
Abstract
This study aims to determine the level of adherence to treatment in ankylosing spondylitis (AS) patients and to identify possible factors associated to lack of adherence. We included consecutive AS patients (NY modified criteria). Sociodemographic and clinical data were collected. Patients answered auto-reported questionnaires: Bath Ankylosing Spondylitis Disease Activity Index, Bath Ankylosing Spondylitis Functional Index, Ankylosing Spondylitis Quality of Life, and Center for Epidemiological Studies Depression scale. Patients with rheumatoid arthritis (RA) (ACR’87 criteria) were assessed as the control group. The adherence of the studied groups to medical treatment and exercises was measured by means of two questionnaires: Compliance Questionnaire on Rheumatology (CQR) and Exercise Attitude Questionnaire-18 (EAQ-18). The study included 59 patients with AS and 53 patients with RA. Of the AS patients, 43 (72.9 %) were male, median age 47 years (interquartile range (IQR) 33–57) and median disease duration of 120 months (IQR 33–57). Of the RA patients, 37 (69.8 %) were female, had a median age of 56 years (IQR 43.5–60) and a median disease duration of 156 months (IQR 96–288). There were no significant differences in the results of the adherence questionnaires between both groups, with a total median of 68.42 for the CQR in both groups and of 40.7 in AS vs. 42.6 in RA for the EAQ. When dichotomizing patients as adherent and non-adherent, taking as good adherence a cut value in the CQR and EAQ higher than 60, adherence to pharmacological treatment was significantly higher in RA vs. AS (92.5 vs. 74.6 %, p = 0.01) and there were no differences in the EAQ. On the uni- and multivariate analysis, lack of adherence to treatment was not associated to sex, age, disease duration, education, health insurance, depressive status, and disease activity parameters in neither group of patients. AS have an acceptable adherence to pharmacological treatment, although it is lower than RA patients; nonetheless, both groups show a lack of adherence to exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease that primarily affects young adult men and is characterized by the involvement of sacroiliac joints, the spine, hips, and to a lesser extent, peripheral joints. The course of AS is generally progressive with the consequent deterioration of functional capacity and disability related to spinal ankylosis and coxofemoral joints’ involvement. This disease causes a decrease in quality of life and a high socioeconomic impact for both the patient and society. A proper treatment including education, physical therapy exercises, and drugs is essential to achieve a good control of the disease [1–6].
One of the most important determinants in order to fulfill this treatment is the compliance of the patient. Adherence to pharmacological treatment may be evaluated in several ways; there are direct methods such as the determination of drug blood levels and the measurement of biological markers in serum or urine, and indirect methods such as the assessment of clinical response, pill count, and specific questionnaires [7]. To our knowledge, there is only one questionnaire validated on Rheumatology, the “Compliance Questionnaire on Rheumatology (CQR),” which measures the adherence to treatment regimens and identifies factors that determine a suboptimal adherence. Such questionnaire has been validated in a study performed in patients with rheumatoid arthritis, polymyalgia, and gout, where it was compared with a medication electronic monitoring system, showing a sensitivity and specificity of 98 and 67 % to detect good adherence to treatment [8].
Some studies in AS patients determine their adherence to exercise programs, but in no case the evaluation of adherence was the main objective, and its evaluation had not been sufficiently standardized [9, 10]. In order to evaluate the adherence to physical therapy and exercises, a specific questionnaire has been developed, the “Exercise Attitude Questionnaire EAQ-18,” which consists of 18 items and has had a very good acceptance by both patients and experts [11].
Until the present, to our knowledge, there are only two studies that evaluate adherence to medical treatment in AS patients [12, 13] and there are few reports about adherence to physical therapy and/or to an exercise program; such adherence is inferred from the fulfillment of the prescribed plans. For that reason, the objective of our study was to determine the level of adherence to treatment in AS patients and to identify possible factors associated to lack of adherence.
Material and methods
The study included consecutive AS patients according to the New York-modified criteria [14], which attended ambulatory care in a specialized clinic who works on Thursday noon, during the year 2010. Sociodemographic data (age, sex, education, occupation) were collected. Disease activity in AS patients, functional capacity, quality of life, and depression were assessed by Bath Ankylosing Spondylitis Disease Activity Index, Bath Ankylosing Spondylitis Functional Index, Ankylosing Spondylitis Quality of Life, and Center for Epidemiological Studies Depression scale questionnaires, respectively. All of them were culturally adapted and validated in our country [15, 16]. Treatment received was also collected. As a control group, non-selected patients with rheumatoid arthritis (RA) (ACR’87 criteria [17]) from our outpatient clinic were assessed. In RA patient, disease activity was evaluated by Disease Activity Index 28 composite index and functional capacity by Health Assessment Questionnaire-Argentina version [18].
