
Abstract
The aim of this study is to review over a period of 5 years the clinical spectrum of rheumatic diseases seen in a tertiary hospital in Ouagadougou, Burkina Faso. A retrospective study of case records was conducted from March 1, 2006 to March 30, 2011 in the Rheumatology service, Department of Internal Medicine of the University Hospital Yalgado Ouedraogo. Of the 4,084 patients seen, 2,381 were women (58.30 %) and 1,703 were men (41.70 %). The mean age at disease onset was 42.12 years, ranging from 3 to 92 years. Among the rheumatologic conditions, mechanical and degenerative disorders were the most common, found in 3,053 cases (74.76 %). Among these cases, spinal pathology predominated, especially low back pain (19.93 %). The frequency of osteoarthritis was 19.70 % (804 cases) with a predominance of knee osteoarthritis (657 cases). Infectious pathology was dominated by osteoarticular tuberculosis (48 cases), particularly Pott’s disease (43.68 % of infectious diseases). Among the cases of inflammatory arthritides, rheumatoid arthritis was the leading cause (116 cases or 2.84 %). It was followed by spondyloarthropathies in which arthritis related to HIV predominated (21 out of 81 cases). Metabolic diseases were mainly represented by the gout (162 cases or 3.96 %) with male predominance. Comorbidities included high blood pressure (46.57 %), diabetes mellitus (13.78 %), hemoglobinopathies (9.66 %), epigastric pain (7.25 %), and peptic ulcer confirmed by endoscopy (6.75 %). Rheumatology in Burkina Faso is booming. The profile of rheumatologic diseases in Burkina Faso, after 5 years of practice, confirms the diversity and importance of these conditions dominated by a degenerative pathology of the spine and limbs, including infectious diseases such as Pott’s disease and the inflammatory and metabolic diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rheumatic conditions are a public health problem in developed countries [1]. In Sub-Saharan Africa, they are not a concern due to priority areas such as infections mainly with the human immunodeficiency virus (HIV) and malaria. However, even if the first studies carried out in this part of the world have concluded for the rarity of rheumatic diseases, the work of the last 10 years have reversed that impression [2–6].
Indeed, rheumatoid arthritis (RA) appears frequently in sub-Saharan Africa according to a recent study in the Democratic Republic of Congo [7]. The prevalence of systemic lupus erythematosus is not known but the disease appears to be more severe in sub-Saharan Africa [8]. Spondyloarthropathies seem to be dominated by arthritis associated with HIV infection [9].
In Burkina Faso, rheumatology is a recent specialty. The first consultation is dated March 2006. A first study carried out after 2 years of practice had allowed us to assess the spectrum of rheumatic diseases in the country [10]. Five years later, we found it necessary to study the clinical spectrum of rheumatologic diseases in a rheumatologic department and compare them to other African and Caucasian studies.
Patients and methods
This was a retrospective study of case records conducted from March 2006 to March 2011 in the Department of Internal Medicine, at the University Hospital Yalgado Ouedraogo in Ouagadougou, capital of Burkina Faso. Burkina Faso is a landlocked Sahelian country located in West Africa. Its population was estimated at 14,017,282 inhabitants in 2006 [11]. Ouagadougou (1,475,223 inhabitants), its capital, is the only city in the country with a rheumatology service.
All patients who have had a rheumatology consultation were included, and these patients were examined by the same rheumatologist (O D-D) and have been submitted to a form of data collection with sociodemographic variables (age, sex), disease history, duration of disease progression, the clinical and para-clinical semiology, and the concluded diagnosis.
The diagnosis of the mechanical and degenerative pathologies was radio–clinical, that of the infectious was clinic–biological. All the patients with rheumatoid arthritis, systemic lupus erythematosus, and scleroderma met the ACR criteria [12–14]. Spondyloarthropathies met Amor criteria [15] and rheumatic fever, Duckett Jones criteria [16]. Polymyalgia rheumatica and juvenile idiopathic arthritis fulfilled the appropriate criteria [17, 18]. The diagnosis of tuberculosis osteoarticular was based on presumption argument (night fever, asthenia, weight loss, cold abscess, tuberculin skin test, sensitivity to anti-tuberculosis drug). Gout and fibromyalgia fulfilled the appropriate criteria [19, 20].
