
Abstract
Chronic infections may mimic antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAV). We investigated which markers may help in the diagnosis and the prognosis of infections associated with proteinase 3 (PR3) and myeloperoxidase (MPO)-ANCA. In this study (1993–2008)—with an average follow-up of 5.1 years—we compared 66 AAV patients with 17 PR3 and/or MPO-ANCA-positive patients with protracted bacterial (11/17) or viral (6/17) infections. Seven of 17 patients had subacute bacterial endocarditis (SBE), while six of 17 patients had various autoimmune manifestations of chronic hepatitis C virus (HCV) infection. We determined ANCA, antinuclear antibodies, anti-PR3, anti-MPO, anticardiolipin (aCL), antibeta 2 glycoprotein I (β2-GP I), cryoglobulins, C3, and C4. Patients with infections were younger than AAV patients (p < 0.01). There was no difference in frequency of renal and skin lesions. AAV patients more frequently had pulmonary and nervous system manifestations (p < 0.01). Patients with infections more frequently had dual ANCA (high PR3, low MPO), aCL, anti-β2-GP I, cryoglobulins, and hypocomplementemia (p < 0.001). Immunosuppressive therapy (IST) was used in five 17 patients who had persistently high ANCA, cryoglobulinemia, and hypocomplementemia. There was no difference in frequency of lethality and renal failure in the two study groups. In patients who are PR3- and/or MPO-ANCA positive, SBE and HCV infection should be excluded. Although similar in renal and skin manifestations in comparison to AAV, only patients with infections developed multiple serological abnormalities. In patients with infections, concomitant presence of ANCA, cryoglobulins, and hypocomplementemia was associated with severe glomerulonephritis. The serological profile should be repeated after specific antimicrobial or surgical therapy, since some cases might require IST.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The idiopathic systemic vasculitides (ISV) are characterized by chronic vessel wall inflammation of unknown origin [1]. A number of potential environmental trigger factors have been reported, including drugs and infections [2–4].
A link between infection and vasculitis has long been suspected. Associations between hepatitis B virus infection (HBV) and polyarteritis nodosa or hepatitis C virus (HCV) infection and cryoglobulinemic vasculitis are now well recognized [5, 6]. On the other hand, bacterial and viral infections can trigger the production of various autoantibodies, antinuclear antibodies (ANA), anticardiolipin antibodies (aCL), cryoglobulins, and antineutrophil cytoplasmic antibodies (ANCA), which are not always associated with vasculitis [6–8]. Generally, infection-associated autoantibodies tend to be transient, of lower titers, and more often of the IgM type.
ANCA specific for proteinase 3 (PR3) and myeloperoxidase (MPO) are serological markers of small vessel “pauci-immune” ISV [1]. Cytoplasmic PR3-ANCA has high specificity (99%) for the newly diagnosed Wegener’s granulomatosis (WG) [1]. Perinuclear MPO-ANCA is present in 70% of patients with microscopic polyangiitis (MPA) and in 38–50% of patients with Churg–Strauss syndrome (CSS) [9]. The diagnosis of ANCA-associated vasculitides (AAV) is based on the presence of clinical manifestations with characteristic histopathological findings and the presence of PR3-ANCA or MPO-ANCA [1, 9]. AAV may have a variety of presentations, including constitutional symptoms (fever, myalgia, and weight loss) with predominant involvement of the upper and lower respiratory tract, skin, kidneys, and the nervous system [1]. Pauci-immune segmental necrotizing glomerulonephritis (SNGN) with or without crescents is often present [9]. Unfortunately, some subacute or chronic infections may mimic idiopathic AAV, and their differential diagnosis may be difficult [6, 8, 9]. Moreover, PR3-ANCA and MPO-ANCA have been detected following bacterial (streptococcal, staphylococcal, and tuberculosis), viral (parvovirus B19 and HCV), protozoal (malaria), and fungal infections [9–13].
We addressed this issue by comparing clinical and serological data from 66 AAV patients with 17 patients whose ANCA positivity was associated with confirmed protracted bacterial or viral infections, diagnosed during a 15-year period. These two subsets of patients usually have similar clinical presentations, but the therapy is quite different. Up to now, no guidelines on treatment of protracted infections associated with ANCA and severe glomerulonephritis (GN) have been defined. The identification of trigger factors is essential for more effective and less toxic therapy for infections associated with ANCA. In this study, we showed that antibody profile may help to distinguish infections associated with PR3- and MPO-ANCA from primary AAV.
