
Abstract
The clinical features of fibromyalgia are associated with various psychological factors, including stress. We examined the hypothesis that the path that psychological factors follow in influencing fibromyalgia symptoms is through their direct effect on stress. Ninety-eight females with ACR 1990 classified fibromyalgia completed the following questionnaires: The Big 5 Personality Inventory, Fibromyalgia Impact Questionnaire, Perceived Stress Scale, Profile of Mood States, Mastery Scale, and Perceived Control of Internal States Scale. SPSS (PASW version 22) was used to perform basic t tests, means, and standard deviations to show difference between symptom characteristics. Pathway analysis using structural equation modelling (Laavan) examined the effect of stress on the relationships between psychological factors and the elements that define the fibromyalgia phenotype. The preferred model showed that the identified path clearly linked the psychological variables of anxiety, neuroticism and mastery, but not internal control, to the three key elements of fibromyalgia, namely pain, fatigue and sleep (p < 0.001), via the person’s perceived stress. Confusion, however, did not fit the preferred model. This study confirms that stress is a necessary link in the pathway between certain identified, established and significant psychological factors and key fibromyalgia symptoms. This has implications for the understanding of contributing mechanisms and the clinical care of patients with fibromyalgia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stress is thought to play an important role in the development, maintenance and/or exacerbation of fibromyalgia and this association has been the focus of many studies [1–5]. Stress may also result from the symptoms and disabilities that characterize fibromyalgia. Thus, the association of stress with fibromyalgia is complex and multidimensional and its causal role in fibromyalgia remains to be better defined.
Thoughts and emotions as well as the psychological responses can lead to biological reactions, among these being the stress-response. This response is characterized by activation of neuronal, hormonal and behavioural systems, all aimed at preserving or restoring body homeostasis. Among these activations is a direct effect on the central pain processing systems that are relevant to fibromyalgia [6–8].
In this current study, we aimed to amalgamate and explore the relationships found in past studies [2, 9–12] namely pain, fatigue, quality of sleep and cognitive dysfunction and the selected typical key psychological variables that significantly associate with fibromyalgia. These variables include mastery, internal control, coping, thinking styles, anxiety, depression, and personality types, such as neuroticism.
In our previous studies, we have utilized perceived stress as a measure that we feel best reflects the type of stress found in fibromyalgia. That is the person’s appraisal and reaction to everyday stressors in daily life. We have shown that, using this measure, as stress levels increase so do the symptoms of fibromyalgia increase [2]. We hypothesized that certain psychological variables, such as anxiety, mastery and control, will modulate stress in different directions and as a consequence impact the stress-dependent symptoms associated with fibromyalgia. The model used in this study thus comprised a “top-down” view of fibromyalgia with the proposal that psychological factors directly act through their effect on stress to modulate the symptoms of fibromyalgia.
Methods
Patients and ethics
Details of patient recruitment and ethics approval have been previously published [2, 9, 12]. All participants were confirmed by a rheumatologist as fulfilling the ACR 1990 fibromyalgia classification criteria. Patients with concomitant clinical conditions likely to affect their assessment were excluded. Males were excluded due to low numbers. All patients participated voluntarily and no fees were paid.
Ninety-eight female fibromyalgia patients were identified [13, 14]. All participants were sent written information regarding the study along with a consent form which, when signed, was followed by a series of questionnaires. We did not systematically identify co-morbidities, ethnicity or drugs (including nicotine) in all patients and hence these components were not included in the analysis.
Questionnaires
The following questionaries were used according to the methodology of our previous studies [2, 9, 12]: The Big 5 Personality Inventory to assess neuroticism [15]; the Fibromyalgia Impact Questionnaire (FIQ) to assess pain intensity, sleep quality, level of depression and anxiety [16]; the Perceived Stress Scale (PSS) to assess the degree that an individual experiences feeling of being overwhelmed by everyday stressful life events over the previous month [17]; the Profile of Mood States (POMS) to assess confusion [18]; the Perceived Control of Internal States scale (PCOISS) to assess the degree of control based on the individual’s thoughts, feelings and behaviours [19] and the Mastery scale to assess the person’s ability to deal with difficulties and challenges in everyday life [20].
