the adult population over the age of 50 years [1]. It is the most common systemic vasculitis in Western Europe and North America, with the reported incidence rates between 1.0 and 76.6 per 100,000 adults aged ≥ 50 years (Table 1) [2,3,4,5,6,7,8,9,10,11,12,13]. The involvement of the cranial arteries (c-GCA), with the potential severe complications, such as permanent visual loss and ischemic stroke, is well known. The modern imaging modalities, e.g. colour Doppler ultrasonography (CDS), magnetic resonance angiography, computer tomographic angiography, and fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT), have enabled us to study the involvement of other vascular territories, especially the arteries stemming from the aortic arch and identifying the so called large vessel GCA (lv-GCA). The frequency of lv-GCA depends on the imaging modality used, varying between 18 and 83% [14, 15]. The incidence of lv-GCA has thus far not yet been systematically studied. The aim of our prospective study was to determine the incidence of GCA in a well-defined country region, using not only ACR classification criteria with a positive temporal artery biopsy (TAB) result as the gold standard but also the results of CDS and/or PET-CT.
Methods
Setting
This prospective study was performed at the University Medical Centre (UMC) Ljubljana, in collaboration with the Institute of Pathology, the Medical Faculty, University of Ljubljana. The UMC Ljubljana is the only centre providing a rheumatological service for the adult population of both the Ljubljana and Gorenjska regions. The patients with suspected GCA from these two regions are referred by their family doctor or local/private practice ophthalmologists to the Department of Rheumatology, UMC Ljubljana, or in case of severe visual disturbances, to the Department of Ophthalmology, UMC Ljubljana. When suspected cases are first observed by another subspecialist (e.g. neurologist, specialist of infectious diseases, angiologist, ear, nose and throat specialist, etc.), a rheumatologist is regularly consulted. The Institute of Pathology, the Medical Faculty, University of Ljubljana processes and analyses all the TAB samples performed in the Ljubljana and Gorenjska regions.
Patients
We included incipient GCA cases diagnosed between 1 January 2012 and 31 December 2017, who then were residents of the Ljubljana region or the Gorenjska region.
The Ljubljana region and the Gorenjska region combined had an average adult population of 704,342; 323,297 of these were aged ≥ 50 years (176,104 females, and 147,193 males) according to the data obtained from the Department of Demographic and Social Statistics at the Statistical Office of the Republic of Slovenia. More than 95% of residents were Caucasians.
Giant cell arteritis diagnosis
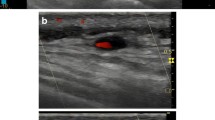
Patients with symptoms compatible with c-GCA needed to fulfil the American Colleague of Rheumatology, 1990 (ACR) classification criteria, and also have a positive TAB or the halo sign on TA-CDS. In the event of signs and symptoms of extracranial large artery involvement and negative TAB or TA CDS; GCA was diagnosed when the findings of CDS of the large arteries or PET/CT were consistent with vasculitis. We routinely examined the large supra-aortic arteries: carotid, vertebral, subclavian, axillary and brachial arteries by CDS. Lower limb arteries (the external iliac artery, femoral artery, popliteal artery, posterior tibial artery and the dorsal artery of the foot) were examined only in those patients that presented with symptoms consistent with vasculitic involvement of the lower limb arteries.
In patients who were first referred to a rheumatologist, we performed CDS prior to the initiation of glucocorticoid treatment. In patients with severe visual manifestations, who were first referred to an ophthalmologist, we performed CDS after the initiation of glucocorticoids.
In order not to miss rare cases of GCA in the residents of the studied regions diagnosed and managed in hospitals in other Slovenian regions, a list of patients with TAB performed during the study time period was obtained from the Institute of Pathology.
Statistical analysis
The annual incidence rate of GCA was calculated using the average number of new GCA cases observed annually as the numerator, and the average adult population aged 50 years or more of the studied two regions as the denominator. The 95% confidence interval (CI) was calculated using the one-sample Poisson rate. Statistical analyses were done using the MiniTab v16, MiniTab Inc., USA.