The adherence of the studied groups to medical treatment and exercises was measured by means of two questionnaires: CQR, which measures adherence to pharmacological treatment, and EAQ-18, which measures adherence to exercise. Both questionnaires were previously translated into Spanish by two bilingual physicians and a non-physician person retranslated them into English, demonstrating that they maintained the original features (back translation). The CQR (Appendix 1) consists of 19 items, in which patients have to indicate their level of agreement for certain statements through a Likert scale of four points (strongly disagree, 1 point; somewhat disagree, 2 points; somewhat agree, 3 points; strongly agree, 4 points). Six items present negative statements (no. 4, no. 8, no. 9, no. 11, no. 12, and no. 19); consequently, the score should be reversed (4 = 1, 3 = 2, 2 = 3, 1 = 4). The final score is calculated adding up all items, subtracting 19, and then dividing it by 0.57 in order to take it to a 0–1 scale. With this, an adherence scale that can vary from 0 (no adherence) to 100 (perfect adherence) may be obtained when multiplying it by 100 [8].
The EAQ-18 (Appendix 2) consists of 18 items and answers are scored through Likert scale of four points (strongly disagree, 1 point; somewhat disagree, 2 points; somewhat agree, 3 points; strongly agree, 4 points). Likewise, the score is reverted for negative statements (no. 1, no. 2, no. 3, no. 4, no. 8, no. 9, no. 11, no. 12, no. 13, no. 14, no. 15, no. 16). The final score is calculated adding up all items, subtracting 18, and then dividing it by 0.54 in order to take it to a 0–1 scale; finally, it is multiplied by 100, obtaining a final range from 0 to 100 [11]. CQR and EAQ reproducibility was evaluated in ten patients (five RA and five AS) who completed the questionnaires with 1 week difference and was evaluated by the intraclass correlation coefficient.
For the statistical analysis, a descriptive analysis was performed. Continuous variables were expressed in median and interquartile range (IQR) and compared by Student’s t test and categorical variables were compared by X 2 or Fisher’s exact test. Those variables that in the univariate analysis reached a significance level of <0.1 were included in two multiple linear regression models taking the absolute values of the CQR and the EAQ-18 as dependent variables. Sociodemographic and clinical variables were used as independent variables. In both models, we checked for multicollinearity by the variance inflate factor.
Results
The study included 59 patients with AS and 53 patients with RA. Of the AS patients, 43 (72.9 %) were male, had a median age of 47 years (IQR 33–57) and a median disease duration of 120 months (IQR 33–57). Of the RA patients, 37 (69.8 %) were female, had a median age of 56 years (IQR 43.5–60) and median disease duration of 156 months (IQR 96–288). Features of patients are described in Table 1. Treatments received for AS and RA included: non-steroid anti-inflammatory drugs (NSAIDs), 80 %/68 %; low dose oral steroids, 12 %/51 %; disease-modifying anti-rheumatic drugs (DMARDs), 8.5 %/91 %; and tumor necrosis factor-alpha antagonists, 35.6 %/31 %, respectively.
There were no significant differences in the results of the adherence questionnaires between both groups, CQR median values were 68.42 (IQR 59.6-75.4) for AS patients and 68.42 (IQR 63.15–74.56) for RA patients, and EAQ median values were 40.7 (IQR 5.6–77.8) in AS vs. 42.6 (IQR 5.6–90.7) in RA.
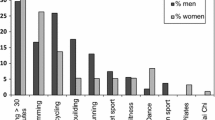
Figures 1 and 2 plot the proportion of AS and RA patients with different scores in CQR and EAQ-18.

Proportion of adherent ankylosing spondylitis and rheumatoid arthritis patients, measured by Compliance Questionnaire on Rheumatology (CQR)

Proportion of adherent ankylosing spondylitis and rheumatoid arthritis patients, measured by Exercise Attitude Questionnaire (EAQ-18)
When dichotomizing patients as adherent and non-adherent, taking as good adherence a cut off value in the CQR and EAQ higher than 60, adherence to pharmacological treatment was significantly higher in RA vs. AS (92.5 vs. 74.6 %, p = 0.01) and there were no differences in the EAQ. On the uni- and multivariate analysis, non-adherent AS patients for CQR were older, had longer disease duration, and had worse depression scores; however, this differences did not reach statistical significance. EAQ scores were almost similar in adherent and non-adherent patients (Table 2).