Patients and methods
Patients
From 1993 to 2008, 3,754 patients were tested for ANCA in the Laboratory for Allergy and Clinical Immunology in Belgrade, and 104 of 3,754 (2.7%) were PR3-ANCA and/or MPO-ANCA positive. Sixty-six of 104 patients had AAV, 21 of 104 had drug-induced ANCA, and 17 of 104 had protracted bacterial (11/17) or viral (6/17) infections. In this retrospective study, we compared clinical and serological data from 66 AAV patients with 17 patients who had protracted infections associated with ANCA. The follow-up period was from 2 weeks to 15 years, or 5.1 years on the average.
Patients with AAV
The first group consisted of 66 AAV patients (33 WG, 29 MPA, and four CSS). The diagnoses of WG, MPA, and CSS were established according to clinical, serologic, and pathohistologic criteria [1]. The diagnoses were pathohistologically confirmed in 57 of 66 patients. Kidney biopsy was performed in 42 patients (29 SNGN with cellular and fibrous crescents, four SNGN without crescents, and six SNGN with arteritis, and three had mesangial proliferation). Direct immunofluorescence (DIF) was done in 19 of 42 patients: In 15 of 19, it was negative, two of 19 showed IgM, and two of 19 had IgM and IgG.
Complete blood count, renal function tests, and complete urine tests (including 24 h proteinuria) were checked at the time of diagnosis and then serially during the follow-up period. We excluded associated viral (serology and PCR), bacterial (culture, microscopy, and serology), fungal (direct microscopy, culture, histopathology, and serology), and protozoal infections (pathogen identification in peripheral blood smears, bone marrow aspirate, stool specimens or duodenal contents, histopathology, serology, and PCR).
Therapy of patients with AAV
Patients with AAV were treated with prednisone at 0.5 mg kg−1 day−1, in combination with cyclophosphamide, either 6 i.v. pulses at 700 mg/m2, or at 2 mg kg−1 day−1 per os. This standard regimen could not induce clinical remission in 11 of 66 AAV patients, and the additional immunosuppressive therapy (IST) was necessary (plasma exchanges in four patients and intravenous immunoglobulins (IVIg) at 2 g/kg in seven patients).
ANCA-positive patients with prolonged infections
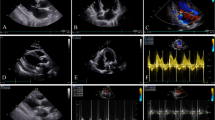
The second group consisted of 17 patients whose ANCA specific to PR3 and/or MPO were associated with confirmed protracted infection. Their immunological profile was studied because of various clinical/laboratory disorders, such as prolonged fever, weight loss, elevated acute phase reactants, purpura, pathological urine sediment, acute renal failure (ARF), etc. In all 17 PR3-ANCA- and/or MPO-ANCA-positive patients, inflammatory bowel diseases, sclerosing cholangitis, other autoimmune diseases, and malignancies were excluded. Subacute or chronic bacterial infections were confirmed in 11 of 17 patients (Table 2). The diagnosis of infective endocarditis was established according to the revised Duke Clinical diagnostic criteria [14]. According to the criteria [14], seven of 11 patients had definitive subacute bacterial endocarditis (SBE) (four of seven patients had two major criteria, and three of seven had one major and three minor criteria). Predisposing factors for SBE were identified in all patients (Table 2). Two had prosthetic valves (patients 1 and 5), one had a pacemaker (patient 7), one had ventriculo-atrial shunt (patient 6), two patients had previous dental procedures (patients 2 and 3), and one patient with Down’s syndrome also had ventricular septal defect (patient 4). In four of seven patients, endocardial involvement was confirmed by echocardiography, while three of seven patients had a new heart murmur (patients 2, 3, and 4).
The diagnosis of cutaneous and pulmonary tuberculosis (TB) was established in two patients by pathohistology of a skin biopsy and Löwenstein’s sputum culture, respectively (Table 2, patients 10 and 11).