Ethics committee approval
The study was approved by the National Medical Ethics Committee.
Results
During the 6-year observation period, we identified 169 incipient GCA cases (66.3% female, female to male ratio 2.0) in the Ljubljana and Gorenjska regions. One hundred and fifty-four (91.1%) cases were diagnosed at the Department of Rheumatology and 15 (8.9%) cases at the Department of Ophthalmology. No residents from the studied regions were diagnosed with GCA in other Slovenian hospitals. The median patient age (interquartile range (IQR)) was 75.1 (68.6–80.0, 54.6–97.5) years. The median (IQR) disease duration time was 30 (14–60) days.
The allocation of cases according to the way of diagnosing GCA is presented in Fig. 1. One-hundred-and-thirty-nine (82.2%) patients fulfilled the ACR classification criteria. A TAB was performed in 128 (75.7%) cases, and was consistent with GCA in 108 (84.4%) cases. The remaining patients who fulfilled ACR classification criteria had a positive TA-CDS. Thirty patients who did not fulfil the ACR classification criteria had either positive CDS of other arteries or PET/CT (18 cases had positive CDS, 3 cases positive PET/CT, and 9 cases positive both CDS and PET/CT). A TAB was performed in 9 of these 30 cases, and was positive in 3 of them. In total, we found extracranial large vessel involvement in 42 (24.8%) cases. The clinical characteristics of our GCA cohort are presented in Table 2. Patients with lv-GCA were significantly younger than those with c-GCA (p = 0.001), and numerically, but not significantly so, more often female (76.2% vs. 63.0%).

Chart flow of diagnosing GCA. TAB temporal artery biopsy; CDS colour Doppler ultrasonography; TA temporal artery, extracranial large arteries; PET/CT positron emission tomography–computed tomography
Based on the adult population of the pooled Ljubljana and Gorenjska regions, we determined the age adjusted annual incidence rate of GCA at 8.7 (95% CI 7.5–10.1) per 100,000 adults ≥ 50 years. The estimated incidence rate in females was 10.6 (95% CI 8.8–12.7) and in males 6.4 (95% CI 4.9–8.3) per 100,000 adults ≥ 50 years. The age adjusted incidence of c-GCA was 6.5 (95% CI 5.5–7.8) per 100,000 ≥ 50 years (females 7.6 (95% CI 6.0–9.4), males 5.3 (95% CI 3.9–7.0)), and the age adjusted incidence of lv-GCA 2.2 (95% CI 1.6–2.9) per 100,000 ≥ 50 years (females 3.0 (95% CI 2.1–4.2), males 1.1 (95% CI 0.6–2.0)).
The estimated incidence rate increased with patient age, and was the highest in the age group between 70 and 79 years (20.0 (95% CI 15.9–24.8) cases per 100,000). Age and gender specific incidence rates are presented in Fig. 2. We found no significant seasonal variations of GCA. There were 40 (23.7%), 41 (24.3%), 42 (24.8%), and 46 (27.2%) cases in spring, summer, autumn, and winter, respectively. Nevertheless, an annual fluctuation of new GCA cases was noted (the lowest number of new GCA cases in year 2013 (20 new cases (11.8%) and the highest number in year 2016 (37 new cases (21.9%)); this difference was statistically significant (p = 0.024) (Fig. 3).

Age- and gender-specific incidence rates of GCA

Annual variation of GCA cases
Discussion
The epidemiology of GCA has been extensively investigated in the past. Most studies were retrospective, relied on the ACR 1990 classification criteria, accepting the TAB as the diagnostic gold standard, and thus focused on c-GCA and missed lv-GCA cases [2,3,4,5,6, 9,10,11,12,13].
The present study is a prospectively designed epidemiological study in which we, in addition to the ACR classification criteria and a TAB, implemented CDS and PET/CT to encompass the entire spectrum of the disease. This is the first study ever to evaluate the incidence of extracranial large vessel-GCA (i.e. lv-GCA).
