
Abstract
This study was conducted to examine the relationship between the degree of asymptomatic hyperuricemia and the development of gout, in men and women. The database of a screening center was searched for all subjects with asymptomatic hyperuricemia (>7.0 mg/dl men, >5.6 mg/dl women) during 2000–2012. We included men and women without previous diagnosis of gout, and a follow-up of at least 5 years. The risk of gout was analyzed in relation to the degree of hyperuricemia at the first visit. Of the 5,234 subjects who matched the inclusion criteria, 4,241 were normouricemic at their first visit and 993 were hyperuricemic. The mean follow up period was 7.5 years. Gout was diagnosed at the last visit in 34 subjects; four in the normouricemia group and 30 in the hyperuricemia group (0.1 % vs. 3.0 %, p < 0.001). Only one woman developed gout. The odds ratio (OR) for developing gout was 32 times higher in the hyperuricemic group than in the normouricemic group. The OR to develop gout was 11.2 (confidence interval [CI] 3.6–35.2) in men with mild hyperuricemia compared to 107.1 (CI 34.2–334.9) in men with moderate hyperuricemia, and 624.8 (CI 134.0–2,913.1) in men with severe hyperuricemia. Multivariate analysis of uric acid levels, thiazide use, regular alcohol consumption and estimated glomerular filtration rate (eGFR) showed that only the level of uric acid retained statistically significant for increasing the risk of gout. There is a strong association between the absolute level of uric acid and the risk to develop gout, strikingly so for men with severe hyperuricemia. Monitoring is recommended for that group, which poses the greatest risk to develop gout.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gout is a painful inflammatory arthritis induced by the deposition of monosodium urate crystals in synovial space and other tissues [1]. Although the association between elevated uric acid levels and gout is well documented [1], the actual risk for developing gout in patients with asymptomatic hyperuricemia is largely unknown. Early studies from the 1960s through the 1980s addressing this issue estimated that two-thirds or more of hyperuricemic individuals will remain asymptomatic [2–4]. Recent epidemiological studies imply that the incidence and prevalence of both gout and hyperuricemia has increased in recent decades [5–11].Several factors may account for the rise in serum uric acid levels. These include a Western diet, rising rates of obesity, increasing diuretic use and an ageing population [1].
There is no consensus on the treatment of patients with asymptomatic hyperuricemia and asymptomatic hyperuricemia is commonly left untreated. This is partly because the majority of patients with hyperuricemia are unlikely to develop gout, and also due to possible side effects of treatment with allopurinol [12, 13]. This approach has not been thoroughly investigated, and is largely based on the findings of the 1987 Normative Aging Study [2] that assessed the risk of asymptomatic hyperuricemic subjects to develop gout. It was estimated in this study, which included only male patients, that 22 % of subjects with uric acid levels higher than 9 mg/dl will develop gout within 5 years.
Due to the paucity of data, the American College of Rheumatology refrained from addressing the pharmacological management of asymptomatic hyperuricemia in its recent guidelines [14].
As the prevalence of gout and hyperuricemia seems to be rising in recent decades, it is imperative to assess the consequence of asymptomatic hyperuricemia and to reexamine the questionable strategy of not treating subjects with asymptomatic hyperuricemia. The aim of this study was to examine the relationship between the degree of asymptomatic hyperuricemia and the risk to develop of gout, in both men and women. As most of those with asymptomatic hyperuricemia will remain asymptomatic, we aimed to identify and characterize those who pose an increased risk to develop gout, in attempt to single out the group who may need close monitoring and possibly treatment.
Subjects and methods
The Recanati Center for Preventive Medicine at Rabin Medical Center in Israel provides a comprehensive annual medical evaluation for males and non pregnant females (ages 20–80 years). In each visit the subjects undergo a thorough medical history, a complete physical examination, a broad range of blood and urine tests, a chest X-ray, an electrocardiogram, an exercise stress test and a lung function test. We retrospectively analyzed the database for all subjects found to have asymptomatic hyperuricemia. Only those with no prior diagnosis of gout and a follow-up period of at least 5 years were included in this study. The study protocol was approved by the Helsinki Ethics Committee of Rabin Medical Center.