Statistical analysis
Initial descriptive analysis was conducted using SPSS (PASW version 22). t tests, means and standard deviations were used to explore the differences between groups in symptom characteristics. Pathway analysis using structural equation modelling (SEM) was conducted using Laavan (Latent variable analysis) [21]. These models permit inclusion of variables that are correlated with and can be used to predict one or more variables. This SEM approach is advantageous to test if there are interrelationships among observable and latent variables and it is the only technique that can do complete and simultaneous analysis between these variables [22].
Parameter estimates, including factor loadings, path coefficients or direct, indirect and total associations and residual error variance terms for criterion variables, were tested for statistical significance (alpha = .05, two tailed). The following indices were used for goodness of fit of the accepted model: goodness of fit (GFI) 0–1, adjusted goodness of fit (AGFI) 0–1, standardized root mean square residual (SRMR) <0.05, root mean square error of approximation (RMSEA) 0.05–0.08, Tucker-Lewis index (TLI) 0–1 and normal fit index (NFI) 0–1.
Results
The demographics of the group have been detailed in our previous publications [9].
The means (standard deviations) of the study measures were pain 6.34 (2.34), fatigue 7.90 (2.03), sleep quality 7.79 (2.18), confusion 10.14 (4.93), neuroticism 25.95 (5.22), depression 3.76 (2.74), anxiety 4.48 (2.83), internal control 57.48 (9.76), mastery 16.58 (3.21) and perceived stress 28.96 (5.65).
The relationships between the perceived stress score and the FM phenotype namely pain, fatigue, sleep disturbance and confusion are shown in Table 1, along with psychological components identified as the strongest predictors in the relationship between stress and the phenotypes. There is a significant association between stress and all of the fibromyalgia characteristics and all the psychological variables [2].
These variables were used in this subsequent pathway analysis. The key steps in determining the preferred model are shown in Table 2.
The goodness of fit characteristics for this pathway model are shown in Table 3. There is good fit of the preferred final model for all assessed methods except for RMSEA.
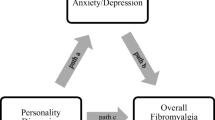
The final preferred theoretical model is shown in Fig. 1.

The final preferred model showing the loadings linking various elements that associate with stress and fibromyalgia
Discussion
We have previously found significant associations between the core clinical features of fibromyalgia, namely pain, sleep disturbance, fatigue and stress in a population of females with fibromyalgia [2, 9–12]. We have also found significant associations between certain psychological characteristics within the same population, and stress [2]. We have shown that psychological variables such as personality, thinking styles, mood and attitude all associate strongly with clinical features of fibromyalgia, and also with stress [9, 10, 12]. Additionally, we have shown that stress also modulates a number of these key psychological processes and characteristic symptoms in females with fibromyalgia [2].
In this current study, we explored indicators that potentially influence the direction of the associated variables in this same patient population. We proposed a “top-down” model suggesting that psychological variables firstly link to stress and this stress then subsequently links to the clinical features of fibromyalgia. Hence, we proposed that psychological variables act through stress to associate with symptoms of fibromyalgia.
In this study, we identified pathways that showed certain psychological variables associated with stress and only through stress did they associate significantly with fibromyalgia symptoms. Furthermore, both anxiety and neuroticism showed a clear association with stress. All elements within the pathway have a strong face validity based on our observations in clinical practice where psychological variables are deemed to modulate fibromyalgia symptoms. The characteristics of these patients appeared typical of those seen in clinical practice and reported elsewhere [23, 24]. Additionally, we feel that the scale used to rate stress in this population appropriately reflects the reaction to everyday stressors that occur in this population.
Higher scores on the Mastery scale associated with less distress, with patients perceiving to be more in control of the situation at hand, but in contrast internal control did not show a significant link in the final pathway model. The internal control scale has a higher cognitive influence than the Mastery scale and may align to the lack of contribution of confusion, one of the key fibromyalgia symptoms, in the model. Further studies of the individual components of each of the scales, rather than the overall validated score that was used in this current analysis, may help explain this finding.
Limitations of our study include the number of patients involved in analysis being at the lower level to achieve robustness of modelling using this technique, and this may explain why the goodness of fit in one domain using the RMSEA was not in the significant range. Nevertheless, the other four goodness of fit appraisals were significant. Additionally, our study was of cross-sectional design which clearly does not specifically assess causal effect relationships. However, of the models that were considered, the most robust one (presented here) would favour psychological elements which are more likely to be derived from everyday life events rather than as a reaction to the condition of fibromyalgia itself.