Chronic HCV or HCV/HBV viral infections were confirmed in six of 17 patients (Table 3). Chronic HCV infection was diagnosed in six patients (at least two positive determinations) by a third-generation ELISA (Biokit, Barcelona, Spain). At presentation and during the follow-up period, PCR analysis of blood revealed the presence of HCV RNA in one patient (Table 3). HBsAg positivity was detected by ELISA test. Four of six patients had predominant extrahepatic, autoimmune manifestations of HCV or HCV/HBV infection (Table 3).
Kidney biopsies were carried out in 10 of 17 ANCA-positive patients with infections: three patients had crescentic GN (CGN), three had SNGN without typical crescents, three had mesangial glomerulonephritis, and one had diffuse chronic sclerotic GN. DIF was performed in five of 10 patients: Two of five showed IgM and C3 (3+); two of five had IgM, IgG, and C3 (2+) deposits in mesangium; one of five was negative.
Therapy of ANCA-positive patients with prolonged infections
Eight of patients with bacterial infections were treated with antibiotics, while three of 11 with antibiotics and surgery (valve replacement, patients 1, 3, and 6) 3–6 months after recovery. Patient 3 had an amputation of toes after septic embolization. Only patient 7 received antibiotics and three i.v. methylprednisolone pulses of 1,000 mg. Patient 4 was treated with IVIg, 500 mg kg−1 month−1 (Table 2).
Four of six ANCA-positive patients with chronic HCV infection were treated intermittently with corticosteroid therapy (Table 3). Three patients (patients 1, 2, and 3) were treated with pulses of methylprednisolone (three to six pulses of 500–1,000 mg) followed by oral prednisone at 0.5 mg/kg, with gradual dose tapering. One patient (patient 1) was treated with cyclophosphamide (three i.v. pulses at 700 mg/m2). In one case (patient 4), the interferon-α therapy was introduced, but the patient had very pronounced flu-like symptoms and refused further therapy (Table 3).
Methods
First, serum samples were obtained at the time of diagnosis, and none of the patients had previously received IST. Patients with TB had not received antituberculotics before ANCA testing. IgG ANCA titers were determined at the initial visit and at least 6 months thereafter, using an indirect immunofluorescence assay with “in-house” ethanol-fixed preparation of neutrophils, starting with 1:16 dilution, as previously described [15]. PR3-ANCA and MPO-ANCA were detected (cutoff 15 U/mL) by ELISA (Organtec Diagnostica, GmbH, Germany).
Antinuclear (ANA) IgG antibodies were detected by IIF using HEp-2 cells as substrate (Mast Diagnostica, Reinfeld, Germany). Anti-dsDNA IgG antibodies were detected by IIF on Crithidia lucilliae (Mast Diagnostica, Germany). The concentrations of specific antibodies (Sm/RNP, RNP, SS-A, and SS-B) in ANA and antiextractable nuclear antigens (ENA) positive sera were measured (cutoff 15 U/mL) by commercial standard ELISA (Organtec Diagnostica, GmbH). Antihistone (AHA) antibodies (cutoff 40 U/mL) were measured by commercial standard ELISA (Organtec Diagnostica, GmbH).
Concentrations of aCL IgG and IgM (cut-off 10 GPL U/mL and 7 MPL U/mL, respectively) and anti-β-2 glycoprotein (GP) I IgG and IgM (cut-off 5 U/mL) were measured by commercial standard ELISA (Organtec Diagnostica, GmbH).
Concentrations of C3 (normal values 0.8–1.5) and C4 (normal values 0.1–0.4) complement components and C-reactive protein (CRP) (normal values <5 mg/L) were measured by nephelometry (Orion Diagnostica, Espoo, Finland).
The presence (at least two positive determinations) and the type of cryoglobulins were investigated by the standard procedure [16]. Cryoprecipitate was analyzed by immunofixation and by agglutination for the presence of rheumatoid factor (Orion Diagnostica, Espoo, Finland).
Statistical analysis
Frequencies of nonparametric characteristics in AAV- and ANCA-positive patients with infection were compared using χ 2 test or with Fisher’s exact test. Student’s t test was applied in comparisons of continuous variables. Probability (p) values less than 0.05 were considered statistically significant. Data were analyzed by SPSS statistical software version 10.0 for Windows (SPSS, Inc, Chicago, IL, USA).
