
Abstract
The subacromial syndrome is the most common source of shoulder pain. The mainstays of conservative treatment are non-steroidal anti-inflammatory drugs and exercise therapy. Recently, low-level laser therapy (LLLT) has been popularized in the treatment of various musculoskeletal disorders. The aim of this study is to evaluate the additive effects of LLLT with exercise in comparison with exercise therapy alone in treatment of the subacromial syndrome. We conducted a randomised clinical study of 80 patients who presented to clinic with subacromial syndrome (rotator cuff and biceps tendinitis). Patients were randomly allocated into two groups. In group I (n = 40), patients were given laser treatment (pulsed infrared laser) and exercise therapy for ten sessions during a period of 2 weeks. In group II (n = 40), placebo laser and the same exercise therapy were given for the same period. Patients were evaluated for the pain with visual analogue scale (VAS) and shoulder range of motion (ROM) in an active and passive movement of flexion, abduction and external rotation before and after treatment. In both groups, significant post-treatment improvements were achieved in all parameters (P = 0.00). In comparison between the two groups, a significant improvement was noted in all movements in group I (P = 0.00). Also, there was a substantial difference between the groups in VAS scores (P = 0.00) which showed significant pain reduction in group I. This study indicates that LLLT combined exercise is more effective than exercise therapy alone in relieving pain and in improving the shoulder ROM in patients with subacromial syndrome.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Shoulder disorders are a common cause of persistent musculoskeletal morbidity, especially increasing in the middle to older age groups [1, 2]. The prevalence of shoulder disorders has been reported between 7% and 25% of the general population and 5% percent of general practice consultations related to shoulder complaints [3, 4]. Pain is the primary symptom in most patients with shoulder disorders affecting the soft tissue. In many patients, painful restriction of the shoulder range of motion (ROM) limits the ability to perform daily activities [5, 6]. In addition, shoulder pain is often associated with impaired ability to sleep, so affecting mood and concentration. People with shoulder pain have been shown to score substantially less than normal values on the SF-36 (a standardized measure of general health) for physical function, social function, physical role function, emotional role function and pain [7, 8].
A painful shoulder may be caused by various diseases and conditions, including neurological or vascular disorders, neoplasms, referred pain from internal organs, and disorders of the cervical spine (extrinsic causes), but the most causes are articular or periarticular diseases like subacromial syndrome that includes rotator cuff and biceps tendinitis, calcifying tendinitis, subacromial bursitis and rotator cuff rupture that are manifested by pain, limited movement and strength and the loss of shoulder function, which becomes more common with increasing of age and practice of certain occupations and sporting [9, 10]. There are many accepted standard forms of conservative treatment for subacromial syndrome, including non-steroidal anti-inflammatory drugs, corticosteroid injections and physiotherapy interventions, yet little conclusive evidence supports or refutes their efficacy. Physiotherapy encompasses a broad range of interventions. These interventions are often the first line of management for shoulder disorders [11]. Physiotherapy interventions include mobilization, manipulation, acupuncture, exercise and electrotherapy. Electrotherapeutic modalities include ultrasound, bipolar interferential current, transcutaneous electrical nerve stimulation and pulsed electromagnetic field therapy [12–15]. One of the most fascinating developments within the field of electrotherapy in recent years has been the introduction of low-level lasers that were used by some physiotherapists as a therapeutic intervention for musculoskeletal disorders such as back pain, neck pain and shoulder pain [16, 17]. When low-level laser radiation acts as therapeutic doses can produce change in physiochemical, biophysical, biochemical and physiological processes, which naturally occur in cells [18]. Low-level laser therapy (LLLT) accelerates connective tissue repair with effects on fibroblast function, improve local microcirculation and oxygen supply to hypoxic cells and removes the collected waste products [19, 20]; LLLT also has anti-inflammatory effects with reduction in prostaglandin synthesis [21].
There were different results in the efficacy of LLLT in shoulder disorders. In a study by Bingöl et al., LLLT had no significant improvement in pain, active shoulder ROM compared to exercise therapy in patients with shoulder pain [22]. The same results have been seen in patients with subacromial impingement syndrome, in comparison between the effects of LLLT plus exercise and exercise alone [23]. But there have been a few studies which suggest LLLT alone improves pain and increases recovery rates in comparison with placebo laser in patients with rotator cuff tendinitis [24, 25]. So, there are controversial studies about the efficacy of LLLT alone and its adjutant effects on shoulder disorders. In this regard, the aim of our study is to evaluate the additive effects of LLLT with exercise in treatment of the shoulder pain in patients with subacromial syndrome (rotator cuff and biceps tendinitis).
