
Abstract
The objective of this study was to systemically and comprehensively evaluate the associations between smoking and disease outcomes in patients with ankylosing spondylitis (AS). Information on smoking, clinical features, and sociodemographic characteristics was collected by a questionnaire administered directly to the patient. Group differences were analyzed by t test or chi-square test. Logistic regression analysis was conducted with the Bath AS Disease Activity Index (BASDAI), Bath AS Functional Index (BASFI), C-reactive protein, and erythrocyte sedimentation rate as the dependent variables and different stratification of smoking duration, smoking intensity, and cumulative smoking as independent variables. In order to compare our results with previous studies, meta-analysis was performed to calculate standardized mean difference (SMD) for relationship between outcomes and smoking status. A total of 1178 AS patients were analyzed. Compared with non-smokers, the risk of having active disease (BASDAI ≥ 4) was higher in patients who smoked at least 15 years, or 15 cigarettes per day, or 15 pack-years (OR = 1.70 [1.06, 2.73], 1.75 [1.08, 2.82], and 1.97 [1.06, 3.67], respectively); and smokers had increasing risk of BASDAI ≥ 4 with increasing years of smoking, or cigarettes per day, or pack-years (p-trend = 0.010, 0.008 and 0.006, respectively). The risk of having active disease was higher in patients who smoked at least 15 cigarettes per day or 15 pack-years (OR = 1.74 [1.06, 2.84] and 2.89 [1.56, 5.35], respectively), with increasing number of cigarettes per day and pack-years. Smokers had an increased risk of BASFI ≥ 4 (p-trend = 0.040 and 0.007, respectively). By meta-analysis, current, former and ever smokers had significantly higher BASDAI (SMD = 0.34 [0.18, 0.48], 0.10 [0.01, 0.19], and 0.27 [0.20, 0.34], respectively) and BASFI (SMD = 0.35 [0.16, 0.55], 0.30 [0.22, 0.39], and 0.35 [0.21, 0.50], respectively) compared to non-smokers. Smoking is a risk factor for greater disease activity and worse functioning in AS patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is one of the most common inflammatory chronic rheumatic diseases throughout the world. It characteristically causes chronic inflammatory back pain, spinal mobility restriction, and in many patients, eventual functional disability [1, 2]. Previous studies have reported the associations of ethnic, geographical, and socioeconomic factors with clinical features of AS [3]. It has been reported that different countries had different prevalences of AS: 0.24% in Europe, 0.17% in Asia, 0.59% in North America, 0.10% in Latin America, and 0.07% in Africa. In addition, male/female ratio of AS was also different (3.8 in Europe, 2.3 in Asia, 6.0 in the USA, and 2.0 in Cuba). The prevalence of AS in China ranges between 0.11 and 0.37% [4,5,6,7,8]. The severity of AS, including disease activity, physical function and inflammation might be influenced by various genetic factors [9,10,11]. Also, environmental factors likely play an important role in disease progression [11].
Smoking is a severe public health problem in China and is one of the major environmental risk factors for rheumatoid arthritis (RA) [12,13,14,15]. Several reports have found some associations between smoking and disease outcomes in AS patients [16, 17]. Two studies observed that AS smokers had a significantly higher Bath AS Disease Activity Index (BASDAI) scores than that in non-smokers in Turkish and Egyptian patients [18, 19], while one report found that current but not former smokers had significantly higher BASDAI scores in Australians [20]. Several other studies reported that smoking had an adverse effect on functional ability in AS [17, 18, 20, 21]. However, there was no significant difference between smokers and non-smokers regarding the BASDAI score in Taiwanese and British patients [17, 21], and Gaber et al. [19] also showed that there was no significant difference between smokers and non-smokers with AS about the Bath AS Functional Index (BASFI) in Egyptian AS patients. In addition, a Norwegian study with 11.2-year-follow-up pointed that current but not former smoking was an important risk factor for AS (OR = 1.99, 95% CI = 1.28–3.11) [22].