Results
Demographic characteristics of patients with AAV and prolonged infections
MPO-ANCA- or PR3-ANCA-positive patients with infection were significantly younger (p < 0.01) in comparison to patients with AAV, but there was no division based on gender between the study groups (Table 1). The average duration of symptoms before diagnosis was shorter in patients with infection, but the difference was not statistically significant.
Characteristics of ANCA-positive patients with prolonged infections
Eleven of 17 patients had confirmed bacterial infections (three Streptococcus viridans, one Enterococcus, two coagulase-negative Staphylococcus, three Staphylococcus aureus, two Mycobacterium tuberculosis), while six of 17 had confirmed viral infections (three concomitantly HCV and HBV and three HCV). All relevant clinical, serological, and pathohistological characteristics of PR3-ANCA- and/or/MPO-ANCA-positive patients with associated bacterial and viral infections are presented in Tables 2 and 3.
Clinical differences between patients with AAV and prolonged infections
AAV patients and ANCA-positive patients with infection were characterized by high frequency of arthralgia/myalgia, high fever, and weight loss (Table 4). There were no differences in skin manifestations and renal involvement, including ARF and hematuria between the two study groups (p > 0.05). On the other hand, patients with AAV had significantly more frequent ear/nose/throat (ENT) involvement, pulmonary manifestations, pulmonary–renal syndrome, and nervous system manifestations. ANCA-positive patients with infections had more frequent spleen and/or liver enlargement and new heart murmurs (Table 4).
Serological differences between patients with AAV and prolonged infections
There were no statistical differences in titers and ANCA types between patients with vasculitides and patients with infections (Table 5). On the other hand, patients with infections more frequently expressed dual ANCA positivity (high PR3 and low MPO) together with the presence of ANA, anti-SSA, aCL, anti-β2 GP I, cryoglobulins, and complement consumption (Table 5). For all ANA-positive samples, ANCA/ANA titer ratio was >2. In the group of patients with infections, only one had anti-dsDNA antibodies (titer 1:80), and two patients had anti-SSA (one in low and one in high concentration), one of 17 had antihistone, and one of 17 had anti-Sm/RNP antibodies in low concentration. Nine of 17 (53%) patients with infections had aCL (five IgM, three IgG, and one IgG and IgM). Four of five patients were weakly positive, and one of five was medium positive for IgM aCL. One of three was weakly and two of three were medium positive for IgG aCL. On the other hand, only six of 66 (9%) patients with AAV had aCL (five were weakly IgG positive, and one was medium IgG and IgM positive). IgG and IgM anti-β2 GP I were more frequently present in patients with infections (Table 5). PR3- and/or MPO-ANCA-positive patients with infections and simultaneous presence of ANA and/or aCL did not have other criteria for connective tissue diseases and/or antiphospholipid syndrome.
Low concentrations of C3 and/or C4 were found in eight patients with infections who also had mixed cryoglobulinemia (two of eight patients were ANA positive). Four of eight patients with cryoglobulinemia had bacterial infection, while four of eight patients had chronic HCV infection. Five of eight patients had cryoglobulinemia type II, and three of eight had cryoglobulinemia type III (Tables 2 and 3).
There was no difference in the frequency of high CRP value between AAV and ANCA-positive patients with infections.
There was no difference in the frequency of renal and skin manifestations, presence of autoantibodies, cryoglobulinemia, and low C4 between ANCA-positive patients with bacterial (n=11) and viral (n = 6) infections. Patients with bacterial infections in comparison to patients with viral infections (Tables 2 and 3) had more frequent cANCA (81% versus 50%), but this difference was not statistically significant (p > 0.05).
Follow-up of patients with AAV and prolonged infections
Titers of ANCA and CRP levels decreased slowly after 6 months in both study groups (Table 6). After 6 months, three of 17 patients with infections recovered with disappearance of ANCA, while in nine patients (six cANCA and three pANCA), ANCA titers decreased (Tables 2, 3, and 6) but remained positive. In patients with infections, clinical remission preceded the disappearance of ANCA, especially pANCA, whose titer remained relatively high (median 1/128) after 6 months. After prolonged follow-up (median 2 years), seven of nine patients remained with low ANCA titers (four cANCA and three pANCA) (Tables 2 and 3). High titers of ANCA persisted in four patients with various autoimmune manifestations of HCV infection (Table 3, patients 1, 2, 3, and 5). By contrast, ANCA titer decreased during remission in patients with AAV (Table 6).