Materials and methods
Study participants
A total of 80 patients with diagnosis of subacromial syndrome presented to Shahid Sadoughi clinic (Yazd, Iran) with a priori inclusion/exclusion criteria that were defined based on methodological criteria and a current understanding of the principles of application of LLLT.
Patients with subacromial syndrome (rotator cuff and biceps tendinitis) who were 18 years old and above were eligible. The diagnosis of subacromial syndrome was based on clinical presentation and physical examination. The clinical tests for rotator cuff tendinitis were Impingement test (Neer sign), Hawkins–Kennedy test and Supraspinatus (Jobe) muscle test. For biceps tendinitis, we used Speed test [26].
Participants who had a history of significant trauma or systemic inflammatory conditions such as rheumatoid arthritis or polymyalgia rheumatica, neurological or structural abnormality affecting the shoulder, post-operative and peri-operative shoulder pain, pregnancy or breastfeeding, anticoagulation therapy, diabetes mellitus, cardiac-type chest pain, cigarette smoking, shoulder infection, shoulder trauma and participants with laser therapy contraindication were excluded.
Study design
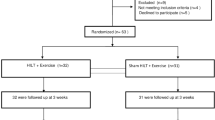
This study is a randomised, double blind, controlled trial that was reviewed and approved by the research ethics committees in Shahid Sadoughi University of Medical Sciences. All subjects gave written informed consent to participate in the study. After measurement of pain severity and shoulder ROM, patients were randomised in two groups by using sealed envelopes method. In group I (n = 40), patients received LLLT and exercise therapy for ten sessions during a period of 2 weeks and in group II (n = 40), placebo laser and the same exercise therapy were given for the same period. One physiotherapist administered treatment for all patients (Fig. 1).

Study design
Interventions
All participants were managed and treated by exercise therapy programs. Shoulder exercise programs included strengthening, stretching and mobilization exercises in clinic and at home. These exercises in clinic were pulley and shoulder wheel exercises in all the sessions; thereafter, the exercises continued at home by teaching the participants. Home exercises were pendular shoulder exercise for two first sessions. From the third session, isometric shoulder exercises and active assisted exercise were done for shoulder muscles improvement (deltoid, biceps, triceps and scapula fixator muscles).
In each treatment session, after the exercise therapy programs, patients in group I received infrared laser radiation (wavelength, 890 nm in pulsed mode). In each treatment session, three points on the shoulder, including anterior (coracoid), posterior (glenohumeral joint) and lateral (rotator cuff tendon) were irradiated for 2 min (a total of 6 min) by using a laser device (Mustang-024, Russia). Also, the biceps tendon was irradiated for patients with biceps tendinitis. The energy density was 2–4 J/cm2 in each three points.
Patients in the second group were treated with placebo laser therapy. The same device which seemed to be working was used but no laser beams were transferred to the treated area. During the study period, the patients were not allowed to take analgesic and/or NSAID medication.
Outcome measures
Outcomes were pain and shoulder ROM. Pain functional assessments were based on 10-cm visual analogue scale (VAS). The visual analogue scale has been shown to be a reliable and valid measure of pain and consists of a standard 10-cm line with verbal anchors indicating “no pain” at 0 cm and “severe pain” at 10 cm [27]. Participants were asked to estimate their pain severity by placing a mark on the line.
Shoulder ROM was measured by a blinded physician unaware of the treatment. The maximum active and passive flexion, abduction and external rotation were measured with a goniometer. Goniometry is a reliable method for shoulder range of motion measurement [28]. The goniometer fulcrum was placed on the greater tuberosity for flexion movement, while for abduction and external rotation movements, it was placed over the anterior aspect of the acromion process and on the tip of the elbow, respectively. After motions, the formed angle was measured. All motions were measured in a supine position.
Statistical analysis
All statistical analysis was conducted on intention to treat basis by using the SPSS 15.0 software. The chosen type I error was set at α = 0.05 and the type II error at β = 0.20. All data were in normal distribution by using Shapiro–Wilk test and results were expressed as mean ± SD. Student’s t tests were considered for the comparison of the result within and between the groups.