Although several studies have analyzed the adverse effect of smoking, the main aspects of the research focused on either smoking status, or duration, or pack-year. Therefore, we aimed to (1) systemically evaluate smoking from different aspects (smoking status, duration, intensity [number of cigarettes per day] and cumulative smoking exposure [pack-years]) and disease outcomes (disease activity, physical function and inflammation) in Chinese AS patients and (2) compare our results of smoking and disease outcomes with previous reports in other studies by meta-analysis.
Materials and methods
Study subjects and data collection
The questionnaire was collected in ten rheumatology departments in the hospitals of Shanghai, Taizhou, Taixing, and Wuxi in China since September of 2010. As of July of 2016, 1359 patients who fulfilled the modified New York criteria (1984) [23] were enrolled and interviewed using questionnaire administered by trained rheumatologists or investigators on site. Patients who did not have smoking information were excluded. This study was approved by the Ethics Committees of the School of Life Sciences of Fudan University, and informed consent was obtained from each participant.
The questionnaire included sociodemographic (such as age, sex, education, and smoking history) and clinical characteristics (such as disease duration, BASDAI, BASFI, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and drug treatments). Furthermore, specific information on smoking including smoking status, smoking duration, and average number of cigarettes per day was also collected. Patients were categorized into non-smokers and ever (former + current) smokers by smoking status. The number of pack-years was calculated (one pack-year = 20 cigarettes per day for 1 year) and divided into three subgroups (0 pack-year, < 15 pack-year, and ≥ 15 pack-year according to cumulative smoking dose) [21], and patients with AS were categorized in three subgroups according to smoking intensity (0 cigarette per day, < 15 cigarettes per day, and ≥ 15 cigarettes per day) [24]. In addition, the patients were also divided into another three groups (0 year, < 15 years, and ≥ 15 years) according to smoking duration. Disease activity and physical function were assessed using the BASDAI [25] and BASFI [26], respectively. A higher score indicated greater disease activity (BASDAI) and adverse functional status (BASFI). In addition, patients were defined as having greater disease activity when the BASDAI was greater than or equal to four [25]; similarly, patients were defined as having an adverse functional status when the BASFI was greater than or equal to four [26]. An elevated ESR was determined when it was higher than 15 mm/h for males and 20 mm/h for females, respectively [27]; CRP was defined as elevated when it was higher than 8 mg/L. Treatment with non-steroidal anti-inflammatory drugs (NSAIDs) were defined as the use of any dose of NSAIDs during previous 3 months. Treatments with any disease-modifying anti-rheumatic drugs (DMARDs) or with any tumor necrosis factor (TNF) blocker were defined as the use of any of these drugs in previous 6 months, and patients with AS took any of the above medicines were defined as “drug treatments” (used as a binary variable). Current smokers were defined as daily smoking of any number of cigarettes, cigars, or pipes.
Literature search
We searched PubMed and China National Knowledge Internet to find relevant studies published before July 2016 using the search terms “ankylosing spondylitis” or “AS” combined with “smoke,” “smokers,” “smoking,” or “pack-year.” Studies were selected if they met the following criteria: (1) they represented an original article, (2) they examined the association of smoking with at least one of the four disease outcomes (BASDAI, BASFI, ESR, or CRP), and (3) titles, abstracts, and full articles were independently screened by two investigators. For every study, the information regarding published data (first author’s, year of publication, journal of publication and the studied population), number and average age of AS cases, and conclusions were extracted.
Statistical analysis
In this analysis, continuous and categorical variables were present as mean with standard deviation (SD) and frequency (%), respectively. Group differences were analyzed by t tests for continuous variables and chi-square tests for categorical variables. Logistic regression was conducted to measure the odd ratios (OR) of different clinical parameters. Clinical manifestations and laboratory test results (such as greater disease activity, adverse functional status, elevated CRP and ESR) were considered as the dependent variables. The different stratification of smoking duration, smoking intensity, and cumulative smoking was defined as independent variables. Gender, age, and drug treatments were considered as covariate variable in multivariable logistic regression. p values for trend (two-sided) were derived from trend tests.