ANA, aCL, anti-β2 GP I, and cryoglobulins disappeared after 6 months in all patients, except in three HCV positive patients and one patient with SBE. Six of eight ANCA-positive patients with protracted infections who had cryoglobulins and hypocomplementemia at presentation, developed ARF or chronic renal failure (CRF) during the follow-up period. In patients with infections, concomitant presence of cryoglobulins and hypocomplementemia was associated with ARF or CRF (p ≤ 0.05).
During the first episode of the disease, lethal outcome occurred in six of 66 (9%) patients in the AAV group and in four of 17 (23%) patients in the infection-associated group (p < 0.05) (Tables 2 and 3).
More relapses were observed in the AAV (95% of patients had at least one relapse) group (p < 0.001), while only four HCV-positive patients had relapses of GN (Table 3 and 6).
Patients with AAV were statistically more frequently treated with IST (Table 6). Ten of 11 patients with bacterial infections (Table 2) were treated with antibiotics, eight of 10 recovered, and two of 10 died (patient 4 with SBE of heart failure and patient 11 with TB or respiratory failure). One of 11 cases (patient 7) who received three i.v. methylprednisolone pulses of 1,000 mg progressed to terminal renal failure (TRF) and died of heart failure. One person (patient 4) with chronic HCV/HBV infection died of pneumonia (Table 3).
During the follow-up period, the following final outcomes were registered: 13 of 66 (20%) AAV patients died, 30 of 66 (45%) developed CRF, and nine of 66 (14%) developed TRF. Four of 17 (23%) patients with infections died, four of 17 (23%) patients developed CRF, and one of 17 (6%) developed TRF (Table 6). There was no difference in frequency of lethal outcomes, CRF, and TRF in patients with AAV and infections associated with ANCA (Table 6).
Discussion
AAV with renal involvement are rare diseases with the mean annual incidence of 1.6 per 100,000 adults and have seasonal, annual, and geographic fluctuation [17, 18]. It is possible that such fluctuations are due to environmental factors, especially to infectious agents. Interestingly, ANCA was described for the first time in eight patients suffering from arbovirus infection [17].
WG, MPA, and CSS are predominantly illnesses of elderly or middle-aged people [1, 18], and this can explain the significantly higher number of younger patients in our group of PR3- and/or MPO-ANCA-positive patients with infections.
In the group of ANCA-positive patients with infections, streptococcal and staphylococcal infections are of special interest. The association of SBE and suppurative skin infections with ANCA has been previously reported [8, 19]. The role of bacterial superantigens as trigger factors has been established: The higher relapse rate in patients with WG who are S. aureus nasal carriers has been well documented [2, 20]. Also, a marked increase in the expression of T cell receptor V β 2.1, which recognizes superantigens, was found in WG and MPA patients [2, 21].
Our experience confirms that ANCA may be induced by M. tuberculosis, as previously reported [22]. Among 45 patients with tuberculosis, ANCA was detected in 20 persons (16 cANCA and four pANCA), while 18 patients had positive ANCA on ELISA (15 PR3 and three MPO) [22]. Generally, clinical and histological similarities between mycobacterial infections and WG implicate that positive ANCA tests must be carefully interpreted.
Standard clinical and serologic criteria for differentiating AAV from ANCA-positive patients with prolonged infections are inadequate, especially at the initial disease presentation. Both groups of ANCA-positive patients had subacute presentation without the difference in the duration of the nonspecific symptoms (Table 1). Analysis of clinical parameters (Table 4) showed that first symptoms (arthralgias, myalgias, weight loss, and fever over 38.5°C) were very similar. There were no differences in frequency of kidney involvement and various skin manifestations in idiopathic and infection-related group (Table 4). By contrast, involvement of ENT, lungs, nervous system, and pulmonary–renal syndrome, which are typical for AAV [1, 9], were less frequently observed in ANCA-positive patients with prolonged infections (Table 4).