Result
Among the 103 patients who were admitted with shoulder pain, 23 patients were excluded and 80 patients with subacromial syndrome (50 women, 30 men) remained. The mean age of study population was 51.7 years. All of the 80 participants completed the treatment. There was no statistically significant difference between the two groups in demographic data such as age, gender, occupational activity and educational level (Table 1).
After treatment, there were statistically significant improvements in pain severity and shoulder ROM in both groups (P = 0.00) (Table 2). In comparison between the two groups, there was a notable difference between groups in VAS scores (P = 0.00) which showed significant pain reduction in group I. Also, there was a significant post-treatment improvement for all active and passive movements in group I (P = 0.00) (Table 3). None of the participants reported any adverse reaction or side effects.
Discussion
Infrared laser radiation was established to be absorbed by oxygen, water, enzyme and biological structures—mainly by cell membranes. When absorbed, infrared radiation is converted into heat, which increases the vibrational energy of biomolecules, and that this phenomenon is the main effect of infrared low-level laser radiation. Laser radiation at the wavelengths of 630 to 1,300 nm has the most efficacy on biological tissues. The laser radiation of this spectral range improves microcirculation, stimulates metabolism, facilitates cell recovery and activates the immune system. Moreover, laser radiation increases the pain threshold of nerve endings that results in pain reduction [18]. Other effects include analgesia, myorelaxation, tissue healing, ligament repair, fibroblast proliferation and anti-inflammatory effects [19–21, 29–31].
This study showed that LLLT plus exercise therapy was more effective than exercise therapy alone in the improvement of pain and active and passive ROM in patients with subacromial syndrome. Few studies have been yet conducted to compare the effectiveness of LLLT in combination with exercise in subacromial syndrome. The results of this trial indicated that pain severity reduced significantly in patients that were treated with LLLT and exercise therapy in comparison to exercise alone, according to VAS score. Also, there was a significant improvement in active and passive shoulder movements in flexion, abduction and external rotation in LLLT and exercise treatment.
In comparison with other studies, Green et al. (Cochrane review study) in a review of varying physiotherapy interventions for shoulder disorders indicated that exercise therapy was effective in recovery of rotator cuff disease, but noted that laser therapy is not effective for rotator cuff tendinitis [32]. Vecchio et al. in a randomised clinical trial of patients with rotator cuff tendinitis found no significant difference between continuous irradiation laser (Ga As Al diode laser, 830 nm wavelength, 5,000 Hz frequency) and sham laser for pain reduction and shoulder ROM improvement, twice weekly for 8 weeks [33]; but, England et al. demonstrated the effectiveness of active infrared laser therapy (Ga As diode laser, 904 nm wavelength, 4,000 Hz frequency, three times weekly for 2 weeks) in tendonitis of the shoulder (supraspinatus or bicipital tendonitis) in active extension, flexion and abduction of the shoulder, pain stiffness movement and shoulder function [13]. Moreover, Saunders showed that LLLT (Ga As diode laser, 820 nm wavelength, 5,000 Hz frequency, three times weekly for 3 weeks) is a useful treatment for tendinitis (supraspinatus tendinitis) in reducing pain, secondary weakness and tenderness [24]. In fact, they showed that LLLT is a good therapeutic method for shoulder tendonitis. In another study, Stergioulas indicated that LLLT (Ga-Al-As laser, 810 nm wavelength, 50 Hz, 12 sessions in 8 weeks) was effective in reduction of pain and shoulder disability in patients with frozen shoulder [34]. In rehabilitation of subacromial impingement syndrome, Yeldan et al. indicated that there is no noticeable difference between LLLT and placebo LLLT in combination to superficial cold and progressive exercise in pain severity, muscle strength and shoulder function. They used Ga As diode laser with 904 nm wavelength and 2,000 Hz frequency at each session for 15 days in 3 weeks [35]. The same results have been seen in study of Bal et al. in comparison of LLLT plus home exercise therapy and home exercise therapy alone [23]. Also, Michener et al. in a systematic review study for rehabilitation of subacromial impingement syndrome pointed out that laser therapy only was effective when used in isolation, not in combination with therapeutic exercise [36]. In the mentioned studies, there are different results about alone or adjutant effects of LLLT in shoulder pain. In our study, the number of patients was more than all studies and we applied defined exercise programs with infrared laser therapy at 890 nm wavelengths but in variable pulse repetition rate from 80 Hz (suitable for chronic inflamatory degenerative dystrophic processes) to 1,500 Hz (suitable for acute inflamatory processes and pronouncd pain syndrome) during the ten sessions in a period of 2 weeks [18]. Our findings are controversial with the studies above about combination effects of LLLT with exercise therapy which the possible explanation for it may be different laser setting and therapeutic protocol. Overall, it must be noted that various factors play important roles on the effectiveness of laser therapy, such as laser wavelength, dosage, intensity, energy density and frequency, also different lasers may have different effectiveness in different shoulder disorders.