The estimated overall incidence rate of GCA in a well-defined region of Slovenia was 8.7 (95% CI 7.5–10.1) cases per 100,000 adults aged ≥ 50 years. The incidence rate was two to three times lower than in the Scandinavian countries, comparable to those from Spain, Canada, and Jerusalem, and even slightly higher than in Italy [1, 3,4,5, 7, 12, 16]. The incidence rate of c-GCA was nearly three times higher than that of lv-GCA (6.5 (95% CI 5.5–7.8) vs. 2.2 (95%CI 1.6–2.9) per 100,000 adults over the age of 50 years). The Slovenian population of two million is demographically homogenous, thus we assume the incidence figures are representative of the entire country.
GCA typically manifests in adults over the age of 50 years. The incidence rate increases with the patient age and was the highest in patients aged ≥ 80 years based on the studies from Minnesota, South Australia, and Italy [6, 7, 9]. In our cohort, the incidence rate peaked at 20.0 per 100,000 adults of 70–79 years of age, who represented 46.7% of all cases.
As previously reported, we found that GCA was more prevalent in women than in men (female to male ratio of 2.0) [3, 7, 10, 13, 17]. In contrast to the reported even higher (4–5-times) female preponderance in lv-GCA compared to c-GCA, we found no significant difference in gender between c-GCA and lv-GCA (female to male ratio of 2.7 and 1.4 in lv-GCA and c-GCA, respectively) [18, 19].
In the long-term, studies of the annual fluctuations of incidence rates that could point to potential environmental, e.g. infectious, triggers of GCA with a cyclic pattern were observed [4, 7]. In Olmsted county, Minnesota, there were six peaks approximately 7 years apart during the 50 years of observation [6]. Similar cyclic patterns, albeit of a different interval, were also reported from Sweden and Jerusalem but not from Spain [3,4,5]. We also observed annual fluctuations in the incidence rates although the short 6-year observation period precluded us from observing any potential cyclic patterns.
About a quarter of our cohort had lv-GCA. Among the 42 lv-GCA patients, 24 (57.1%) fulfilled the ACR classification criteria, and 19 out of 24 patients (79.2%) had a positive TAB. In a previous study of lv-GCA, about 40% fulfilled the ACR classification criteria, and fewer than 45% of patients had a positive TAB. [19] The reason for the high rate of TAB positivity in our cohort is that we only performed the TAB in patients with a halo sign on TA CDS.
The strengths of our study were the prospective unselected inclusion of subjects with both c-GCA and lv-GCA by employing a systematic fast-track work-up that included a TAB, as well as CDS, and when deemed necessary PET/CT for the first time in a GCA incidence study. Additionally, the study covered two well-defined regions that represented about a third of the entire Slovenian population, enabling us to extrapolate the results to the entire country.
There were several reasons to include imaging studies in addition to the ACR classification criteria and a TAB in the diagnostic work-up of GCA. A TAB is a reasonably safe and uncomplicated outpatient procedure, with two major drawbacks. Firstly, it can be false negative, and secondly, it is not readily available in some centres. In our c-GCA subgroup, 14.4% of cases had a negative TAB, while it is usually available within 24 h after presentation in our centre. By systematically employing the CDS-TA in addition to a TAB, we improved the diagnostic sensitivity of the GCA as shown by the TABUL study [20]. Additionally, the present study is the first one to evaluate the incidence of lv-GCA. Based on the observations of Diamantopoulos et al., who found that CDS of a common carotid, axillary, and temporal arteries yielded a 100% sensitivity for GCA diagnosis, we mostly employed CDS of the supraaortic arteries and lower limb arteries when the patient’s symptoms pointed to their involvement [21].
The drawbacks of our study were its relatively short duration, and the failure to perform all the imaging studies in every patient. We performed CDS-TA in 94.1% and CDS of the large extracranial arteries in 89.3% of patients. The imaging studies were not performed in patients with severe vision disturbances, e.g. vision loss, that were treated with glucocorticoids prior to referral to the Department of Rheumatology, since 2 to 4 days of glucocorticoids have been shown to significantly influence the findings on CDS [22].
