
Abstract
In vivo and in vitro aggrecanases degrade proteoglycan aggrecan in articular cartilage. However, the expression of aggrecanases in patients in different stages of osteoarthritis (OA) has not been investigated. This study detected the expression of a disintegrin and metalloproteinase with thrombospondin motifs 4 (ADAMTS-4) and ADAMTS-5 and their proteolytic products, ARGxx, in the synovial fluid (SF) of patients in different stages of OA. This study aimed to evaluate the expression of aggrecanases and to explore the respective roles of these enzymes in human cartilage degradation. A total of 144 patients with knee OA were divided into early-, middle-, and late-stage OA groups according to the degree of cartilage degradation using Recht’s MRI grading standard and the modified Outerbridge classification system. Expression levels of ADAMTS-4, ADAMTS-5, and ARGxx in the SF from these patients were measured using enzyme-linked immunosorbent assay (ELISA) and Western blot analysis. Our findings showed that ADAMTS-4 and ARGxx expression levels in the early-stage group were significantly higher than in the other two groups. ADAMTS-5 in the early-stage group and ADAMTS-4, ADAMTS-5, and ARGxx in the late-stage group were significantly higher than those in the middle-stage OA group. Both ADAMTS-4 and ADAMTS-5 levels were correlated with ARGxx levels (P < 0.05). The correlation coefficients of ADAMTS-4 and ADAMTS-5 were 0.236 and 0.068, 0.729 and 0.479, and 0.675 and 0.257 in the early-, middle-, and late-stage groups, respectively, and 0.530 and 0.258 in the total SF samples. Western blot analysis revealed that the ADAMTS-4 and ADAMTS-5 in SF were 50 kDa proteins and that ARGxx in SF had at least two molecular masses, 55 kDa and 70 kDa. The expression levels of all three proteins were consistent with the ELISA results. These results suggested that aggrecanases were involved in all stages of human OA aggrecan degradation, especially in the early and late stages. ADAMTS-4 levels were higher in early- compared with middle- or late-stage OA and were also more correlated with ARGxx than ADAMTS-5; thus, ADAMTS-4 might be the principal aggrecanase of aggrecan degradation in human OA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) is a progressive degenerative disease of synovial joints characterized by the erosion of articular cartilage in which depletion of aggrecan is a crucial initial pathological event [1]. Aggrecanases and matrix metalloproteinases (MMPs) are two key families of enzymes that degrade aggrecan and type II collagen in the articular cartilage matrix [2, 3]. In vivo and in vitro cartilage explant experiments have revealed that aggrecanases are the principal proteinases of aggrecan degradation during articular cartilage destruction rather than MMPs [4–6]. A disintegrin and metalloproteinase with thrombospondin motifs 4 (ADAMTS-4) and ADAMTS-5, also named aggrecanase 1 and aggrecanase 2, respectively, are two members of the ADAMTS gene family, and these enzymes play an essential role in aggrecan degradation [7–10]. Although the comparison of aggrecanase-generated neoepitopes in the synovial fluid (SF) in early- and late-stage OA in dogs has been reported [11], the differential expression of aggrecanases and their products in the human synovial fluid during different stages of OA has not been investigated. The relative contribution of individual ADAMTS-4 and ADAMTS-5 proteinases to cartilage destruction during OA has also not been resolved.
We conducted the present study to investigate the levels of ADAMTS-4 and ADAMTS-5 and the proteolytic products of aggrecan ARGxx in the SF of patients during different stages of OA. We used enzyme-linked immunosorbent assay (ELISA) and Western blot analysis and examined the correlation between aggrecanases and ARGxx to evaluate the respective effects of the two enzymes on human aggrecan degeneration.