We feel that appreciation of these associations will aid the understanding of the pathophysiology of fibromyalgia through further studies that link psychological factors involving stress to objective measures of function in fibromyalgia, such as neuroimaging. The clinical management of the person with fibromyalgia will be also be improved if the effects of stress, together with those psychological factors that enhance or modulate stress, are addressed proactively in management.
References
Kivimaki M, Leino-Arjas P, Virtanen M, Elovainio M, Keltikangas-Jarvinen L, Puttonen S et al (2004) Work stress and incidence of newly diagnosed fibromyalgia: prospective cohort study. J Psychosom Res 57(5):417–22
Malin K, Littlejohn GO (2013) Stress modulates key psychological processes and characteristic symptoms in females with fibromyalgia. Clin Exp Rheumatol 31(6 Suppl 79):S64–71
Hassett AL, Clauw DJ (2011) Does psychological stress cause chronic pain? Psychiatr Clin North Am 34(3):579–94
Van Houdenhove B (2005) Premorbid “overactive” lifestyle and stress-related pain/fatigue syndromes. J Psychosom Res 58(4):389–90
Low LA, Schweinhardt P (2012) Early life adversity as a risk factor for fibromyalgia in later life. Pain Res Treat 2012:1–15
Gupta A, Silman AJ (2004) Psychological stress and fibromyalgia: a review of the evidence suggesting a neuroendocrine link. Arthritis Res Ther 6(3):98–106
Thieme K, Turk DC (2012) Cognitive-behavioral and operant-behavioral therapy for people with fibromyalgia. Reumatismo 64(4):275–85
Thieme K, Turk DC, Gracely R, Maxiner W, Flor H (2015) The relationship among psychological and psychophysiological characteristics of fibromyalgia patients. J Pain 16(2):186–96
Malin K, Littlejohn G (2012) Psychological control is a key modulator of fibromyalgia symptoms and comorbidities. J Pain Res 5:463–71
Malin K, Littlejohn G (2012) Neuroticism in young women with fibromyalgia links to key clinical features. Pain Res Treat 10:1–7
Malin K, Littlejohn G (2014) Psychological fibromyalgianess exists on a continuous spectrum. Austin J Orthop Rheumatol 1(1):1–7
Malin K, Littlejohn G (2015) Rumination modulates stress and other psychological processes in fibromyalgia. Eur J Rheumatol 4:143–8
Wolfe F (1989) Fibromyalgia: the clinical syndrome. Rheum Dis Clin North Am 15(1):1–18
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL et al (1990) The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 33(2):160–72
John OP, Robins RW, Pervin LA (1999) The big five personality inventory. In: Pervin LA, John O (eds) Handbook of Personality: Theory and Research. Guilford, New York, pp 103–138
Burckhardt CS, Clark SR, Bennett RM (1991) The fibromyalgia impact questionnaire: development and validation. J Rheumatol 18(5):728–33
Cohen S, Kamararck TRM (1983) A global measure of perceived stress. J Health Soc Behav 2:385–96
McNair D, Lorr M, Droppleman LF (1992) Manual for the profile of mood states. Educational and Industrial Testing Service, San Diego, C.A
Pallant J (2000) Development and validation of a scale to measure perceived control of internal states. J Pers Assess 2:308–37
Pearlin L, Schooler C (1978) The structure of coping. J Health Soc Behav 19:2–21
Rosseel Y (2012) Lavaan an R package for structural equation modeling. J Stat Softw 48(2):1–36
Yanuar F, Ibrahim K, Jemain A (2010) On the application of structural equation modelling for the contrast of a health index. Environ Health Perv Med 15:285–91
Boyer AL, Mira Pastor MA, Calatayud NP, Lopez-Roig S, Cantero Terol MC (2009) Comparing fibromyalgia patients from primary care and rheumatology settings: clinical and psychosocial features. Rheumatol Int 29(10):1151–60
Walen HR, Cronan PA, Bigatti SM (2001) Factors associated with healthcare costs in women with fibromyalgia. Am J Manag Care 7:Spec No:SP39-47
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Rights and permissions
About this article

Cite this article
Malin, K., Littlejohn, G.O. Psychological factors mediate key symptoms of fibromyalgia through their influence on stress. Clin Rheumatol 35, 2353–2357 (2016). https://doi.org/10.1007/s10067-016-3315-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-016-3315-9