In addition, a meta-analysis was conducted to compare our results with previous reports. A meta-regression model was used to explore source of heterogeneity among studies and the Q statistic was examined to determine any heterogeneity [28]. Stratified analyses were also performed according to different populations. In meta-analysis, P values for heterogeneity over 0.1 illustrated no heterogeneity among studies, and for this case we used a fixed-effect model with inverse variance method to calculate the standardized mean difference (SMD) [29]. When p values for heterogeneity were less than 0.1, the Der-Simonian and Laird method random-effect model was utilized [30]. Through creating funnel plots qualitatively and as measured by Begg’s [31] and Egger’s [32] test, publication biases were examined quantitatively. If the mean disease outcomes (BASDAI, BASFI, CRP and ESR) were not available, the median would be used instead. Similarly, IQRs would be used if SDs were not given. Medians and IQRs were transformed to mean and SDs according to published methods [33]. In case the means (SD) and medians (IQR) were not provided, the studies were excluded in analysis.
All data was carried out by SPSS 22.0 and R (Version 3.2.2: www.r-project.org/). All statistical tests were two-tailed, and a p value of < 0.05 was determined as statistically significant.
Results
Results of our own data: smoking is a risk factor for greater disease activity and worse functioning in Chinese AS patients
A total of 1359 patients with AS were enrolled in our study. After excluding 181 patients who did not have smoking information, the remaining 768 (65.20%) non-smokers, 114 (9.67%) former, and 296 (25.13%) current smokers with AS were analyzed in this study. Sociodemographic and clinical characteristics of patients are shown in Table 1. Males comprised 73.24% of the patients. The average age and age at disease onset were 36.57 ± 12.78 and 29.25 ± 11.48 years old, respectively. The disease duration was 7.33 ± 7.51 years, and 88.67% patients were HLA-B27 positive. The comparison between smoking and non-smoking AS patients is shown in Table 2. Compared with non-smokers, more former smokers had an elevated ESR (p = 0.031) and BASFI ≥ 4 (p = 0.019), while both current and ever smokers had a higher BASDAI score (p = 0.001 or 0.003) and higher frequencies of BASDAI ≥ 4 (p < 0.001 or p = 0.002) and BASFI ≥ 4 (p = 0.022 or p = 0.004) compared to non-smokers.
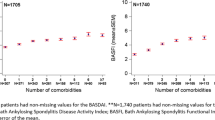
Associations between smoking and disease outcomes are shown in Table 3, revealing the crude and adjusted analytical results of smoking associated with disease outcomes. Independent variables tested in multivariate logistic regression models included age, gender, and drug treatment. Increased smoking intensity, smoking duration, and cumulative smoking exposure were all associated with higher disease activity (p-trend < 0.001) and poorer functioning (p-trend < 0.001) in the unadjusted model.
The association between smoking duration and disease outcome was conducted (Table 3). Compared with non-smokers, the risk of high disease activity was greatest in patients who smoked at least 15 years (OR = 1.70, 95% CI 1.06–2.73, p < 0.05), followed by 0–15 years (OR = 1.58, 95% CI 1.04–2.39, p < 0.05). With increasing years of smoking, smokers had increasing risk of greater disease activity compared with non-smokers (p-trend = 0.010). Nevertheless, there was no association between functional status and smoking duration (p-trend = 0.118).
In addition, the adjusted model (adjusted for age, gender and drug treatment) was also conducted in further analyses (Table 3). Compared with non-smokers, the risk of greater disease activity was highest in patients who smoked at least 15 cigarettes/day (OR = 1.75, 95% CI 1.08–2.82, p < 0.05), followed by 0–15 cigarettes/day (OR = 1.56, 95% CI 1.05–2.33, p < 0.05). Smokers had increasing risk of higher disease activity with increasing smoking intensity (p-trend = 0.008). In addition, the physical function of AS patients was also influenced by smoking intensity. Compared with non-smokers, the OR of poorer function was 2.34 (95% CI 1.51–3.63, p < 0.001) in patients who smoked at least 15 cigarettes/day, and increased smoking intensity predicted an increased risk of worse functioning (p-trend = 0.040).