Patients and methods
Synovial fluid samples
In total, 144 SF samples were collected from the knee OA joints of 144 patients. A routine procedure of suction or aspiration during arthroscopy or intra-articular injection of hyaluronate sodium (HA) or steroid anti-inflammatory drugs was used. Inclusion criteria ensured that the patients had magnetic resonance imaging (MRI) prior to SF aspiration or arthroscopy. Exclusion criteria included any other intra-articular treatment within 2 years and any oral medicines within 1 month of OA treatment. A diagnosis of knee OA was confirmed using radiological and clinical examinations based on the criteria of the American College of Rheumatology [12]. All patients were divided into early-, middle-, and late-stage OA groups according to the degree of cartilage degeneration. Degeneration was assessed using Recht’s grading standard on MRI [13] and the modified Outerbridge classification system [14]. MRI is accurate for cartilage degeneration assessment when using fat-suppressed spoiled gradient-echo and the T1 and T2 mapping sequences [15, 16]. We did not adopt the Kellgreen Lawrence classification because the joint-space width is greatly affected by the position of the joint in the X-ray beam and because it is very difficult to assess early-stage OA cartilage degeneration using an X-ray. The MRI was assessed by one MRI specialist and one orthopedic specialist according to Recht’s grading standard. If the two assessments were different, another MRI specialist was asked to assess. If the patients received arthroscopy, we used the modified Outerbridge classification as the final grading because it has a direct view of the cartilage. The details of the two grade systems are as follows: Recht’s MRI grading criteria—grade 0, normal articular cartilage; grade 1, hierarchical structure of cartilage loss, cartilage appears in the limitations of the low signal area, and cartilage has a smooth surface; grade 2, cartilage surface contours of mild to moderate irregular cartilage defect depth and less than 50 % loss of cartilage thickness; grade 3, cartilage surface profile of moderate to severe irregularities and a depth of cartilage defects that exceeds 50 % but is not completely off; and grade 4, full-thickness cartilage defects, stripping, and subchondral bone quality of exposure with or without subchondral bone signal changes. Modified Outerbridge classification system: grade 0, normal cartilage; grade 1, cartilage softening and/or swelling; grade 2, mild surface fibrillation and/or less than 50 % loss of cartilage thickness; grade 3, severe surface fibrillation and/or loss of more than 50 % of cartilage thickness but without exposure of subchondral bone; and grade 4, complete loss of cartilage with subchondral bone exposure.
The early-stage OA group included patients with Recht’s and Outerbridge grades of 1 and 2 who demonstrated slight cartilage erosion. The major treatments for these patients were oral medicines or intra-articular injections. The middle-stage OA group included patients of grade 3 who demonstrated moderate cartilage erosion for which treatments of intra-articular injection or/and arthroscopy may be needed. The late-stage OA group included patients of grade 4 who demonstrated extensive cartilage erosion, with arthroplasty as the major treatment. Descriptive characteristics and the clinical data of the patients are shown in Table 1. There were 12 patients under the age of 40 years, and all were in the early-stage group.
SF samples were centrifuged at 3,000×g to remove cells and particulate material, and the samples were immediately stored in Eppendorf tubes at −80 °C until use. The study was approved by the ethics committee of our faculty. Written informed consent was obtained from all participants.
Enzyme-linked immunosorbent assay for SF aggrecanases and the proteolytic products of aggrecan
The expression levels of ADAMTS-4, ADAMTS-5, and ARGxx in the synovial fluids were measured using the indirect enzyme-linked immunosorbent assay (ELISA). SF samples were diluted fivefold in a bicarbonate coating buffer (0.05 M, pH 9.6), and 100 μl was incubated in 96-well ELISA plates (Costar, USA) overnight at 4 °C. The ELISA plate wells were washed with 200 μl of PBS, pH 7.4, containing 0.05 % Tween-20 (Sigma) (PBS-T). Washing was done thoroughly and uniformly three times for 3 min, and the plates were then blocked in freshly prepared PBS-T containing 5 % skim milk (BD, Difco, USA) for 1 h at room temperature. The wells were thoroughly and uniformly washed three times with PBS-T. The rabbit polyclonal antibodies against ADAMTS-4 (ab39201) and ADAMTS-5 (ab41037) and mouse monoclonal antibody [BC-3] to aggrecan ARGxx (ab3773) were purchased from Abcam (USA). The primary antibodies were diluted with PBS-T according to the manufacturer’s instructions. The dilutions of these three antibodies were 1:1,000, 1:500, and 1:300, respectively. Antibody dilutions were added to the microplates and incubated for 2 h at 37 °C. The wells were washed three times with PBS-T and 100 μl of goat anti-rabbit IgG (whole molecule) or goat anti-mouse IgG (Fab specific) alkaline phosphatase-conjugated antibody (Sigma). A 2,000-fold dilution was added to the wells for 1 h at 37 °C. The plate was developed after a final wash with PBS-T by the addition of the alkaline phosphatase yellow (pNPP) liquid substrate system for ELISA (Sigma). An ELISA plate reader (Bio-Tek) was used to measure the reaction absorbance at 405 nm. The ELISA results are presented as optical densities (OD).