The differential diagnosis between SBE and AAV may be difficult [8, 23], especially if a heart murmur is absent, as in four of our seven patients with SBE (Table 2). Minor criteria for SBE [14], including a slow indolent course with fever, GN, and purpura, overlap with those of the AAV (Table 2). Chirinos et al. collected literature data on eight ANCA-positive cases with SBE who had subacute constitutional symptoms, elevated erythrocyte sedimentation rate, hematuria, and/or proteinuria, and seven of eight had anemia and skin manifestations, most often purpura [10]. Osler's nodes, Janeway lesions, and splinter hemorrhages typical for SBE may mimic cutaneous vasculitis in AAV. Other studies also demonstrated that manifestations such as GN, arthritis, purpura, pulmonary infiltrates, epistaxis, and sinus symptoms typical for AAV are often present in ANCA-positive patients with SBE [8, 24, 25]. Sometimes, splenomegaly or hepatosplenomegaly can be useful clinical parameters, because they are more frequently seen in SBE, as we found in our patients [10].
The presence of ANCA in SBE patients has been previously reported [8, 25, 26]. ANCA were more frequently specific to PR3 with concomitant presence of organ-nonspecific autoantibodies (ANA, aCL), the same as in our study [8, 10, 24–26]. Genetic sequences of S. aureus, one of microorganisms causing SBE, are complementary to critical sequence of PR3 [27]. Until now, there were only two reports of MPO-ANCA positivity in patients with SBE [28, 29]. In our group, two of seven patients with SBE were MPO-ANCA positive, and one of them developed ARF with lethal outcome.
How infections produce ANCA in SBE in not clear, but in an experimental system, the immunization of rats with pasteurized protein from Escherichia coli and S. aureus resulted in circulating ANCA and in pauci-immune SNGN [30]. It has been shown that B cells, stimulated by bacterial unmethlylated oligodeoxynucleotides via toll-like receptor 9 (TLR9), produce ANCA [31]. The recently described release of neutrophil extracellular traps (NETs), containing target autoantigens PR3 and MPO, are also important [32].
Although chronic bacterial infections are more frequently associated with ANCA, chronic HCV infection can also induce ANCA against MPO, PR3, and bactericidal permeability increasing protein and cathepsin G [9, 12, 33]. Chronic HCV infection implicates prolonged antigen stimulation and severe autoimmune manifestations, often without clinical important hepatitis [6]. Adults and young patient from our group with chronic HCV or HCV/HBV infection had various autoimmune manifestations, including recurrent purpura, arthralgias, livedo, GN, and polyneuropathy. Both PR3-ANCA and MPO-ANCA were reported in HCV infection [12, 33, 34]. The over-expression of CD81 and the expansion of CD5+ B lymphocytes in HCV-infected patients may play a role in the development of HCV-associated autoimmunity [35]. According to all these data, we recommend routine testing for HCV in PR3-ANCA and/or MPO-ANCA-positive patients, especially in communities with a high prevalence of HCV infection.
In spite of similar clinical findings, our study demonstrates that AAV patients and ANCA-positive patients with prolonged infections have different serological profiles. Patients with infections more frequently expressed dual ANCA positivity (PR3 high/MPO low) together with presence of ANA, cryoglobulins, complement consumption, aCL, and anti-β2 GP I. There are few reports of dual, PR3-ANCA, and MPO-ANCA positivity in SBE and HCV infections [13, 36, 37]. Interestingly, drug-induced ANCA vasculitis can be also positive for both PR3-ANCA and MPO-ANCA [38]. By contrast, as we also found, only a few patients with AAV exhibited both PR3-ANCA and MPO-ANCA specificities [9].
Mixed cryoglobulinemia with hypocomplementemia that we found in our patients was reported in ANCA-associated bacterial and viral infections [6, 10, 13, 33]. HCV core particles that concentrate in the cryoprecipitate may play a role in the interactions between cryoglobulins, endothelial cells, and neutrophils [33]. We found that in patients with infections, concomitant presence of ANCA, cryoglobulins, and complement consumption was associated with severe GN. Neumann et al. reported significantly higher levels of proteinuria in ANCA-positive patients with cryoglobulinemia and low complement level [36]. Contrary to AAV, DIF of renal biopsy in ANCA-positive patients with infections demonstrate presence of immune deposits [39]. Accordingly, screening for cryoglobulins and the determination of autoantibodies and complement components levels, together with histological and immuhistological findings, are mandatory in ANCA-positive patients with infection.