Cumulative smoking exposure was also analyzed (Table 3). Compared with non-smokers, the risk of greater disease activity was higher in group with 0–15 and ≥ 15 pack-years (OR = 1.68, 95% CI 1.21–2.35, p < 0.01; OR = 2.37, 95% CI 1.34–4.20, p < 0.01, respectively), a greater number of pack-years predicted an increased risk of higher disease activity (p-trend < 0.001), and the risk of functional impairment in patients who smoked at least 15 pack-years was 2.89 (95% CI 1.56–5.35, p < 0.001) compared with non-smokers. With greater number of pack-years, smokers had increasing risk of functional impairment (p = 0.007). However, an association of smoking with higher risk of elevated CRP or ESR was not observed (Table 4).
Meta-analysis showed that smokers have higher BASDAI and BASFI SCORES than non-smokers in AS patients
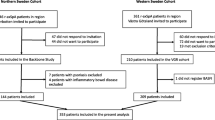
According to the filtering criteria illustrated in Supplemental Fig. 1, nine published studies [11, 16, 17, 19, 21, 34,35,36,37] and our unpublished data set were included in meta-analysis. Among them, six were from Europe [11, 21, 34,35,36,37], two were from China [16, 17], and one was from Egypt [19] (Supplemental Table 1).
Comparison of BASDAI between smokers and non-smokers by meta-analysis
The meta-analysis of BASDAI scores in selected studies is shown in Fig. 1. Compared with non-smokers, significantly higher BASDAI scores were observed in ever smokers (SMD = 0.27, 95% CI 0.20–0.34). When stratified the AS patients into Chinese group and Caucasian group, the analysis showed similar results (SMD = 0.24, 95% CI 0.13–0.34; SMD = 0.31, 95% CI 0.21–0.41, respectively). In addition, current and former smokers had significant higher BASDAI scores than non-smokers (SMD = 0.34, 95% CI 0.18–0.49; SMD = 0.10, 95% CI 0.01–0.19, respectively).

Comparison of BASDAI between smokers and non-smokers in AS patients
Comparison of BASFI between smokers and non-smokers by meta-analysis
The meta-analysis of BASFI scores in the selected studies is shown in Fig. 2. Compared with non-smokers, significantly higher BASFI scores were observed in ever smokers (SMD = 0.35, 95% CI 0.21–0.50). AS patients were divided into Chinese and Caucasian groups, and analysis showed similar results (SMD = 0.22, 95% CI 0.12–0.33; SMD = 0.44, 95% CI 0.34–0.54, respectively). Current and former smokers had significant higher BASFI scores than non-smokers (SMD = 0.35, 95% CI 0.16–0.55; SMD = 0.30, 95% CI 0.22–0.40, respectively).

Comparison of BASFI between smokers and non-smokers in AS patients
No statistically significant difference between smokers and non-smokers by meta-analysis
In a meta-analysis, no statistically significantly different levels of ESR (SMD = 0.00, 95% CI − 0.11–0.10) and CRP (SMD = 0.00, 95% CI − 0.31–0.30) were found between ever smokers and non-smokers (Fig. 3).

Comparison of inflammatory markers between ever and non-smokers in AS patients
Publication bias
Publication bias was examined qualitatively by funnel plots and estimated by Begg’s and Egger’s tests. The p values were 0.86 (BASDAI) and 0.17 (BASFI) in Egger’s test and 0.19 (BASDAI) and 0.86 (BASFI) in Begg’s test. Therefore, no publication bias existed in our study.
Discussion
In this study, we have systemically studied the relationship between smoking and outcomes in patients with AS from different aspects (smoking status, duration, intensity, and cumulative smoking exposure). Our comprehensive analysis of smoking in AS patients indicated that longer smoking duration is associated with higher risk of greater disease activity, and smokers have increasing risk of greater disease activity with increasing smoking years. Higher smoking intensity and cumulative smoking exposure are associated with higher risk of greater disease activity and worse dysfunction in AS patients, and smokers have an increased risk of greater disease activity and worse functional status with increasing smoking intensity and cumulative smoking exposure.