Quantification of SF aggrecanases and the proteolytic products of aggrecan using Western blot analysis
Twenty four SF samples were chosen randomly from the three groups, resulting in eight per group, for Western blot analysis. The SF samples were centrifuged at 3,000×g for 10 min at 4 °C. The supernatant fluids were collected, and the BCA Protein Assay Kit (Beyotime, Jianshu, China) was used to measure the total protein concentrations of the samples. SF samples with equal amounts of protein (1.6 μg) were treated with sodium dodecyl sulfate loading buffer (Beyotime, Jianshu, China) and boiled for 5 min at 100 °C. The PageRuler™ Prestained Protein Ladder (Fermentas) was used as the molecular weight standard. The samples were analyzed using sodium dodecyl sulfate polyacrylamide gel electrophoresis on 8–12 % polyacrylamide gels, and the separated proteins were transferred to polyvinylidene fluoride (PVDF) membranes (Millipore, USA). The PVDF membranes were blocked in freshly prepared Tris-buffered saline (pH 7.6) and 5 % skim milk containing 0.05 % Tween-20 for 1 h at room temperature. The membranes were incubated with primary antibodies against ADAMTS-4, ADAMTS-5, and ARGxx as described above and incubated overnight at 4 °C. The membranes were washed three times for 10 min with Tris-buffered saline buffer, pH 7.6, containing 0.05 % Tween-20 (Sigma) (TBST) and incubated with a 5,000-fold dilution of goat anti-rabbit IgG or goat anti-mouse IgG linked to alkaline phosphatase (Sigma) as the secondary antibody for 1 h at 37 °C. The immunosignals were visualized after a final wash with TBST with a BCIP/NBT alkaline phosphatase color development kit (Beyotime, Jianshu, China) according to the manufacturer’s instructions. A mouse anti-gylceraldehyde-3-phosphate dehydrogenase (GAPDH) antibody (Santa Cruz, USA) at a 1:1,000 dilution standardized and normalized the loading of SF samples into each well. Protein expression was quantified using Quantity One software (BIO-RAD, USA), version 4.6.2.
Statistical analysis
The expression levels of ADAMTS-4, ADAMTS-5, and the proteolytic products of aggrecan, ARGxx, in SF are presented as the mean ± standard deviation (SD). Data were first checked for normality. ADAMTS-4 and ADAMTS-5 met the assumption of normal distribution, but ARGxx did not. Differences in ADAMTS-4 and ADAMTS-5 among the three groups were compared by one-way ANOVA. Differences in the expression levels of ARGxx among the three groups were compared by the Kruskal–Wallis test. The LSD test was used to compare the expression differences between groups. The associations of aggrecanases and the proteolytic products of aggrecan were analyzed using correlation analysis. Differences with a two-sided P value of less than 0.05 were considered significant. All statistical analyses were performed using IBM SPSS software (Chicago, USA) for Windows, version 19.0.
Results
Expression levels of ADAMTS-4, ADAMTS-5, and ARGxx in SF using ELISA
The expression levels of ADAMTS-4 and ARGxx in the SF in the early-stage OA group were significantly higher than in the middle- and late-stage OA groups (P < 0.01 and P < 0.0001, respectively) (Fig. 1). The expression levels of ADAMTS-4 and ADAMTS-5 in the early- and late-stage OA groups were also significantly higher than in the middle-stage OA group (P < 0.01). ARGxx expression in late-stage OA was higher than in the middle-stage group (P < 0.0001). ADAMTS-5 expression was significantly higher than ADAMTS-4 in all three groups (P < 0.01) (Table 2). However, ADAMTS-4 expression levels were positively correlated with ARGxx levels in all three groups. ADAMTS-5 only positively correlated with ARGxx in the first two groups. The correlation coefficients of ADAMTS-4 and ADAMTS-5 were 0.236 and 0.068, 0.729 and 0.479, and 0.675 and 0.257 in the early-, middle-, and late-stage groups, respectively (Fig. 2). The overall SF correlation coefficients of ADAMTS-4 and ADAMTS-5 were 0.530 and 0.258, respectively.