This clinical trial has some limitations. First, the outcome measures were limited to VAS and measurement of ROM and we did not evaluate other outcome measures such as shoulder disability or quality of life in patients. So, more studies should be conducted to assess these outcome measures by Shoulder Disability Questionnaire or Disabilities of the Arm, Shoulder and Hand Questionnaire. The other limitation of our study was that we had no long-term follow-up after treatment.
Conclusion
Our study indicates that LLLT combined with exercise therapy is more effective than exercise therapy alone in relieving pain and in improving the shoulder joint ROM in patients with subacromial syndrome (rotator cuff and biceps tendinitis), but further studies with larger samples, longer term findings and possible comparisons with other conservative interventions are needed to establish the effectiveness of this protocol.
References
Roquelaure Y, Ha C, Leclerc A, Touranchet A, Sauteron M, Melchior M et al (2006) Epidemiologic surveillance of upper-extremity musculoskeletal disorders in the working population. Arthritis Rheum 55:765–778
Badley EM, Tennant A (1992) Changing profile of joint disorders with age: findings from a postal survey of the population of Calderdale, West Yorkshire, United Kingdom. Ann Rheum Dis 51:366–371
Van der Heijden GJMG, van der Windt DAWM, de Winter AF (1997) Physiotherapy for patients with soft tissue shoulder disorders: a systematic review of randomised clinical trials. Br Med J 315:25–30
Peters D, Davies P, Pietroni P (1994) Musculoskeletal clinic in general practice: study of 1 year referrals. Br J Gen Pract 44:25–29
Croft P (1993) Soft-tissue rheumatism. In: Silman AJ, Hochberg MC (eds) Epidemiology of the rheumatic diseases. Oxford University Press, Oxford, pp 375–421
Van der Windt DAWM, Koes BW, De Jong BA, Bouter LM (1995) Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 54:959–964
Beaton D, Richards L (1996) Measuring function of the shoulder. J Bone Joint Surg 78:882–890
Gartsman GM, Brinker MR, Khan M, Karahan M (1998) Self assessment of general health status in patients with five common shoulder conditions. J Shoulder Elbow Surg 7:228–237
Green S, Buchbinder R, Hetrick S (2005) Acupuncture for shoulder pain. Cochrane Database Syst Rev CD005319
Cunningham LS, Kelsey JL (1984) Epidemiology of musculoskeletal impairments and associated disability. Am J Public Health 74:574–579
Lee M, Haq A, Wright V, Longton E (1973) Periarthritis of the shoulder: a controlled trial of physiotherapy. Physiotherapy 59:312–315
Herrera-Lasso I, Moborak L, Fernandez-Dominguez L, Cardiel M, Alarcon-Segovia D (1993) Comparative effectiveness of packages of treatment including ultrasound or transcutaneous electrical nerve stimulation in painful shoulder syndrome. Physiotherapy 79:251–253
England S, Farrell AJ, Coppock JS, Struthers G, Bacon PA (1989) Low power laser therapy of shoulder tendonitis. Scand J Rheumatol 18:427–431
Downing D, Weinstein A (1986) Ultrasound therapy of subacromial bursitis. Phys Ther 66:194–199
Binder A, Parr G, Hazleman B (1984) Pulsed electromagnetic field therapy of persistent rotator cuff tendonitis. Lancet 1:695–698
Beckerman H, de Bie RA, Bouter LM, de Cuyper HJ, Oostendorp RAB (1992) The efficacy of laser therapy for musculoskeletal and skin disorders: a criteria-based meta-analysis of randomized clinical trials. Phys Ther 72:483–491
Bjordal JM, Couppé C, Chow RT, Tunér J, Ljunggren EA (2003) A systematic review of low level laser therapy with location-specific doses for pain from chronic joint disorders. Aust J Physiother 49:107–116