We found that smoking was associated with greater disease activity in Chinese AS patients, which was consistent with previous studies [13, 18, 19, 21]. More specifically, current but not former smokers were associated with increased BASDAI scores, which are also reported in an Australian study of 126 AS patients [20]. In addition, increased smoking duration, smoking intensity, and cumulative smoking exposure were all associated with greater disease activity in our study (p-trend = 0.010, 0.008 and 0.006, respectively). Mattey et al. found that smokers had a dose-response relationship with disease activity in 606 British AS subjects, and it was independent of several confounders (such as age, sex, disease duration and social deprivation) [21]. However, Chen et al. found that the disease activity of AS patients was not affected by smoking duration and cumulative smoking exposure based on a study of 35 smoking patients [17]. In our analysis, we collected 1178 AS patients and the analysis was conducted from different aspects (smoking duration, intensity and cumulative smoking exposure). Besides, similar results were also confirmed in our meta-analysis. Therefore, smoking was associated with greater disease activity in AS patients.
Functional impairment in AS patients was found in current and former smokers in our study; this may suggest irreversible impact of smoking on physical function. Until now, the relationship between smoking and BASFI was inconsistent in many studies. Chen et al. found that both smoking duration and cumulative smoking exposure were associated with physical function in 75 Taiwanese patients with AS [17]. Another study conducted in Australia found a positive relationship with current smoking, but not with cumulative smoking exposure in 126 AS patients [20, 38], while Mattey et al. found that cumulative smoking exposure was associated with higher risk of functional impairment in 606 British AS patients [21]. In our study, both increased smoking intensity and cumulative smoking exposure but not smoking duration were associated with an increased risk of functional impairment (p-trend < 0.001). ESR and CRP levels were not significantly higher in ever smokers than those in non-smokers in logistic and meta-analysis, which was similar with previous studies [13, 35, 38].
Our study has several strengths. It represents the largest sample size of AS patients in the Chinese population with comprehensive clinical and demographic information; on the other hand, it has included information of drug treatment, especially TNF-α inhibitors [39] such as adalimumab [40,41,42], etanercept [43] and infliximab [44] which could improve disease activity and physical function. Interestingly, the effect of smoking on the efficacy of TNF blockers is controversial. One report found that smoking did not influence TNF-α blocker response in Australia [34], while another study illustrated that smokers had poorer TNF blocker treatment response than non-smokers in Danish patients [36]. In order to address these contradictory data, drug treatment was adjusted in our multivariable logistic analysis, and the relationship between smoking and worse BASDAI as well as BASFI scores still remained. In addition, to avoid bias caused by different populations and small sample size, we summarized several previous researches via meta-analysis. However, our study has some limitations as well. Firstly, it is difficult to avoid recall bias when questioned about their disease and smoking status. Secondly, we cannot prove causality because of cross-sectional design in our study. Lastly, including more subjects might have provided a more powerful result in our meta-analyses.
Although several studies have analyzed the adverse effect of smoking, they primarily focused on different aspects of smoking (such as smoking status, or pack-years smoked, or smoking duration). In our study, we have systemically studied the relationship between smoking and outcomes in patients with AS from several different aspects (such as smoking status, duration, intensity and cumulative smoking exposure) using multivariable logistic regression. In addition, in order to compare our results with previous studies, meta-analysis was performed to calculate SMD for relationship between outcomes and smoking status. In conclusion, the adverse effect of smoking is mainly on the disease activity and physical function. In addition, the association of cumulative smoking exposure and smoking intensity with disease activity and physical function is also observed in our AS patients.