Comparison of the expression levels of ADAMTS-4, ADAMTS-5, and ARGxx in synovial fluid from patients at different stages of OA using ELISA. ADAMTS-4, ADAMTS-5, and ARGxx expressions are represented as optical density (OD) values at 405 nm. A P value of less than 0.05 was considered statistically significant. Single asterisk (*) P < 0.01 compared with the middle- and late-stage OA groups; double asterisk (**) P < 0.01 compared with the middle-stage OA group; white-filled triangle (△) P < 0.0001 compared with the middle- and late-stage OA groups; number sign (#) P < 0.0001 compared with the middle-stage OA groups

The correlation between the levels of ADAMTS-4, ADAMTS-5, and ARGxx in SF of OA patients. A P value of less than 0.05 was considered statistically significant
These results suggested that aggrecanases were involved in all stages of human OA aggrecan degradation, especially in the early and late stages. The ADAMTS-4 level was higher in the early compared with the middle and late stages; it was also more correlated with ARGxx than ADAMTS-5, although the ADAMTS-5 expression levels were higher than ADAMTS-4 in all three groups. ADAMTS-4 may be the principal aggrecanase in the human OA pathological process.
Western blot analysis of ADAMTS-4, ADAMTS-5, and ARGxx in SF
The expression levels of ADAMTS-4, ADAMTS-5, and the aggrecan products in the three groups were quantified using Western blotting. The expression of ADAMTS-4 (50 kDa) in the SF samples of early-stage OA patients was significantly elevated compared with the middle- and late-stage OA groups (P < 0.05). ADAMTS-5 (50 kDa) expression levels were higher in the early- and late-stage OA groups than in the middle-stage OA group (P < 0.05). Full-length ADAMTS-4 (90 kDa) and ADAMTS-5 (102 kDa) were not detectable in the synovial fluids. A major protein band (approximately 70 kDa) and weak protein band (approximately 55 kDa) were detected with the anti-aggrecan ARGxx antibody [BC-3]. ARGxx expression levels were greater in the early- and late-stage OA groups than the middle-stage OA group (P < 0.05). These results are expressed as protein levels relative to GAPDH protein levels in Table 3 and Fig. 3.

Expression levels of ADAMTS-4, ADAMTS-5, and ARGxx in synovial fluids from patients at different stages of OA using Western blotting. Synovial fluid samples with equal amounts of total proteins from the synovial fluid of OA joints in the early stage (lane 1), middle stage (lane 2), and late stage (lane 3) were loaded into each well. The arrows indicate the molecular weights of the proteins. A mouse anti-GAPDH (37 kDa) antibody normalized the loading of synovial fluid samples into each well
These results were consistent with our ELISA results. They suggest that at least two ARGxx molecular weights exist in human OA SF but that no full-length aggrecanases exist in human OA SF.
Discussion
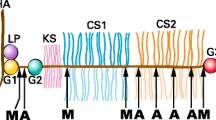
Articular cartilage is a connective tissue composed of chondrocytes embedded in the extracellular matrix, which is composed of two major components: type II collagen and the proteoglycan aggrecan. The depletion of aggrecan due to proteolytic cleavage in articular cartilage is the initial event in OA development, followed by the irreversible breakdown of collagen [17, 18]. It has been reported that aggrecanases play a crucial role in aggrecan degradation in cartilage, which occurs in the interglobular domain (IGD) of the aggrecan core protein [4, 5, 19]. Two major cleavage sites exist within the IGD of the core protein in the matrix depletion from cartilage [20–22]. Aggrecan cleavage between Glu373 and Ala374 in the IGD by aggrecanases generates two fragments of G1-EGE and ARGxx with most glycosaminoglycans, which are essential for the binding of aggrecanase and aggrecan and their escape from articular cartilage [23]. Therefore, the levels of ARGxx fragments can represent the effects of aggrecanases in cartilage degradation.
