
Abstract
Rice body formation is an uncommon inflammatory disorder associated with systemic disorders such as rheumatoid arthritis and tuberculosis infection. The pathophysiology of rice bodies is poorly understood. We describe a case of rice body formation in a 51-year-old male who presented with pain and swelling of the left wrist. The patient had no previous history of rheumatic disease, joint trauma, or infectious disease. He underwent a radical tenosynovectomy and had immediate improvement of symptoms. Despite extensive evaluation, the etiology of the rice bodies could not be identified. An increasing number of case reports have described rice body formation without a known cause suggesting an alternative, unidentified method of pathogenesis. We describe a unique case of rice body formation and a review of the literature with emphasis on theories of pathogenesis, diagnostic methods, and treatment.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Rice bodies were first described in 1895 as intra-articular proteinaceous masses associated with tuberculosis [1]. Macroscopically resembling polished rice, rice bodies are now more commonly encountered as sequelae of multiple rheumatic disorders including rheumatoid arthritis [2], juvenile arthritis [3, 4], seronegative inflammatory arthritis [2], osteoarthritis [5], and chronic bursitis [6]. We describe a rare presentation of rice bodies in a patient with no clinical evidence of infection or joint disease. Current theories of pathogenesis are discussed.
Case report
A 51-year-old left-handed male presented with a 2-year history of an enlarging mass proximal to his left wrist. The mass was associated with numbness and pain in his index finger, hand, and forearm. The patient had no prior history of joint trauma or rheumatic disease. The patient took no medications and his past medical history was unremarkable. An MRI scan revealed a 14.1-cm long × 3.8-cm AP × 7-cm wide soft tissue lesion which was described radiologically as a large non-aggressive soft tissue mass centered around the flexor digitorum tendons (Fig. 1). The findings were deemed most consistent with a synovial-based mass such as a giant cell tumor or synovial sarcoma. An open incisional biopsy revealed multiple small ovoid nodules of fibrinoid proteinaceous material enveloped by neutrophilic debris consistent with rice bodies (Fig. 2). The patient's initial postoperative period was uneventful with primary healing of the wounds. Symptoms of median neuropathy improved; however, the patient continued to have mild numbness of his index finger several months after surgery. The final pathological findings demonstrated hyperplastic synovium containing rice bodies with a prominent granulomatous response. Histochemical staining for acid fast bacilli was negative. Follow-up 1 year after surgery reveals no evidence of recurrence.

a Sagittal T2-weighted MR image of left distal forearm revealing mildly enlarged tendon sheaths and many small masses with low signal intensity. b Axial T2-weighted MR image of left distal forearm revealing small masses of low signal intensity surrounding the flexor digitorum tendons

a Photomicrograph of hyperplastic synovium at ×10 magnification predominantly composed of fibrous tissue infiltrated by chronic inflammatory cells consisting of lymphocytes, histiocytes, and scattered mast cells. b Photomicrograph of rice body at ×4 magnification. The nodules of fibrinoid and proteinaceous material are enveloped by neutrophilic debris. c Photomicrograph of rice body at ×20 magnification. The dense proteinaceous and fibrinoid material (rice body) sparsely infiltrated by lymphocytes
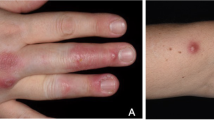
Three months after radical synovectomy, the patient underwent evaluation for autoimmune and rheumatologic disease. Apart from minor swelling and erythema noted over the left hand and index finger, the patient's musculoskeletal exam was unremarkable. Anti-dsDNA (<1 IU/mL), anti-RNP (<0.2 AI), anti-Smith (<0.2 AI), anti-SS-A (<0.2 AI), and anti-SS-B (<0.2 AI) antibodies were within normal limits. Antinuclear antibodies and HLA B27 association were negative. Evaluation for rheumatoid arthritis revealed no elevation in rheumatoid factor or CCP IgG/IgA antibodies. The only laboratory abnormalities identified were elevated LDL (148 mg/dL) and total (236 mg/dL) cholesterol. It was concluded that the patient did not meet criteria for rheumatologic disease. Patient continued to be asymptomatic 1 year after surgery.
Discussion
Rice bodies are historically considered a nonspecific response to joint inflammation. Incidence is most common in rheumatoid arthritis, where rice bodies were found in 72 % of adult rheumatoid joints upon synovial lavage [2]. Rice body formation appears unrelated to arthritis duration, severity, or associated radiographic changes [2]. Rice bodies have been isolated from all major joints and can present as a painless mass [7] or with painful neuropathy [8] depending on location.