Buylin VA, Mskovin SV (2001) Low-intensity laser therapy of various diseases. Technika Firm, Moscow
Kreisler M, Christoffers AB, Al-Haj H, Willershausen B, d’Hoedt B (2002) Low level 809 nm diode laser induced in vitro stimulation of the proliferation of human gingival fibroblasts. Lasers Surg Med 30:365–369
Simunovic Z (1996) Low level laser therapy with trigger points technique: a clinical study on 243 patients. J Clin Laser Med Surg 14:163–167
Sakurai Y, Yamaguchi M, Abiko Y (2000) Inhibitory effect of low-level laser irradiation on LPS-stimulated prostaglandin E2 production and cyclooxygenase-2 in human gingival fibroblasts. Eur J Oral Sci 108:29–34
Bingöl U, Altan L, Yurtkuran M (2005) Low-power laser treatment for shoulder pain. Photomed Laser Surg 23:459–464
Bal A, Eksioglu E, Gurcay E, Gulec B, Karaahmet O, Cakci A (2009) Low-level laser therapy in subacromial impingement syndrome. Photomed Laser Surg 27:31–36
Saunders L (1995) The efficacy of low level laser therapy in supraspinatus tendinitis. Clin Rehabil 9:126–134
Gudmundssen J, Vikne J (1987) Laser treatment for epicondylitis humeri and rotator cuff syndrome. Nord Tidskr Idrettsmed 2:6–15
Miller RH, Dlabach JA (2008) Shoulder and elbow injuries. In: Canale ST, Beatty JH (eds) Campbell’s operative orthopaedics, 11th edn. Mosby Elsevier, Philadelphia, pp 2603–2607
Wewers ME, Lowe NK (1990) A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health 13:227–236
Hayes K, Walton JR, Szomor ZR, Murrell GA (2001) Reliability of five methods for assessing shoulder range of motion. Aust J Physiother 47:289–290
Enwemeka CS, Parker JC, Dowdy DC, Harkness EE, Sanford LE, Woodruff LD (2004) The efficacy of low power lasers in tissue repair and pain control: a meta analysis study. Photomed Laser Surg 22:323–329
Sattayut S, Hugles F, Bradley P (1999) 820 nm gallium aluminium arsenide laser modulation of prostaglandin E2 production in interleukin I stimulated myoblasts. Laser Ther 11:88–95
Gam AN, Thorsen H, Lonnberg F (1993) The effect of low level laser therapy on musculoskeletal pain: a meta analysis. Pain 52:63–66
Green S, Buchbinder R, Hetrick S (2003) Physiotherapy interventions for shoulder pain. Cochrane Database Syst Rev CD004258
Vecchio P, Cave C, King V et al (1993) A double blind study of the effectiveness of low level laser treatment of rotator cuff tendinitis. Br J Rheumatol 32:740–742
Stergioulas A (2008) Low-power laser treatment in patients with frozen shoulder: preliminary results. Photomed Laser Surg 26:99–105
Yeldan I, Cetin E, Ozdincler AR (2009) The effectiveness of low-level laser therapy on shoulder function in subacromial impingement syndrome. Disabil Rehabil 31:935–940
Michener LA, Walsworth MK, Burnet EN (2004) Effectiveness of rehabilitation for patients with subacromial impingement syndrome: a systematic review. J Hand Ther 17:152–164
Acknowledgements
The authors gratefully acknowledge Mr. Esfandiar Modami (Mojibian Hospital, Yazd, Iran), Miss Ladan Ghahramani (Allameh Tabataba’i University, Tehran, Iran) and Mr. Amir Mohammad Mahabadi (Shahid Sadoughi University of Medical Sciences, Yazd, Iran) for their help during our research.
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Abrisham, S.M.J., Kermani-Alghoraishi, M., Ghahramani, R. et al. Additive effects of low-level laser therapy with exercise on subacromial syndrome: a randomised, double-blind, controlled trial. Clin Rheumatol 30, 1341–1346 (2011). https://doi.org/10.1007/s10067-011-1757-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-011-1757-7