Blood count, erythrocyte sedimentation rate, C reactive protein, transaminases, and creatinine were performed in all patients. Anti-citrullinated peptide antibodies, antinuclear, DNA antibodies, and ECT antibodies were made for suspected RA or connective tissue disease. Radiographs of affected joints were made for all patients. Bone densitometry was not performed in all patients. Magnetic resonance imaging was inaccessible. Joint aspiration with cytobacteriological examination and search of microcrystals of joint fluid was performed in all patients with intra-articular effusion. All data were collected on a survey form and processed by Epi Info. Chi-square, Fisher, and Kruskal–Wallis tests were used. Any difference associated with a probability value (p) less than 0.05 was considered statistically significant.
Results
Four thousand one hundred thirty-four patients were recruited during the study period. Four thousand eighty-four had a rheumatic disease. There were 2,381 female patients (58.3 %) and 1,703 male (41.7 %), with male to female ratio of 0.72. The mean age at disease onset was 42.12 years (range 3–92 years). Figure 1 shows the distribution of patients by age and sex. The mean duration between disease onset and diagnosis was 49 ± 7.6 months.

Distribution of patients by age and sex
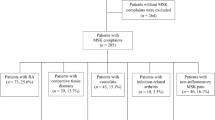
Fifty patients with chest pain associated with gastroduodenal ulcer, hiatal hernia, or heart disease were excluded. Three thousand fifty-three patients (74.76 %) had a mechanical or degenerative disease. Table 1 shows the distribution of patients according to the different disease groups. Among them, the common spine disorders occurred in 1,417 patients (34.71 %). Table 2 shows the distribution of patients according to the mechanical etiologies. Infectious pathology was dominated by osteoarticular tuberculosis (48 cases or 1.17 % of rheumatologic affections); the mean age of patients was 42.5 ± 18.36 years with male to female ratio of 2. Nineteen cases of septic arthritis were reported (0.46 %). Three hundred twenty-six patients (7.98 %) had inflammatory arthritides. Table 3 shows the distribution of patients according to the type of inflammatory arthritis. One hundred sixty-two patients (3.97 %) had gout, and their mean age was 49.9 ± 7.02 years with male to female ratio of 31.4. Four cases of chondrocalcinosis (mean age 67.7 years) and 38 had asymptomatic hyperuricemia. Tumor pathology consisted of eight cases of multiple myeloma (mean age 52.5 years) and two cases of bone metastases. Soft tissue rheumatism was dominated by fibromyalgia (103 cases or 2.52 %); the mean age of the patients was 43.02 years with male to female ratio of 0.69; 40 cases of algodystrophy were observed. Two hundred three patients (4.97 %) had undetermined rheumatism. The mean age of the patients was 32.45 years with male to female ratio of 0.63.
One thousand eight hundred twenty-one patients had comorbidities. High blood pressure was observed in 848 patients (20.76 %). Table 4 shows the distribution of patients with comorbid conditions according to the type of rheumatic disease.
Discussion
Four thousand eighty-four patients were seen in consultation of rheumatology in 5 years. The annual average was 816.8 new patients. Any interpretation of our results must take into account the inherent bias in patient recruitment. Rheumatology consultation is not the only possible consultation of patients with rheumatologic diseases. Some patients have been cared for in orthopedics, traumatology, neurology, or neurosurgery department. An earlier study on the first 2 years of rheumatology practice showed an annual frequency of 719.5 patients per year [10]. This increase in rate is probably due to a better knowledge of the specialty by the populations. Our series included a female predominance (58.3 %). This could be caused by a bias in relation with the structure of the population [11]. However, this frequency is the same with other African countries and reflects the predisposition of women for most rheumatic diseases [3, 21]. The average age of patients at disease onset was 42.12 years; it is the most active age group of the population. Therefore, the functional impact of the disease has major economic consequences for the patient and the country. Mechanical and degenerative disease appears to be the most common rheumatic complaints in Africa [2, 3, 6, 21, 22]. It was dominated by degenerative spine disease. Knee osteoarthritis seems to be the primary site of osteoarthritis in the lower limbs [5]. In our study and in accordance with other African studies, hip osteoarthritis seems to be rare, especially in its primary form. Oniankitan et al. in Togo, however, have reported 46.1 % of primary forms among a series of 89 cases. If the high frequency of knee osteoarthritis seems to be due to genetic factors and obesity, the scarcity of primary hip osteoarthritis could be related to the low incidence of hip dysplasia [23]. The low frequency of hip osteoarthritis has also been suggested to be due to squatting position adapted by many Africans [24].