The origin of rice body formation is poorly understood. Composition studies have demonstrated that rice bodies have an acidophilic amorphous core surrounded by fibrin and collagen [9]. The presence of microvasculature within some rice bodies and a protein composition similar to synovial membrane lead Berg et al. to propose that they were derived from microinfarcted synovium [9, 10]. Synovium shed due to articular inflammation would become encased by fibrin within the synovial cavity. This theory was supported by the isolation of rice bodies containing viable cells which most closely resembled type B synovial lining cells [11]. Furthermore, apatite and calcium pyrophosphate dihydrate crystals have also been identified within rice bodies [5, 12]. These crystals are seen in the synovial fluid of joints damaged by osteoarthritis [13].
Although primarily isolated from articular joints, rice bodies have been identified at extra-articular sites. Rice bodies have been isolated from pleural fluid [14], along tendon sheaths [15–17] and within bursae [6] suggesting a non-synovial origin. Muirhead et al. identified rice bodies at a site of extra-articular injury with foreign body inflammation [18]. It was proposed that rice bodies were formed by fibroblasts surrounding a fibrin clot where activation of the fibroblasts would produce the collagenous component. Immunohistochemical analysis by Sugano et al. revealed rice bodies had a cellular component which consisted primarily of T cells and a minor number of neutrophilic and histiocytic cells [19]. These findings supported the theory that rice bodies were the result of chronic inflammation.
Rice bodies are present in less than 50 % of cases of tuberculous tenosynovitis [20]. Tuberculous tenosynovitis with rice bodies presents with granulomatous inflammation with Langhan giant cells and localized caseous necrosis [16, 20]. Ziehl–Neelsen positivity is usually seen as are symptoms of other tuberculous lesions [20]. In our case, the patient had no history of tuberculosis symptoms or exposure. Furthermore, the lesion was negative for acid fast bacilli and did not present with characteristic tuberculous histology.
MRI is considered the imaging modality of choice for rice bodies which appear iso- or hypointense to skeletal muscle on T1- and T2-weighted images [21, 22]. Although sometimes difficult to differentiate from chronic synovial proliferation, pigmented villonodular synovitis (PVNS), and synovial osteochondromatosis, a lack of susceptibility artifact on gradient echo sequences can allow discrimination from synovial chondromatosis and PVNS [21]. The unmineralized cartilage-containing masses of synovial chondromatosis commonly appear isointense or mildly hyperintense on T1-weighted and hyperintense on T2-weighted sequences relative to skeletal muscle. PVNS often also shows foci of signal voids reflecting hemosiderosis which is not seen in rice bodies [22].
The clinical management of rice body formation in the forearm focuses on surgical excision. Surgical removal is recommended for all patients with symptoms of nerve compression or those suspected of mycobacterial infection [17]. Rheumatoid patients with asymptomatic rice bodies in the forearm may require prophylactic tenosynovectomy to prevent tendon rupture [16]. Complete excision has been suggested for cases suspected of rice body formation due to inflamed tenosynovium to prevent recurrence. Recurrence post-surgery has been reported in the literature [8].
The formation of rice bodies at sites of traumatic injury, infection, and rheumatic disease suggests an important role for inflammation in rice body pathogenesis. We described a patient with rice body formation who presented with synovial inflammation from an unknown cause. Our findings are similar to those of previous reports (Table 1) and suggest an alternative route for rice body formation to that described in the literature. It is of note that the patient presented here had a 30-year history of chemical exposure due to his employment at an oil refinery. A recent study described elevated levels of circulating advanced oxidation protein products, markers of generalized oxidative stress and inflammation, in oil refinery workers [23]. Previous reports of non-tuberculous rice body formation have not addressed the potential significance of patient occupational and/or environmental exposure. It is possible that certain chemical compounds may predispose individuals to rice bodies.
In conclusion, we describe a case of rice body formation in a healthy male of unknown etiology. Further studies are necessary to better understand the pathogenesis of rice bodies and their significance in articular tissue response to inflammation.