The effect of aggrecanases on the pathology of cartilage degradation has been investigated in vivo [24–28] and in vitro [26, 28–31], but the significance of aggrecanases in cartilage erosion under pathological environments in humans is unclear. No comparative studies of aggrecanases in the synovial joints of patients in different stages of OA have been reported. Our study showed that ADAMTS-4 levels were higher in early- compared with middle- and late-stage OA; ADAMTS-4 may be the principal aggrecanase in the human OA pathological process. This result supports the viewpoint that the depletion of aggrecan is the initial event in OA development [17, 18]. Our results also demonstrated that ADAMTS-4, ADAMTS-5, and ARGxx existed in all stages of OA SF, and their levels were prominently expressed during the early and late stages of human OA. Therefore, the inhibition of aggrecanases may not only prevent the pathogenesis of human OA but may also slow its progression. These results support a theoretical basis for the development of aggrecanase inhibitors as a therapeutic intervention in arthritic diseases. The expression levels of ADAMTS-4, ADAMTS-5, and ARGxx might be affected by the volume of synovial fluids, age of the patient, and synovium-generated aggrecanases [24]. The correlations between aggrecanases and ARGxx, however, were not affected by these factors. The significance of the two most important and effective aggrecanases in aggrecan degradation remains debatable. The relative contribution of individual ADAMTS-4 and ADAMTS-5 proteinases to cartilage destruction during OA has not been resolved. Previous results from mouse knockout studies have demonstrated that ADAMTS-5 but not ADAMTS-4 knockout mice were protected from aggrecan depletion and cartilage erosion in OA and cytokine-stimulated articular cartilage [27, 28]. These experiments suggested that ADAMTS-5 is the major aggrecanase of mouse cartilage degradation in vivo and in vitro, although a study of ADAMTS-4 and ADAMTS-5 double-knockout mice revealed that novel aggrecan-degrading activity remained in the cartilage [29]. However, several in vitro experiments in bovine cartilage [30] and a porcine chondrocyte culture system [31] have demonstrated that ADAMTS-4 plays a significant role in aggrecan catabolism. Kamm et al investigated and compared the expression of several cytokines and catabolic enzymes in the synovial membrane, SF, and articular cartilage from normal and naturally osteoarthritic joints from horses. They concluded that ADAMTS-4 may be the primary aggrecanase responsible for degrading cartilage in OA [32]. An in vitro study of human cartilage using small interfering RNA demonstrated that both ADAMTS-4 and ADAMTS-5 contribute to the characteristic cartilage damage of human OA [10]. In this study, we demonstrated that ADAMTS-4 levels were positively correlated with ARGxx levels in all three groups and that the correlation coefficients were significantly higher than that of ADAMTS-5, although ADAMTS-5 expression was significantly higher than ADAMTS-4 in all three groups. This result suggested that ADAMTS-4 plays a more significant role than ADAMTS-5 in aggrecan degradation in human arthritis. This finding contradicts the results of some studies in mice [27, 28] and is consistent with some in vitro studies in bovine [30, 31], horse [32], and human cartilage [10].
The proteolytic activity of ADAMTS-5 was approximately 1,000-fold greater than ADAMTS-4 under physiological conditions in vitro, and the ADAMTS-5 with the highest proteolytic activity was 80 kDa [33]. In our study, only 50 kDa ADAMTS-4 and ADAMTS-5 were detected in human OA SF. Therefore, ADAMTS-5 was not fully activated in human OA SF. Protease activity is affected by a series of molecular events, including promoter activity, the regulation of non-coding RNA, transcriptional regulation, post-translational processing, and alternative splicing. Whether the aggrecanase mRNA expression levels in OA cartilage were up-regulated [24] or down-regulated [26] when compared with “normal” cartilage remains unclear. Therefore, further research on aggrecanases, especially their activation mechanisms and inhibitors, is required to fully elucidate the pathogenic mechanisms of arthritis. ADAMTS-4 may be a more attractive target for anti-arthritis drugs for human OA prevention and treatment.