RA was the commonest chronic inflammatory arthritis (116 cases or 2.84 %), confirming the overall impression of an increase or a better diagnosis of this condition. In fact, Adelowo et al. reported in 2011, 200 cases of RA in 10 years in Nigeria with a hospital frequency of 12.3 % [25]. Recently, Malemba et al. found a RA prevalence of 0.6 %, which is close to that of some European studies [7, 26]. The production of antibodies against citrullinated peptides was associated with the presence of the shared epitope and the disease seemed severe [27, 28]. Spondyloarthropathies were dominated in our series by arthritis related to HIV in accordance with our primary impression [5, 9]. Psoriatic arthritis was rare (only one case) [5, 6, 29]. Ankylosing spondylitis is not rare but seems uncommon [30]. Its association with the antigen HLA B27 * 05 was confirmed by our previous work [31]. In contrast, the high incidence of systemic lupus erythematosus with African blacks reported in the international literature seems questionable. Indeed, its frequency was low (0.6 %) in our series in line with other African studies [32–34]. The frequency of the gout was 3.97 %, which was higher than RA prevalence. The increase of high blood pressure and obesity within the population, probably related to transition in nutrition, could be factors favoring gout [35]. One thousand eight hundred twenty-one patients had a pathological history including 848 cases (46.57 %) of high blood pressure, 132 cases (7.25 %) of epigastralgies, and 123 cases (6.75 %) of peptic ulcer causing therapeutic problems particularly with anti-inflammatory drugs in the long term. Association of high blood pressure, diabetes mellitus type 2, and hemoglobinopathies with the mechanical and degenerative disease needs to be clarified by further studies.
Our work whose objective was to study the clinical spectrum of rheumatologic diseases in a unit of Rheumatology in Burkina Faso includes limits linked to the difficulties of biological examinations with a large part of indefinite rheumatism. In addition, it is the only unit of rheumatology in the country, inaccessibility is also geographical. The insufficient knowledge on the special subject by doctors, often causing the fact that some patients cannot find their way through, and the low number of rheumatologists (only one in this study period) may be factors of undervaluation of the frequencies of different disease. These factors explain the high period between the disease onset and the diagnosis. Our results are not superposable to the country. The high cost of population-based studies limit their realization in our context.
Conclusion
Rheumatology is booming in Burkina Faso. The profile in rheumatologic diseases in Burkina Faso, after 5 years of practice, confirms the diversity and importance of these diseases. Mechanical and degenerative disease, RA, and gout are common. Diseases such as psoriatic arthritis, post-menopausal osteoporosis, and primary hip osteoarthritis seem rare. Population-based studies are needed to confirm this impression.
References
Zeigler LE, Bardin T (2000) The rheumatisms, the world stake in the next decade (2000–2010): the decade of bones and joints. Rev Rhum 67:11–13
Bileckot R, Ntsiba H, Mbongo JA, Masson C, Brégeon C (1992) The rheumatic affections observed in a hospital environment in Congo. Sem Hôp Paris 68(10):282–285
Kouakou N’zué M, N’dri A, Eti E et al (1994) Basic epidemiological data on rheumatology in Ivory Coast hospital. Rhumatologie 46(9):239–242
McGill PE, Njobvu PD (2001) Rheumatology in sub-Saharan Africa. Clin Rheumatol 20:163–167
Mijiyawa M (1993) Bone and joint disorders in black Africa. Rev Rhum 60:451–457
Singwe-Ngandeu M, Meli J, Ntsiba H et al (2007) Rheumatic diseases in patients attending a clinic at a referral hospital in Yaoundé. East Afr Med J 84:404–409
Malemba JJ, Mbuyi-Muamba JM, Mukaya J, Bossuyt X, Verschueren P, Westhovens R (2012) The epidemiology of rheumatoid arthritis in Kinshasa, Democratic Republic of Congo–a population-based study. Rheumatology (Oxford) 51(9):1644–1647
Eti E, Hayem G, De Bandt M, Tubach F (1998) SLE in black patients from Africa and the French West Indies. Spectrum and race differences. Clin Exp Rheumatol 16:762–763
Njobvu PD, McGill PE, Jellis JE, Pobee JOM (1996) Rheumatic disorders at a Zambian teaching hospital. Br J Rheumatol 36(3):400–406
Ouédraogo DD, Yaméogo PS, Tiéno H, Traoré R, Nacoulma EWC, Drabo YJ (2008) Epidemiological profile of the affections observed during the first 2 years of rheumatological practice in the Burkina Faso. [abstract Me 55]. Rev Rhum 75:1150–1151
INSD (2007) Definitive results of the general inventory of the population and the habitation of 2006. INSD, Burkina Faso
Arnett FC, Edworthy SM, Bloch DA et al (1988) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31:315–324
Hochberg MC (1997) Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 40:1725
Preliminary criteria for the classification of systemic sclerosis (scleroderma) (1981) Bull Rheum Dis 31:1–6.