References
Corona-Sanchez EG, Munoz-Valle JF, Gonzalez-Lopez L, Sanchez-Hernandez JD, Vazquez-Del Mercado M, Ontiveros-Mercado H, Huerta M, Trujillo X, Rocha-Munoz AD, Celis A et al (2012) −383 A/C tumor necrosis factor receptor 1 polymorphism and ankylosing spondylitis in Mexicans: a preliminary study. Rheumatol Int 32(8):2565–2568. https://doi.org/10.1007/s00296-011-1997-5
Jimenez-Balderas FJ, Mintz G (1993) Ankylosing spondylitis: clinical course in women and men. J Rheumatol 20(12):2069–2072
Dean LE, Jones GT, MacDonald AG, Downham C, Sturrock RD, Macfarlane GJ (2014) Global prevalence of ankylosing spondylitis. Rheumatology (Oxford, England) 53(4):650–657. https://doi.org/10.1093/rheumatology/ket387
Zeng QY, Chen R, Xiao ZY, Huang SB, Liu Y, Xu JC, Chen SL, Darmawan J, Couchman KG, Wigley RD et al (2004) Low prevalence of knee and back pain in southeast China; the Shantou COPCORD study. J Rheumatol 31(12):2439–2443
Dai SM, Han XH, Zhao DB, Shi YQ, Liu Y, Meng JM (2003) Prevalence of rheumatic symptoms, rheumatoid arthritis, ankylosing spondylitis, and gout in Shanghai, China: a COPCORD study. J Rheumatol 30(10):2245–2251
Wigley RD, Zhang NZ, Zeng QY, Shi CS, Hu DW, Couchman K, Duff IF, Bennett PH (1994) Rheumatic diseases in China: ILAR-China study comparing the prevalence of rheumatic symptoms in northern and southern rural populations. J Rheumatol 21(8):1484–1490
Liao ZT, Pan YF, Huang JL, Huang F, Chi WJ, Zhang KX, Lin ZM, Wu YQ, He WZ, Wu J et al (2009) An epidemiological survey of low back pain and axial spondyloarthritis in a Chinese Han population. Scand J Rheumatol 38(6):455–459. https://doi.org/10.3109/03009740902978085
Ye Z, Zhuang J, Wang X, Li J, Zhang L (2006) Epidemiological survey on prevalence of ankylosing spondylitis in 5992 Shenzhen inhabitants. Chin J Clin Rheumatol 10:159–161
Joo YB, Bang SY, Kim TH, Shim SC, Lee S, Joo KB, Kim JH, Min HJ, Rahman P, Inman RD (2014) Bone morphogenetic protein 6 polymorphisms are associated with radiographic progression in ankylosing spondylitis. PLoS One 9(8):e104966. https://doi.org/10.1371/journal.pone.0104966
Cortes A, Maksymowych WP, Wordsworth BP, Inman RD, Danoy P, Rahman P, Stone MA, Corr M, Gensler LS, Gladman D, Morgan A, Marzo-Ortega H, Ward MM, SPARCC (Spondyloarthritis Research Consortium of Canada)., TASC (Australo-Anglo-American Spondyloarthritis Consortium), Learch TJ, Reveille JD, Brown MA, Weisman MH (2015) Association study of genes related to bone formation and resorption and the extent of radiographic change in ankylosing spondylitis. Ann Rheum Dis 74(7):1387–1393. https://doi.org/10.1136/annrheumdis-2013-204835
Ramiro S, Landewe R, van Tubergen A, Boonen A, Stolwijk C, Dougados M, van den Bosch F, van der Heijde D (2015) Lifestyle factors may modify the effect of disease activity on radiographic progression in patients with ankylosing spondylitis: a longitudinal analysis. RMD Open 1(1):e000153. https://doi.org/10.1136/rmdopen-2015-000153
Lu B, Rho YH, Cui J, Iannaccone CK, Frits ML, Karlson EW, Shadick NA (2014) Associations of smoking and alcohol consumption with disease activity and functional status in rheumatoid arthritis. J Rheumatol 41(1):24–30. https://doi.org/10.3899/jrheum.130074
Chung HY, Machado P, van der Heijde D, D'Agostino MA, Dougados M (2012) Smokers in early axial spondyloarthritis have earlier disease onset, more disease activity, inflammation and damage, and poorer function and health-related quality of life: results from the DESIR cohort. Ann Rheum Dis 71(6):809–816. https://doi.org/10.1136/annrheumdis-2011-200180
Papadopoulos NG, Alamanos Y, Voulgari PV, Epagelis EK, Tsifetaki N, Drosos AA (2005) Does cigarette smoking influence disease expression, activity and severity in early rheumatoid arthritis patients? Clin Exp Rheumatol 23(6):861–866