In conclusion, the estimated overall incidence rate of both c-GCA and lv-GCA in Slovenia of 8.7 (95% CI 7.5–10.1) cases per 100,000 adults aged ≥50 years was comparable with studies from southern Europe, with the incidence rate of c-GCA being nearly 3 times higher than that of lv-GCA, when CDS was the predominantly used imaging modality.
Funding statement
The authors would like to acknowledge funding from the Slovenian Research Agency (ARRS) for the National Research Programme P3-0314.
References
Gonzalez-Gay MA, Vazquez-Rodriguez TR, Lopez-Diaz MJ, Miranda-Filloy JA, Gonzalez-Juanatey C, Martin J, Llorca J (2009) Epidemiology of giant cell arteritis and polymyalgia rheumatica. Arthritis Rheum 61(10):1454–1461. https://doi.org/10.1002/art.24459
Pamuk ON, Donmez S, Karahan B, Pamuk GE, Cakir N (2009) Giant cell arteritis and polymyalgia rheumatica in northwestern Turkey: clinical features and epidemiological data. Clin Exp Rheumatol 27(5):830–833
Bas-Lando M, Breuer GS, Berkun Y, Mates M, Sonnenblick M, Nesher G (2007) The incidence of giant cell arteritis in Jerusalem over a 25-year period: annual and seasonal fluctuations. Clin Exp Rheumatol 25(1 Suppl 44):S15–S17
Gonzalez-Gay MA, Miranda-Filloy JA, Lopez-Diaz MJ, Perez-Alvarez R, Gonzalez-Juanatey C, Sanchez-Andrade A, Martin J, Llorca J (2007) Giant cell arteritis in northwestern Spain: a 25-year epidemiologic study. Medicine 86(2):61–68. https://doi.org/10.1097/md.0b013e31803d1764
Petursdottir V, Johansson H, Nordborg E, Nordborg C (1999) The epidemiology of biopsy-positive giant cell arteritis: special reference to cyclic fluctuations. Rheumatology 38(12):1208–1212
Salvarani C, Crowson CS, O'Fallon WM, Hunder GG, Gabriel SE (2004) Reappraisal of the epidemiology of giant cell arteritis in Olmsted County, Minnesota, over a fifty-year period. Arthritis Rheum 51(2):264–268. https://doi.org/10.1002/art.20227
Catanoso M, Macchioni P, Boiardi L, Muratore F, Restuccia G, Cavazza A, Pipitone N, Mancuso P, Luberto F, Salvarani C (2017) Incidence, prevalence, and survival of biopsy-proven giant cell arteritis in northern Italy during a 26-year period. Arthritis care & research 69(3):430–438. https://doi.org/10.1002/acr.22942
Boesen P, Sorensen SF (1987) Giant cell arteritis, temporal arteritis, and polymyalgia rheumatica in a Danish county. a prospective investigation, 1982-1985. Arthritis Rheum 30(3):294–299
Dunstan E, Lester SL, Rischmueller M, Dodd T, Black R, Ahern M, Cleland LG, Roberts-Thomson P, Hill CL (2014) Epidemiology of biopsy-proven giant cell arteritis in South Australia. Intern Med J 44(1):32–39. https://doi.org/10.1111/imj.12293
Mohammad AJ, Nilsson JA, Jacobsson LT, Merkel PA, Turesson C (2015) Incidence and mortality rates of biopsy-proven giant cell arteritis in southern Sweden. Ann Rheum Dis 74(6):993–997. https://doi.org/10.1136/annrheumdis-2013-204652
Mader TH, Werner RP, Chamberlain DG, Doornbos D (2009) Giant cell arteritis in Alaska natives. Can J Ophthalmol 44(1):53–56. https://doi.org/10.3129/i08-164
Ramstead CL, Patel AD (2007) Giant cell arteritis in a neuro-ophthalmology clinic in Saskatoon, 1998-2003. Can J Ophthalmol 42(2):295–298. https://doi.org/10.3129/canjophthalmol.i07-005