References
Riese H (1895) Di Reiskorpchen in tuberculos erkranken synovalsacken. Detsch Z Chir 42:1–99
Popert AJ, Scott DL, Wainwright AC, Walton KW, Williamson N, Chapman JH (1982) Frequency of occurrence, mode of development, and significance of rice bodies in rheumatoid joints. Ann Rheum Dis 41:109–117
Wynne-Roberts CR, Cassidy JT (1979) Juvenile rheumatoid arthritis with rice bodies: light and electron microscopic studies. Ann Rheum Dis 38:8–13
DiVito A, Kan JH (2008) Juvenile idiopathic arthritis with rice bodies. Pediatr Radiol 38:1263
Bucki B, Lansaman J, Janson X, Billon-Galland MA, Marty C, Ruel M, Kuntz D, Dryll A, Bardin T (1994) Osteoarthritis with rice bodies in calcium microcrystals. 4 cases with ultrastructural study. Rev Rhum Ed Fr 61(6):415–420
Steinfeld R, Rock MG, Younge DA, Cofield RH (1994) Massive subacromial bursitis with rice bodies: report of three cases, one of which was bilateral. Clin Orthop Relat Res 301:185–190
Uludeg S, Seyahi A, Ege Y, Tetik O (2010) Rice body mass formation mimicking a neoplastic disease around the trochanteric bursae of the hip. Acta Orthop Traumatol Turc 44(5):492–495
Iyengar K, Manickavasagar T, Nadkarni J, Mansour P, Loh W (2011) Bilateral recurrent wrist flexor tenosynovitis and rice body formation in a patient with sero-negative rheumatoid arthritis: a case report and review of literature. Int J Surg Case Rep 2(7):208–211
Berg E, Wainwright R, Barton B, Puchtler H, McDonald T (1977) On the nature of rheumatoid rice bodies: an immunologic, histochemical and electron microscope study. Arthritis Rheum 20(7):1343–1349
Cheung HS, Ryan LM, Kozin F, McCarty DJ (1980) Synovial origins of rice bodies in joint fluid. Arthritis Rheum 23(1):72–76
Wynne-Roberts CR, Cassidy JT (1979) Juvenile rheumatoid arthritis with rice bodies: light and electron microscopic studies. Ann Rheum Dis 36:8–13
Li-Yu J, Clayburne GM, Sieck MS, Walker SE, Athreya BH, DeHoratius RJ, Schumacher HR Jr (2002) Calcium apatite crystals in synovial fluid rice bodies. Ann Rheum Dis 61:387–390
Gibilisco PA, Scumacher R, Hollander JL, Soper KA (1985) Synovial fluid crystals in osteoarthritis. Arthritis Rheum 28(5):511–515
Kassimos D, George E, Kirwan JR (1994) Rice bodies in the pleural aspirate of a patient with rheumatoid arthritis. Ann Rheum Dis 53(6):427–428
Luiz CP, Ramananathan EB, Buhi L, Muirhead D (1994) A case of date palm thorn-induced extra articular synovitis with rice grain bodies. Dr J Rhematol 33:1190–1191
Suso S, Piedro L, Ramon R (1988) Tuberculous synovitis with “rice bodies” presenting as carpal tunnel syndrome. J Hand Surg 13:574–576
Cuomo A, Pirpiris M, Otsuka NY (2006) Case report: biceps tenosynovial rice bodies. J Pediatr Orthop B 15:423–425
Muirhead DE, Johnson EH, Luis C (1998) A light and ultrastructural study of rice bodies recovered from a case of date thorn-induced extra-articular synovitis. Ultrastruct Pathol 22:341–347
Sugano I, Nagao T, Tajima Y, Ishida Y, Nagao K, Ohno T, Ooishi S (2000) Variation among giant rice bodies: report of four cases and their clincopathological features. Skeletal Radiol 29:525–529
Pimm LH, Waugh W (1957) Tuberculous tenosynovitis. J Bone Joint Surg 39B:91–101
Spence LD, Adams J, Gibbons D, Mason MD, Eustace S (1998) Rice body formation in bicipito-radial bursitis: ultrasound, CT and MRI findings. Skeletal Radiol 27:30–32
Griffith JF, Peh WC, Evans NS, Smallman LA, Wong RW, Thomas AM (1996) Multiple rice body formation in chronic subacromial/subdeltoid bursitis: MR appearances. Clin Radiol 51:511–514
Spatari G, Saitta S, Cimino F, Sapienza D, Quattrocchi P, Carrieri M, Barbaro M, Saija A, Gangemi S (2012) Increased serum levels of advanced oxidation protein products and glycation end products in subjects exposed to low-dose benzene. Int J Hyg Environ Health 215:389–392
Nagasawa H, Okada K, Senma S, Chida S, Shimada Y (2009) Tenosynovitis with rice body formation in a non-tuberculosis patient: a case report. Ups J Med Sci 114:184–188
Hauser B, Hutchinson D (2011) Clinical image: rice body arthritis. Arthritis Rheum 63(4):1158
Ergun T, Lakadamyali H, Aydin O (2008) Multiple rice body formation accompanying the chronic nonspecific tenosynovitis of flexor tendons of the wrist. Radiat Med 26:545–548
Tyllianakis M, Kasimatis G, Athanaselis S (2006) Rice-body formation and tenosynovitis of the wrist: a case report. J Ortho Surg 14(2):208–211
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Forse, C.L., Mucha, B.L., Santos, M.L.Z. et al. Rice body formation without rheumatic disease or tuberculosis infection: a case report and literature review. Clin Rheumatol 31, 1753–1756 (2012). https://doi.org/10.1007/s10067-012-2063-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-012-2063-8