We look at the adherence scores for patients receiving biologic treatment in both groups (almost 100 % on anti-TNF treatment) compared to patients not receiving these medications. CQR and EAQ scores were higher in patients receiving anti-TNF treatment; however, differences did not reach statistical significance (Table 3).
Discussion
Poor adherence to chronic treatment regimens is very common, contributing to a considerable worsening of the disease and an increase in health care expenditures. Physicians should take into account this factor and improve it by educating the patient, making treatment as simple as possible, and adapting such treatment to the everyday life of the patient [17]. In rheumatic diseases, most compliance studies have been performed in RA [19–22].
To our knowledge, this is the first study that evaluated compliance with pharmacological treatment in AS, using a self-administered questionnaire that evaluates adherence to pharmacological treatment, such as the CQR. No differences were found in the results between AS and RA patients considering absolute values. When dichotomizing the groups as patients adherent and non-adherent to treatment, we detected that RA patients had a significantly higher adherence to pharmacological treatment than those with AS. This could be due the broad therapeutic availability and proven effectiveness in RA, contrary to AS, where pharmacological resources were limited until the arrival of anti-TNF therapies. This data are in accordance with the literature, where previous studies indicate that 60–80 % of patient with RA comply with the treatment [19–22]. A study was performed in 228 RA patients, which the CQR was used to measure adherence to treatment with DMARDs, adherence was of 68 % and it was found that the lack of adherence was associated to a longer disease duration, higher number of perceived adverse events, and belief about the necessity of treatment [19].
Regarding exercises and physical therapy, although there are some works that compare different therapeutic modalities [23–26], to our knowledge, there are no reports that assess patients’ adherence to a physical therapy program with a specific self-questionnaire. Constant physical exercise has shown to be very effective in AS patients. To assess adherence, we chose a self-questionnaire that was easy for our patients to understand and answer, showing a good reproducibility. However we did not discriminate among different types of exercises.
Unfortunately, there is no gold standard for evaluating adherence, and results may vary regarding the instrument that is used to measure such evaluation. Self-questionnaires have the advantage of being a simple, cheap, and fast method; yet, they have the disadvantage of being easy to manipulate by the patient.
This study has some limitations, such as the low number of patients included and the absence of a gold standard for the classification of adherent and non-adherent, which could lead to a possible overestimation of this classification. We consider important to clarify that the response of patients referred to its adherence to medication in general, and we do not discriminate between NSAIDs, DMARDs, and biologics, and no evaluation was performed regarding adverse events. However CQR’s questions refer to the feeling of the patient on the importance of medication for their welfare, irrespective of the medication they receive.
The lack of adherence is a major problem in chronic diseases, and there is a need of developing effective strategies in order to improve it. According to our study, patients with AS have an acceptable adherence to pharmacological treatment, although it is lower than RA patients; nonetheless, both groups show a lack of adherence to exercise. Future studies will be necessary in order to determine reasons related to the lack of adherence.
References
Gran JT, Skomsvoll JF (1997) The outcome of ankylosing spondylitis: a study of 100 patients. Br J Rheumatol 24:908–911
van der Linden S, van der Heijde D (1998) Ankylosing spondylitis. Clinical features. Rheum Dis Clin North Am 24:663–673
Brophy S, Mackay K, Al-Saidi A, Taylor G, Calin A (2002) The natural history of ankylosing spondylitis as defined by radiological progression. J Rheumatol 29:1236–1243
Ward MM (1998) Quality of life in patients with ankylosing spondylitis. Rheum Dis Clin North Am 24:815–826
Ward MM, Weisman M, Davis JC Jr, Reveille JD (2005) Risk factors for functional limitations in patients with long-standing ankylosing spondylitis. Arthritis Rheum (Arthritis Care Res) 53:710–717