Amor B, Dougados M, Mijiyawa M (1990) Criteria of the classification of spondylarthropathies. Rev Rhum Mal Osteartic 57:85–89
Committee Report of A.H.A (1992) Guidelines for the diagnosis of rheumatic fever, Jones criteria 1992 Update. JAMA 268:2069
Jones JG, Hazleman BL (1981) Prognosis and management of polymyalgia rheumatic. Ann Rheum Dis 40:1–5
Petty RE, Southwood TR, Baum J et al (2004) ILAR Classification of juvenile idiopathic arthritis: second revision, Edmonton 2001. J Rheumatol 31:390–392
Wallace SL, Robinson H, Masi TA, Decker JL, McCarty JD, Yu TF (1977) Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum 20:895–900
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL (1990) The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheum 33:160–172
Slimani S, Amokrane KE, Guellati B, Mohammed-Hadj A, Ladjouze-Rezig A (2008) Epidemiological and clinical characteristics of a consultation Rheumatology in east Algerian. Rev Rhum 75(10–11):1145 [abstract Me 39]
Mijiyawa M, Djagnikpo AK, Agbanouvi AE, Koumouvi K, Agbetra A (1991) Rheumatic diseases seen in hospital outpatient in Lomé (Togo). Rev Rhum 58(5):349–354
Oniankitan O, Kakpovi K, Fianyo E et al (2009) Risk factors of hip osteoarthritis in Lomé, Togo. Med Trop 69(1):59–60
Adebajo AO (1991) Pattern of osteoarthritis in a West African teaching hospital. Ann Rheum Diseases 50:20–22
Adelowo OO, Ojo O, Oduenyi I, Okwara CC (2010) Rheumatoid arthritis among Nigerians: the first 200 patients from a rheumatology clinic. Clin Rheumatol 29:593–597
Guillemin F, Saraux A, Guggenbuhl P et al (2005) Prevalence of rheumatoid arthritis in France—2001. Ann Rheum Dis 64(10):1427–1430
Singwe-Ngandeu M, Finckh A, Bas S, Tiercy JM, Gabay C (2010) Diagnostic value of anti-cyclic citrullinated peptides and association with HLA-DRB1 shared epitope alleles in African rheumatoid arthritis patients. Arth Res Ther 12:1–7
Ouédraogo DD, Singbo J, Diallo O, Sawadogo SA, Tiéno H, Drabo JY (2011) Rheumatoid arthritis in Burkina-Faso: clinical and serological profiles. Clin Rheumatol 30:1617–1621
Ouédraogo DD, Meyer O (2011) Psoriasis arthritis in sub-Saharan African. Joint Bone Spine 79:17–19
Ouédraogo DD, Tiéno H, Kaboré H, Palazzo E, Meyer O, Drabo JY (2009) Ankylosing spondylitis in rheumatology patients in Ouagadougou (Burkina-Faso). Clin Rheumatol 28(12):1375–1377
Diaz-Peña R, Ouedraogo DD, Lopez-Vazquez A, Sawadogo SA, Lopez-Larrea C (2012) Ankylosing spondylitis in three Sub-Saharan populations: HLA-B*27 and HLA-B*14 contribution. Tissue Antigens 80:14–15
Deligny C, Thomas L, Dubreuil F et al (2002) Systemic lupus in Martinique: epidemiological survey. Rev Med Interne 23:21–29
Mijiyawa M, Amanga K, Oniankitan OI, Pitché P, Tchangaï-Walla K (1999) Connective tissue diseases in Africa. Rev Med Interne 20:13–17
Adelowo OO, Oguntona SA (2011) Patten of lupus erythematosus among Nigerians. Clin Rheumatol 28(6):699–603
Mijiyawa M, Bouglouga OE (2003) Hyperuricemie and gout in intertropical area. Rev Rhum 70:152–156
Acknowledgments
We thank Professor Tikly Mohammed, Division of Rheumatology, Chris Hani Baragwanath Academic Hospital, University of the Witwatersrand, Johannesburg, South Africa who read and corrected the English translation of this manuscript.
Disclosures
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ouédraogo, DD., Ntsiba, H., Tiendrébéogo/Zabsonré, J. et al. Clinical spectrum of rheumatologic diseases in a department of rheumatology in Ouagadougou (Burkina Faso). Clin Rheumatol 33, 385–389 (2014). https://doi.org/10.1007/s10067-013-2455-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-013-2455-4