Serum uric acid levels were tested in all cases on Beckman Coulter AU 2700, using an enzymatic color test. We defined hyperuricemia as a uric acid level ≥7 mg/dl for men and ≥5.6 mg/dl for women, according to recent literature [15]. The subjects were divided into groups according to their baseline uric acid level: normouricemia (NUA) or hyperuricemia (HUA). The group of HUA was further subdivided into sub-groups according to severity: mild HUA (7–8.4 mg/dl for men and 5.6–6.9 mg/dl for women), moderate HUA (8.5–9.9 mg/dl for men and 7–8.4 mg/dl for women) and severe HUA (>10 mg/dl for men and >8.5 mg/dl for women). We based our classification of severity of HUA on a modification of the classification published by Min et al. in 2009 [16]. The diagnosis of gout at their last visit was established either by documentation from the primary physician or by self-report. We calculated the odds ratio (OR) to develop gout, in both the normal and the high level of uric acid groups, as well as in the sub-groups according to severity of uric acid level.
Statistical analysis
Statistical analysis was performed with SPSS for Windows version 17 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as means ± 1 standard deviation (SD), and categorical variables as percentages. ORs for contracting gout, dependant on baseline variables, were computed by logistic regression. The t-test was used to compare continuous variables between groups, and the chi-square test was used for categorical variables. UA for two groups (Normal/High) groups at baseline were compared using t-test for continuous variables and chi-Square for categorical variables. UA for four groups (Normal/Mild/Moderate/Severe) groups at baseline were compared using ANOVA, with Tukey’s correction for multiple comparisons, for continuous variables. In addition to estimated glomerular filtration rate (eGFR), the following baseline variables were included in the Logistic Regression model: UA Levels, Thiazide usage and Alcohol consumption. As only one Female contracted Gout, Gender was not included in the model.
Results
Of the 5,234 subjects who matched the inclusion criteria, 3,866 (74 %) were males and 1,368 (26 %) were females. Patient characteristics are presented in Table 1. The mean follow up period was 7.53 ± 1.97 years for the normouricemic (NUA) group and 7.68 ± 2 years for the hyperuricemic (HUA) group (p = 0.03). Average age was 42.9 ± 9.1 years for the NUA and 43.7 ± 9.2 years for the HUA group.
At their first visit, 4,241 subjects were found to be NUA and 993 were HUA. At their last visit, gout was diagnosed in 34 patients: four with NUA at the first visit (0.1 %) and 30 with HUA at the first visit (3.1 %, p < 0.001). The OR for developing gout in the HUA group was 32 (confidence interval [CI] 11.3–90.7). When conducting a multivariate analysis comprising of all the variables which were statistically different between normo and hyperuricemic subjects (Table 1), HUA remained a highly significant independent risk factor for gout development.
When conducting a separate analysis for men and women, 3,003 of the men had NUA at their first visit and 863 had HUA. At their last visit, four of the NUA men were diagnosed with gout (0.1 %), compared to 29 of the HUA (3.4 %, p < 0.001). The OR for developing gout was 25.2 times higher in the HUA male group than the NUA male group (CI 8.9–71.6). For the women, 1,238 had NUA and 130 had HUA at their first visit. None of the women in the NUA developed gout, compared to one woman (0.8 %) in the HUA group. Because only one woman developed gout, further statistical analysis was conducted exclusively on the male group.
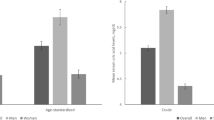
Within the group of men with HUA, the rate of diagnosis of gout at the last visit was identified by the degree of HUA at the first visit (Fig. 1). We found that within the group of men with mild HUA, 1.5 % (11 subjects out 748) were diagnosed with gout at their last visit, whereas 12.5 % (13 subjects out of 104) of the moderate HUA and 45.5 % (five subjects out of 11) of the severe HUA were diagnosed with gout at the end of the study period. The OR to develop gout was 11.2 for men with mild HUA (CI 3.6–35.2), 107.1 for those with moderate HUA (CI 34.2–334.9), and 624.8 for the severe HUA group (CI 134.0–2,913.1).