Dougados M, Baeten D (2011) Spondyloarthritis. Lancet 377(9783):2127–2137
Osterberg L, Blaschke T (2005) Adherence to medication. N Engl J Med 353:487–497
de Klerk E, van der Heijde D, Landewé R, van der Tempel H, van der Linden S (2003) The compliance-questionnaire-rheumatology compared with electronic medication event monitoring: a validation study. J Rheumatol 30(11):2469–2475
Dagfinrud H, Halvorsen S, Vollestad NK, Niedermann K, Kvien TK, Hagen KB (2011) Exercise programs in trials for patients with ankylosing spondylitis: do they really have the potential for effectiveness? Arthritis Care Res (Hoboken) 63(4):597–603
Gross M, Brabdt KD (1981) Educational support groups of patients with ankylosing spondylitis: a preliminary report. Patient Couns Health Educ 3(1):6–12
Manigandan C, Charles J, Divya I, Edward SJ, Aaron A (2004) Construction of exercise attitude questionnaire-18 to evaluate patients’ attitudes toward exercises. Int J Rehabil Res 27(3):229–231
Barlow JH, Macey SJ, Struthers GR (1993) Health locus of control, self-help and treatment adherence in relation to ankylosing spondylitis patients. Patient Educ Couns 20(2–3):153–166
De Klerk E, van der Linden SJ (1996) Compliance monitoring of NSAID drug therapy in ankylosing spondylitis experiences with an electronic monitoring device. Br J Rheumatol 35:60–65
van der Linden S, Valkenburg HA, Cats A (1984) Evaluation of diagnostic criteria for ankylosing spondylitis: a proposal for the modification of the New York criteria. Arthritis Rheum 27:361–368
Citera G, Maldonado Cocco JA, Moroldo M, et al. (1999) Validación de la versión en español de los cuestionarios de capacidad funcional BASFI y actividad de la enfermedad BASDAI en pacientes con Espondilitis Aquilosante en cuatro países Latinoamericanos. Rev Arg Reumatol (abstract-P 033). CONAR
Marengo MF, Citera G, Schneeberger EE, Maldonado Cocco JA (2008) Work status among patients with ankylosing spondylitis in Argentina. J Clin Rheumatol 14:273–277
Arnett FC, Edworthy SM, Bloch DA et al (1987) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31:315–324
Citera G, Arriola MS, Maldonado-Cocco JA et al (2004) Validation and crosscultural adaptation of an Argentine Spanish Version of the Health Assessment Questionnaire Disability Index. J Clin Rheumatol 10:110–115
Bart JF, van den Bemt BJ, van den Hoogen FH, Benraad B, Hekster YA, van Riel PL, van Lankveld W (2009) Adherence rates and associations with nonadherence in patients with rheumatoid arthritis using disease modifying antirheumatic drugs. J Rheumatol 36(10):2164–2170
Doyle DV, Perrett D, Foster OJ, Ensor M, Scott DL (1993) The long-term use of D-penicillamine for treating rheumatoid arthritis: is continuous therapy necessary? Br J Rheumatol 32:614–617
Pullar T, Peaker S, Martin MF, Bird HA, Feely MP (1988) The use of a pharmacological indicator to investigate compliance in patients with a poor response to antirheumatic therapy. Br J Rheumatol 27:381–384
Brus H, van de Laar M, Taal E, Rasker J, Wiegman O (1999) Determinants of compliance with medication in patients with rheumatoid arthritis: the importance of self-efficacy expectations. Patient Educ Couns 36:57–64
Kraag G, Stokes B, Groh J, Hehewa A, Goldsmith C (1990) The effects of comprehensive home physiotherapy and supervision on patients with ankylosing spondylitis—a randomized controlled trial. J Rheumatol 17(2):228–233
Durmus D, Alayliu G, Cil E, Canturk F (2009) Effects of a home-based exercise program on quality of life, fatigue and depression in patients with ankylosing spondylitis. Rehumatol Int 29(6):673–677
Karapolat H, Eyigor S, Zoghi M, Akkoc Y, Kirazli Y, Keser G (2009) Are swimming or aerobic exercise better than conventional exercise in ankylosing spondylitis patients? A randomized controlled study. Eur J Phys Rehabil Med 45(4):449–457
Gyurcsik ZN, András A, Bodnár N, Szekanecz Z, Szántó S (2012) Improvement in pain intensity, spine stiffness, and mobility during a controlled individualized physiotherapy program in ankylosing spondylitis. Rheumatol Int 32(12):3931–3936
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1
Appendix 1 (English version)

Appendix 1 (Spanish version)

Appendix 2
Appendix 2 (English version)

Appendix 2 (Spanish version)

Rights and permissions
About this article
Cite this article
Arturi, P., Schneeberger, E.E., Sommerfleck, F. et al. Adherence to treatment in patients with ankylosing spondylitis. Clin Rheumatol 32, 1007–1015 (2013). https://doi.org/10.1007/s10067-013-2221-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-013-2221-7