Abbreviations
- ADAMTS:
-
A disintegrin and metalloproteinase with thrombospondin motifs
- ELISA:
-
Enzyme-linked immunosorbent assay
- MMP:
-
Matrix metalloproteinase
- OA:
-
Osteoarthritis
- SF:
-
Synovial fluid
References
Martel-Pelletier J, Boileau C, Pelletier JP, Roughley PJ (2008) Cartilage in normal and osteoarthritis conditions. Best Pract Res Clin Rheumatol 22:351–384
Roberts S, Hollander AP, Caterson B, Menage J, Richardson JB (2001) Matrix turnover in human cartilage repair tissue in autologous chondrocyte implantation. Arthritis Rheum 44:2586–2598
Struglics A, Larsson S, Pratta MA, Kumar S, Lark MW, Lohmander LS (2006) Human osteoarthritis synovial fluid and joint cartilage contain both aggrecanase- and matrix metalloproteinase-generated aggrecan fragments. Osteoarthritis Cartilage 14:101–113
Durigova M, Nagase H, Mort JS, Roughley PJ (2011) MMPs are less efficient than ADAMTS5 in cleaving aggrecan core protein. Matrix Biol 30:145–153
Karsdal MA, Madsen SH, Christiansen C, Henriksen K, Fosang AJ, Sondergaard BC (2008) Cartilage degradation is fully reversible in the presence of aggrecanase but not matrix metalloproteinase activity. Arthritis Res Ther 10:R63
Little CB, Hughes CE, Curtis CL, Janusz MJ, Bohne R, Wang-Weigand S, Taiwo YO, Otterness IG, Mitchell PG, Flannery CR, Caterson B (2002) Matrix metalloproteinases are involved in C-terminal and interglobular domain processing of cartilage aggrecan in late stage cartilage degradation. Matrix Biol 21:271–288
Bayliss MT, Hutton S, Hayward J, Maciewicz RA (2001) Distribution of aggrecanase (ADAMts 4/5) cleavage products in normal and osteoarthritic human articular cartilage: the influence of age, topography and zone of tissue. Osteoarthritis Cartilage 9:553–560
Bondeson J, Wainwright S, Hughes C, Caterson B (2008) The regulation of the ADAMTS4 and ADAMTS5 aggrecanases in osteoarthritis: a review. Clin Exp Rheumatol 26:139–145
Sandy JD, Verscharen C (2001) Analysis of aggrecan in human knee cartilage and synovial fluid indicates that aggrecanase (ADAMTS) activity is responsible for the catabolic turnover and loss of whole aggrecan whereas other protease activity is required for C-terminal processing in vivo. Biochem J 358:615–626
Song RH, Tortorella MD, Malfait AM, Alston JT, Yang Z, Arner EC, Griggs DW (2007) Aggrecan degradation in human articular cartilage explants is mediated by both ADAMTS-4 and ADAMTS-5. Arthritis Rheum 56:575–585
Innes JF, Little CB, Hughes CE, Caterson B (2005) Products resulting from cleavage of the interglobular domain of aggrecan in samples of synovial fluid collected from dogs with early- and late-stage osteoarthritis. Am J Vet Res 66:1679–1685
Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, Christy W, Cooke TD, Greenwald R, Hochberg M (1986) Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 29:1039–1049
Recht MP, Kramer J, Marcelis S, Pathria MN, Trudell D, Haghighi P, Sartoris DJ, Resnick D (1993) Abnormalities of articular cartilage in the knee: analysis of available MR techniques. Radiology 187:473–478
Outerbridge RE (1964) Further studies on the etiology of Chondromalacia patellae. J Bone Joint Surg Br 46:179–190
Eckstein F, Burstein D, Link TM (2006) Quantitative MRI of cartilage and bone: degenerative changes in osteoarthritis. NMR Biomed 19:822–854
Eckstein F, Charles HC, Buck RJ, Kraus VB, Remmers AE, Hudelmaier M, Wirth W, Evelhoch JL (2005) Accuracy and precision of quantitative assessment of cartilage morphology by magnetic resonance imaging at 3.0 T. Arthritis Rheum 52:3132–3136
Hollander AP, Pidoux I, Reiner A, Rorabeck C, Bourne R, Poole AR (1995) Damage to type II collagen in aging and osteoarthritis starts at the articular surface, originates around chondrocytes, and extends into the cartilage with progressive degeneration. J Clin Invest 96:2859–2869
Mankin HJ, Lippiello L (1970) Biochemical and metabolic abnormalities in articular cartilage from osteo-arthritic human hips. J Bone Joint Surg Am 52:424–434