Wolfe F (2000) The effect of smoking on clinical, laboratory, and radiographic status in rheumatoid arthritis. J Rheumatol 27(3):630–637
Zhang S, Li Y, Xu X, Feng X, Yang D, Lin G (2015) Effect of cigarette smoking and alcohol consumption on disease activity and physical functioning in ankylosing spondylitis: a cross-sectional study. Int J Clin Exp Med 8(8):13919–13927
Chen CH, Chen HA, Lu CL, Liao HT, Liu CH, Tsai CY, Chou CT (2013) Association of cigarette smoking with Chinese ankylosing spondylitis patients in Taiwan: a poor disease outcome in systemic inflammation, functional ability, and physical mobility. Clin Rheumatol 32(5):659–663. https://doi.org/10.1007/s10067-013-2165-y
Kaan U, Ferda O (2005) Evaluation of clinical activity and functional impairment in smokers with ankylosing spondylitis. Rheumatol Int 25(5):357–360. https://doi.org/10.1007/s00296-004-0451-3
Gaber W, Hassen AS, Abouleyoun II, Nawito ZO (2015) Impact of smoking on disease outcome in ankylosing spondylitis patients. Egypt Rheumatol 37(4):185–189. https://doi.org/10.1016/j.ejr.2014.11.008
Reed MD, Dharmage S, Boers A, Martin BJ, Buchanan RR, Schachna L (2008) Ankylosing spondylitis: an Australian experience. Intern Med J 38(5):321–327. https://doi.org/10.1111/j.1445-5994.2007.01471.x
Mattey DL, Dawson SR, Healey EL, Packham JC (2011) Relationship between smoking and patient-reported measures of disease outcome in ankylosing spondylitis. J Rheumatol 38(12):2608–2615. https://doi.org/10.3899/jrheum.110641
Videm V, Cortes A, Thomas R, Brown MA (2014) Current smoking is associated with incident ankylosing spondylitis—the HUNT population-based Norwegian health study. J Rheumatol 41(10):2041–2048. https://doi.org/10.3899/jrheum.140353
van der Linden S, Valkenburg HA, Cats A (1984) Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 27(4):361–368. https://doi.org/10.1002/art.1780270401
Wilson D, Wakefield M, Owen N, Roberts L (1992) Characteristics of heavy smokers. Prev Med 21(3):311–319. https://doi.org/10.1016/0091-7435(92)90030-L
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A (1994) A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 21(12):2286–2291
Calin A, Garrett S, Whitelock H, Kennedy LG, O'Hea J, Mallorie P, Jenkinson T (1994) A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol 21(12):2281–2285
Adomaviciute D, Pileckyte M, Baranauskaite A, Morvan J, Dadoniene J, Guillemin F (2008) Prevalence survey of rheumatoid arthritis and spondyloarthropathy in Lithuania. Scand J Rheumatol 37(2):113–119. https://doi.org/10.1080/03009740701774966
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558. https://doi.org/10.1002/sim.1186
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22(4):719–748
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188. https://doi.org/10.1016/0197-2456(86)90046-2
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50(4):1088–1101. https://doi.org/10.2307/2533446
Sterne JA, Egger M (2001) Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol 54(10):1046–1055. https://doi.org/10.1016/S0895-4356(01)00377-8
Wiebe N, Vandermeer B, Platt RW, Klassen TP, Moher D, Barrowman NJ (2006) A systematic review identifies a lack of standardization in methods for handling missing variance data. J Clin Epidemiol 59(4):342–353. https://doi.org/10.1016/j.jclinepi.2005.08.017
Kydd AS, Chen JS, Makovey J, Chand V, Henderson L, Buchbinder R, Lassere M, March LM (2015) Smoking did not modify the effects of anti-TNF treatment on health-related quality of life among Australian ankylosing spondylitis patients. Rheumatology (Oxford, England) 54(2):310–317. https://doi.org/10.1093/rheumatology/keu314
Sakellariou GT, Anastasilakis AD, Kenanidis E, Potoupnis M, Tsiridis E, Savvidis M, Kartalis N, Sayegh FE (2015) The effect of smoking on clinical and radiographic variables, and acute phase reactants in patients with ankylosing spondylitis. Rheumatol Int 35(12):2109–2114. https://doi.org/10.1007/s00296-015-3381-3