Baldursson O, Steinsson K, Bjornsson J, Lie JT (1994) Giant cell arteritis in Iceland. an epidemiologic and histopathologic analysis. Arthritis Rheum 37(7):1007–1012
de Boysson H, Aide N, Liozon E, Lambert M, Parienti JJ, Monteil J, Huglo D, Bienvenu B, Manrique A, Aouba A (2017) Repetitive (18)F-FDG-PET/CT in patients with large-vessel giant-cell arteritis and controlled disease. Eur J Intern Med 46:66–70. https://doi.org/10.1016/j.ejim.2017.08.013
Ness T, Bley TA, Schmidt WA, Lamprecht P (2013) The diagnosis and treatment of giant cell arteritis. Dtsch Arztebl Int 110(21):376–385; quiz 386. https://doi.org/10.3238/arztebl.2013.0376
Gonzalez-Gay MA, Garcia-Porrua C, Rivas MJ, Rodriguez-Ledo P, Llorca J (2001) Epidemiology of biopsy proven giant cell arteritis in northwestern Spain: trend over an 18 year period. Ann Rheum Dis 60(4):367–371
Kobayashi S, Yano T, Matsumoto Y, Numano F, Nakajima N, Yasuda K, Yutani C, Nakayama T, Tamakoshi A, Kawamura T, Ohno Y, Inaba Y, Hashimoto H (2003) Clinical and epidemiologic analysis of giant cell (temporal) arteritis from a nationwide survey in 1998 in Japan: the first government-supported nationwide survey. Arthritis Rheum 49(4):594–598. https://doi.org/10.1002/art.11195
Schmidt WA, Seifert A, Gromnica-Ihle E, Krause A, Natusch A (2008) Ultrasound of proximal upper extremity arteries to increase the diagnostic yield in large-vessel giant cell arteritis. Rheumatology 47(1):96–101. https://doi.org/10.1093/rheumatology/kem322
Muratore F, Kermani TA, Crowson CS, Green AB, Salvarani C, Matteson EL, Warrington KJ (2015) Large-vessel giant cell arteritis: a cohort study. Rheumatology 54(3):463–470. https://doi.org/10.1093/rheumatology/keu329
Luqmani R, Lee E, Singh S, Gillett M, Schmidt WA, Bradburn M, Dasgupta B, Diamantopoulos AP, Forrester-Barker W, Hamilton W, Masters S, McDonald B, McNally E, Pease C, Piper J, Salmon J, Wailoo A, Wolfe K, Hutchings A (2016) The role of ultrasound compared to biopsy of temporal arteries in the diagnosis and treatment of giant cell arteritis (TABUL): a diagnostic accuracy and cost-effectiveness study. Health Technol Assess 20(90):1–238. https://doi.org/10.3310/hta20900
Diamantopoulos AP, Haugeberg G, Hetland H, Soldal DM, Bie R, Myklebust G (2014) Diagnostic value of color Doppler ultrasonography of temporal arteries and large vessels in giant cell arteritis: a consecutive case series. Arthritis care & research 66(1):113–119. https://doi.org/10.1002/acr.22178
Hauenstein C, Reinhard M, Geiger J, Markl M, Hetzel A, Treszl A, Vaith P, Bley TA (2012) Effects of early corticosteroid treatment on magnetic resonance imaging and ultrasonography findings in giant cell arteritis. Rheumatology 51(11):1999–2003. https://doi.org/10.1093/rheumatology/kes153
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Rheumatology in Slovenia: Clinical practice and translational research
Rights and permissions
About this article

Cite this article
Pucelj, N.P., Hočevar, A., Ješe, R. et al. The incidence of giant cell arteritis in Slovenia. Clin Rheumatol 38, 285–290 (2019). https://doi.org/10.1007/s10067-018-4236-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-018-4236-6