Little CB, Flannery CR, Hughes CE, Mort JS, Roughley PJ, Dent C, Caterson B (1999) Aggrecanase versus matrix metalloproteinases in the catabolism of the interglobular domain of aggrecan in vitro. Biochem J 344(Pt 1):61–68
Flannery CR, Lark MW, Sandy JD (1992) Identification of a stromelysin cleavage site within the interglobular domain of human aggrecan. Evidence for proteolysis at this site in vivo in human articular cartilage. J Biol Chem 267:1008–1014
Lohmander LS, Neame PJ, Sandy JD (1993) The structure of aggrecan fragments in human synovial fluid. Evidence that aggrecanase mediates cartilage degradation in inflammatory joint disease, joint injury, and osteoarthritis. Arthritis Rheum 36:1214–1222
Sandy JD, Flannery CR, Neame PJ, Lohmander LS (1992) The structure of aggrecan fragments in human synovial fluid. Evidence for the involvement in osteoarthritis of a novel proteinase which cleaves the Glu 373-Ala 374 bond of the interglobular domain. J Clin Invest 89:1512–1516
Tortorella M, Pratta M, Liu RQ, Abbaszade I, Ross H, Burn T, Arner E (2000) The thrombospondin motif of aggrecanase-1 (ADAMTS-4) is critical for aggrecan substrate recognition and cleavage. J Biol Chem 275:25791–25797
Kevorkian L, Young DA, Darrah C, Donell ST, Shepstone L, Porter S, Brockbank SM, Edwards DR, Parker AE, Clark IM (2004) Expression profiling of metalloproteinases and their inhibitors in cartilage. Arthritis Rheum 50:131–141
Plaas A, Osborn B, Yoshihara Y, Bai Y, Bloom T, Nelson F, Mikecz K, Sandy JD (2007) Aggrecanolysis in human osteoarthritis: confocal localization and biochemical characterization of ADAMTS5-hyaluronan complexes in articular cartilages. Osteoarthritis Cartilage 15:719–734
Bau B, Gebhard PM, Haag J, Knorr T, Bartnik E, Aigner T (2002) Relative messenger RNA expression profiling of collagenases and aggrecanases in human articular chondrocytes in vivo and in vitro. Arthritis Rheum 46:2648–2657
Glasson SS, Askew R, Sheppard B, Carito B, Blanchet T, Ma HL, Flannery CR, Peluso D, Kanki K, Yang Z, Majumdar MK, Morris EA (2005) Deletion of active ADAMTS5 prevents cartilage degradation in a murine model of osteoarthritis. Nature 434:644–648
Stanton H, Rogerson FM, East CJ, Golub SB, Lawlor KE, Meeker CT, Little CB, Last K, Farmer PJ, Campbell IK, Fourie AM, Fosang AJ (2005) ADAMTS5 is the major aggrecanase in mouse cartilage in vivo and in vitro. Nature 434:648–652
Rogerson FM, Stanton H, East CJ, Golub SB, Tutolo L, Farmer PJ, Fosang AJ (2008) Evidence of a novel aggrecan-degrading activity in cartilage: studies of mice deficient in both ADAMTS-4 and ADAMTS-5. Arthritis Rheum 58:1664–1673
Tortorella MD, Malfait AM, Deccico C, Arner E (2001) The role of ADAM-TS4 (aggrecanase-1) and ADAM-TS5 (aggrecanase-2) in a model of cartilage degradation. Osteoarthritis Cartilage 9:539–552
Powell AJ, Little CB, Hughes CE (2007) Low molecular weight isoforms of the aggrecanases are responsible for the cytokine-induced proteolysis of aggrecan in a porcine chondrocyte culture system. Arthritis Rheum 56:3010–3019
Kamm JL, Nixon AJ, Witte TH (2010) Cytokine and catabolic enzyme expression in synovium, synovial fluid and articular cartilage of naturally osteoarthritic equine carpi. Equine Vet J 42:693–699
Gendron C, Kashiwagi M, Lim NH, Enghild JJ, Thogersen IB, Hughes C, Caterson B, Nagase H (2007) Proteolytic activities of human ADAMTS-5: comparative studies with ADAMTS-4. J Biol Chem 282:18294–18306
Acknowledgments
This work was supported by the Provincial Natural Science Foundation of Shandong (Y2007C132), National Natural Science Foundation of China (NTFC) (30972720), National Basic Research Program of China (2010CB529105), and Shandong Taishan Scholarship.
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhang, E., Yan, X., Zhang, M. et al. Aggrecanases in the human synovial fluid at different stages of osteoarthritis. Clin Rheumatol 32, 797–803 (2013). https://doi.org/10.1007/s10067-013-2171-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-013-2171-0