Glintborg B, Hojgaard P, Lund Hetland M, Steen Krogh N, Kollerup G, Jensen J, Chrysidis S, Jensen Hansen IM, Holland-Fischer M, Hojland Hansen T et al (2016) Impact of tobacco smoking on response to tumour necrosis factor-alpha inhibitor treatment in patients with ankylosing spondylitis: results from the Danish nationwide DANBIO registry. Rheumatology (Oxford, England) 55(4):659–668. https://doi.org/10.1093/rheumatology/kev392
Jones GT, Ratz T, Dean LE, Macfarlane GJ, Atzeni F (2016) In axial spondyloarthritis, never smokers, ex-smokers and current smokers show a gradient of increasing disease severity—results from the Scotland Registry for Ankylosing Spondylitis (SIRAS). Arthritis Care Res
Ward MM, Weisman MH, Davis JC Jr, Reveille JD (2005) Risk factors for functional limitations in patients with long-standing ankylosing spondylitis. Arthritis Rheum 53(5):710–717. https://doi.org/10.1002/art.21444
Spadaro A, Lubrano E, Marchesoni A, D'Angelo S, Ramonda R, Addimanda O, Perrotta FM, Olivieri I, Punzi L, Salvarani C (2013) Remission in ankylosing spondylitis treated with anti-TNF-alpha drugs: a national multicentre study. Rheumatology (Oxford, England) 52(10):1914–1919
van der Heijde D, Breban M, Halter D, DiVittorio G, Bratt J, Cantini F, Kary S, Pangan AL, Kupper H, Rathmann SS, Sieper J, Mease PJ (2015) Maintenance of improvement in spinal mobility, physical function and quality of life in patients with ankylosing spondylitis after 5 years in a clinical trial of adalimumab. Rheumatology (Oxford, England) 54(7):1210–1219. https://doi.org/10.1093/rheumatology/keu438
van der Heijde D, Schiff MH, Sieper J, Kivitz AJ, Wong RL, Kupper H, Dijkmans BA, Mease PJ, Davis JC Jr (2009) Adalimumab effectiveness for the treatment of ankylosing spondylitis is maintained for up to 2 years: long-term results from the ATLAS trial. Ann Rheum Dis 68(6):922–929. https://doi.org/10.1136/ard.2007.087270
Huang F, Gu J, Zhu P, Bao C, Xu J, Xu H, Wu H, Wang G, Shi Q, Andhivarothai N, Anderson J, Pangan AL (2014) Efficacy and safety of adalimumab in Chinese adults with active ankylosing spondylitis: results of a randomised, controlled trial. Ann Rheum Dis 73(3):587–594. https://doi.org/10.1136/annrheumdis-2012-202533
Baraliakos X, Haibel H, Fritz C, Listing J, Heldmann F, Braun J, Sieper J (2013) Long-term outcome of patients with active ankylosing spondylitis with etanercept-sustained efficacy and safety after seven years. Arthritis Res Ther 15(3):R67. https://doi.org/10.1186/ar4244
Saougou I, Markatseli TE, Voulgari PV, Drosos AA (2010) Maintained clinical response of infliximab treatment in ankylosing spondylitis: a 6-year long-term study. Joint, bone, spine: Rev Rhum 77(4):325–329
Acknowledgments
Computational support was provided by the High-End Computing Center located at Fudan University.
Funding
The study was supported by research grants from the National Basic Research Program (2014CB541801), National Natural Science Foundation of China (31521003), Ministry of Sciences and Technology (2011BAI09B00), US NIH NIAID U01 (1U01AI090909), International S&T Cooperation Program of China (2013DFA30870), and 111 Project (B13016).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
This study was approved by the Ethics Committees of the School of Life Sciences of Fudan University, and informed consent was obtained from each participant.
Disclosures
None.
Electronic supplementary material
ESM 1
(DOCX 193 kb)
Rights and permissions
About this article

Cite this article
Zhang, H., Wan, W., Liu, J. et al. Smoking quantity determines disease activity and function in Chinese patients with ankylosing spondylitis. Clin Rheumatol 37, 1605–1616 (2018). https://doi.org/10.1007/s10067-018-4016-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-018-4016-3