Prevelance of gout in a mean follow-up of 7.5 years in men by degree of hyperuricemia. Severity of hyperuricemia: mild hyperuricemia, 7–8.4 mg/dl; moderate hyperuricemia, 8.5–9.9 mg/dl; severe hyperuricemia >10 mg/dl
We addressed various risk factors associated with the pathogenesis of gout. In a univariate analysis, gout was diagnosed in 0.8 % of subjects who were being treated with thiazide compared to 0.6 % of those who were not (p = 0.57); and in 1.1 % of subjects regularly consuming alcohol compared to 0.6 % of those who were not (p = 0.11). Gout developed in 0.6 % of subjects with eGFR >60 ml/min/1.73 m2 compared to 3.7 % of those with a lower eGFR (OR 6.19, CI 1.4–26.5, p = 0.048). When these factors, together with uric acid levels, were entered into a multivariate analysis model, only uric acid level retained statistical significance.
Discussion
In this study, we demonstrated that the higher the level of uric acid, the higher the risk for development of gout. Striking results were found regarding the risk to develop gout in the group of men with severe HUA (more than 10 mg/dl). Male subjects were at much higher risk of developing gout independent of whether they had a normal or high level of uric acid. The results of our study are consistent with previous observations that women comprise only a small percentage of the population of gout patients, and that gout is rare in premenopausal women [17]. Previous studies addressing the clinical profile of women with gout found that they often used diuretic therapy and had reduced renal function [18]; they were also found to have a higher prevalence of tophi, with higher levels of uric acid [19]. These findings, however, were based on small samples size (23–37 women). In our study, which included 1,368 women, none of these parameters were found to be associated with gout in women. At the same time, the mean age of women in our study was 43.7 ± 9.4, and only 24.1 % of them were older than 50, thus, most of the females in our study were probably premenopausal. The lower level of uric acid in women can largely be attributed to the presence of estrogen, which promotes its excretion during the reproductive period [20]. Future large scaled studies among postmenopausal women will be helpful in determining the actual risk to develop gout in that group.
Recent epidemiological studies point to an increased prevalence of gout worldwide. A recent retrospective study by Zhu et al. [6] yielded an estimated prevalence rate of 3.9 % in the United States. Hyperuricemia, defined as uric acid >7 mg/dl for men and 5.6 mg/dl for women, was found in 21.4 % of patients and was associated with an increase in comorbidities, including kidney disease, obesity, diabetes mellitus and myocardial infarction. Another study, of a Chinese population, noted a marked increase in the prevalence of HUA and gout from the 1980s to 2008, with current rates being 13.19 % and 1.14 %, respectively [19]. Klemp et al. [10] reported a similar trend in New Zealand, particularly in men [10]. In Maori men, the reported prevalence of gout rose from 4.5–10.4 % to 13.9 %; in European men it rose from 0.7–2.0 % to 5.8 %. In spite of the rising prevalence and incidence of both gout and HUA in recent decades, current data on the actual risk posed by HUA for the development of gout remains sparse. The 1967 Framingham study followed 5,127 subjects (2,283 men, 2,844 women), some already with an established diagnosis of gout [3], and investigated, among other characteristics, the relationship of gout and HUA. In the Framingham study gout developed in 36 % of those with uric acid levels of more than 8 mg/dl. Twenty years later, Langford et al. [21] assessed the effect of thiazide treatment on uric acid and creatinine levels in 3,693 subjects with hypertension. At the end of the 5-year follow-up period, only 15 episodes of gout had been recorded. Average uric acid levels were lower than those in our study (upper quartile 7.7 mg/dl). The significant association of gout with thiazide use was further demonstrated by Choi et al. in 2012 [22]. Similar results were not demonstrated in our study, perhaps owing to the relatively young age of our participants, and the low rate of thiazide use in our subjects. The Normative Aging Study in the late 1980s, which included 2,046 participants, all of them males, found that in subjects with uric acid levels of 9 mg/dl or higher, the cumulative incidence of gout reached 22 % after 5 years [2]. Lin and Chou [23] followed up 223 men with asymptomatic HUA for 5 years at the 1990s and found that 18.83 % of them developed gout, with uric acid levels being the only predictor of gout. In our study, conducted on men and women with no prior diagnosis of gout, we showed that there is a correlation between the degree of HUA and the risk to develop gout. Within a mean follow up of 7.5 years, the OR for males with mild HUA (uric acid 7–8.4 mg/dl) to develop gout relative to males with NUA, was 11.2; the OR for those with moderate HUA (uric acid 8.5–9.9 mg/dl) was 107.1, while men with severe HUA (uric acid >10 mg/dl) had a 624.8 higher risk of gout than those with NUA. The results were further confirmed in a multivariate analysis model which included thiazide use, alcohol consumption and renal function. High uric acid level alone was independently associated with a higher risk of developing gout.
The hyperuricemic subjects in our study were followed for a slightly longer duration than the normouricemic subjects (7.68 vs. 7.53 years). Although statistically significant, and potentially might have contributed to somewhat larger numbers of gout in the HUA group, the difference seems to be clinically minimal and thus unlikely to influence or alter the conclusions of our study. The tendency of our hyperuricemic subjects to have hypertension, high triglyceride levels and higher body mass index is consistent with recent publications regarding the role of uric acid in metabolic syndrome [24]. Regarding the dietary composition of nutrition in Israel, Israel is in the Mediterranean basin, but its population immigrated mostly from Europe, Asia, and Africa. It was estimated in a recent study that about 20 % of Israeli population were High Mediterranean diet consumers [25]. The strengths of our study lie in the large cohort of an apparently healthy population, the long median follow up (>7.5 years) including multiple visits and evaluations, and the inclusion of both men and women. Its weaknesses are that the study was retrospective, the selection bias that implies from the voluntary nature of survey, the fact that diagnosis was established either by documentation from the primary physician or by self-report and the fact that the women population was mostly premenopausal.
In summary, our results singles out the group of men with very high levels of uric acid (of more than 10 mg/dl) as having an exceptionally increased risk to develop gout. Follow-up of that specific group and monitoring their uric acid levels might be beneficial, allowing prompt diagnosis and treatment of an arthritis attack, should it occur. Further prospective studies are needed to establish the role of preventative treatment with allopurinol for that group.
References
Neogi T (2011) Gout. N Engl J Med 364:443–452
Campion EW, Glynn RJ, DeLabry LO (1987) Asymptomatic hyperuricemia. Risks and consequences in the Normative Aging Study. Am J Med 82:421–426
Hall AP, Barry PE, Dawber TR, McNamara PM (1967) Epidemiology of gout and hyperuricemia. A long-term population study. Am J Med 42:27–37
Roubenoff R (1990) Gout and hyperuricemia. Rheum Dis Clin North Am 6:539–550
Trifirò G, Morabito P, Cavagna L, Ferrajolo C, Pecchioli S, Simonetti M et al (2013) Epidemiology of gout and hyperuricaemia in Italy during the years 2005–2009: a nationwide population-based study. Ann Rheum Dis 72:694–700
Zhu Y, Pandya BJ, Choi HK (2012) Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am J Med 125:679–687
Arromdee E (2002) Epidemiology of gout: is the incidence rising? J Rheumatol 29:2403–2406
Roddy E (2007) The changing epidemiology of gout. Nat Clin Pract Rheumatol 3:443–449
Annemans L, Spaepen E, Gaskin M, Bonnemaire M, Malier V, Gilbert T (2008) Gout in the UK and Germany: prevalence, comorbidities and management in general practice 2000–2005. Ann Rheum Dis 67:960–966
Klemp P, Stansfield SA, Castle B, Robertson MC (1997) Gout is on the increase in New Zealand. Ann Rheum Dis 56:22–26
Mikuls T, Farrar JT, Bilker WB, Fernandes S, Schumacher HR Jr, Saag KG (2005) Gout epidemiology: results from the UK General Practice Research Database, 1990–1999. Ann Rheum Dis 64:267–272
Gutiérrez-Macías A, Lizarralde-Palacios E, Martínez-Odriozola P, Miguel-De la Villa F (2005) Fatal allopurinol hypersensitivity syndrome after treatment of asymptomatic hyperuricaemia. BMJ 331:623–624
Hammer B, Link A, Wagner A, Böhm M (2001) Hypersensitivity syndrome during therapy with allopurinol in asymptomatic hyperuricemia with a fatal outcome. Dtsch Med Wochenschr 126:1331–1334
Khanna D, Khanna PP, Fitzgerald JD, Singh MK, Bae S, Neogi T et al (2012) 2012 American College of Rheumatology guidelines for management of gout. Part 2: therapy and antiinflammatory prophylaxis of acute gouty arthritis. Arthritis Care Res (Hoboken) 64:1447–1461
Kratz A, Pesce MA, Fink DJ (2012) Laboratory values of clinical importance. In: Fauci AS, Braunwald E, Kasper D et al (eds) Harrison principles of internal medicine, 18th edn. McGraw Hill, New York, USA, p 3596
Min SI, Yun IJ, Kang JM, Park YJ, Min SK, Ahn C et al (2009) Moderate to severe early onset hyperuricemia: a prognostic marker of long term kidney transplant outcome. Nephrol Dial Transplant 24:2584–2590
Schumacher HR, Chen LX (2012) Gout and other crystal-associated arthropathies. In: Fauci AS, Braunwald E, Kasper D et al (eds) Harrison principles of internal medicine, 18th edn. McGraw Hill, New York, USA, pp 2012–2837
Lally E, Ho G Jr, Kaplan SR (1986) The clinical spectrum of gouty arthritis in women. Arch Intern Med 146:2221–2225
Puig J, Michán AD, Jiménez ML, Pérez de Ayala C, Mateos FA, Capitán CF et al (1991) Female gout. Clinical spectrum and uric acid metabolism. Arch Intern Med 151:726–732
Miao Z, Li C, Chen Y, Zhao S, Wang Y, Wang Z et al (2008) Dietary and lifestyle changes associated with high prevalence of hyperuricemia and gout in the Shandong coastal cities of Eastern China. J Rheumatol 35:1859–1864
Langford HG, Blaufox MD, Borhani NO, Curb JD, Molteni A, Schneider KA et al (1987) Is thiazide-produced uric acid elevation harmful? Analysis of data from the Hypertension Detection and Follow-up Program. Arch Intern Med 47:645–649
Choi HK, Soriano LC, Zhang Y, Rodríguez LA (2012) Antihypertensive drugs and risk of incident gout among patients with hypertension: population based case-control study. BMJ 344:d8190:1–9
Lin KC, Chou P (2000) The interaction between uric acid level and other risk factors on the development of gout among asymptomatic hyperuricemic men in a prospective study. J Rheumatol 27:1501–1505
Cohen E, Krause I, Fraser A, Goldberg E, Garty M (2012) Hyperuricemia and metabolic syndrome: lessons from a large cohort from Israel. IMAJ 14:676–680
Bilenko N, Fraser D, Vardi H, Shai I, Shahar DR (2005) Mediterranean diet and cardiovascular diseases in an Israeli population. Prev Med 40:299–305
Conflict of interest
None of the authors have any conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Duskin-Bitan, H., Cohen, E., Goldberg, E. et al. The degree of asymptomatic hyperuricemia and the risk of gout. A retrospective analysis of a large cohort. Clin Rheumatol 33, 549–553 (2014). https://doi.org/10.1007/s10067-014-2520-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-014-2520-7