Many questions about multiple serological abnormalities in ANCA-positive patients with infection, as found in our cases, remain unresolved. Simultaneous presence of various antibodies (ANA, aCL, β2-GP I) suggests that apoptotic blebs on primed neutrophils could be a source of autoantigens in ANCA-positive patients with prolonged bacterial infections [40]. Failure to remove apoptotic neutrophils might result in spreading of autoimmune response and induction of dual ANCA (high PR3/low MPO) in some patients with infections. Binding of ANCA to PR3 and MPO, expressed on the surface of primed neutrophils, induces secretion of TNF-α, IL-8, IL-1, proteases, and stimulates production of oxygen radicals with further enhancement of inflammation [41].
Recently described release of NETs, composed of decondensed chromatin and targeted autoantigens PR3 and MPO, might explain concomitant presence of ANCA and ANA in our patients with chronic infections [32]. It was shown that chromatin in NETs is degraded by extracellular DNAses to soluble nucleosomes, which can trigger production of ANA [42]. The extracellular DNA, modified by antimicrobial proteins, can activate plasmacytoid dendritic cells to produce type 1 interferons via TLR9 [43]. ANCAs are potent activators of NETs formation with induction of the enzyme peptidyl arginin deiminase, which covalently modify nuclear autoantigens, especially histone [44]. Cooperation between ANCA and microbial components during infection could contribute to the observed serological profile of patients with prolonged infections.
Early diagnosis and therapy remain a big challenge in infections associated with ANCA [13, 45]. Our study demonstrated that there were no differences in frequency of CRF, TRF, and lethal outcomes in patients with AAV and infections associated with ANCA. There are a few reports on IST in ANCA-positive patients following SBE [13, 25, 26]. In most of our patients with bacterial infections, an effective antimicrobial therapy or a surgical eradication of infection stopped the sequence of inflammation, resulting in the remission and gradual decrease of ANCA titers. Further studies are needed to standardize the balanced antimicrobial and IST for protracted infections associated with ANCA.
In conclusion, although PR3-ANCA and MPO-ANCA are serological markers for AAV, the interpretation of PR3-ANCA and/or MPO-ANCA positivity should consider the possibility of protracted infection (Streptococcus spp., Staphylococcus spp., and HCV were the most frequent pathogens). We demonstrated that, despite similar constitutional, renal, and skin manifestations, AAV patients and ANCA-positive patients with protracted infections have different serological profiles. The patients with protracted infections more frequently had concomitant PR3-ANCA and MPO-ANCA positivity, ANA, IgM aCL, IgG and IgM anti-β2 GP I, cryoglobulins, and low C3 and/or C4. Concomitant presence of ANCA, cryoglobulins, and complement consumption in patients with infections was associated with severe course of GN. ANCA testing should be repeated after specific antimicrobial therapy, since some cases might require intermittent IST.
References
Jennette JC, Falk RJ, Andrassy K et al (1994) Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum 37:187–192
Kallenberg CG, Tadema H (2008) Vasculitis and infections: contribution to the issue of autoimmunity reviews devoted to “autoimmunity and infection”. Autoimmun Rev 8:29–32
Wiik A (2008) Drug-induced vasculitis. Curr Opin Rheumatol 20:35–39
Bonaci-Nikolic B, Nikolic MM, Andrejevic S et al (2005) Antineutrophil cytoplasmic antibody (ANCA)-associated autoimmune diseases induced by antithyroid drugs: comparison with idiopathic ANCA vasculitides. Arthritis Res Ther 7:1072–1081
Guillevin L, Lhote F, Gherardi R (1997) The spectrum and treatment of virus-associated vasculitides. Curr Opin Rheumatol 9:31–36
Ramos-Casals M, Jara LJ, Medina F et al (2005) HISPAMEC Study Group. Systemic autoimmune diseases co-existing with chronic hepatitis C virus infection (the HISPAMEC Registry): patterns of clinical and immunological expression in 180 cases. J Intern Med 257:549–557
Asherson RA, Cervera R (2003) Antiphospholipid antibodies and infections. Ann Rheum Dis 62:388–393
Choi HK, Lamprecht P, Niles JL et al (2000) Subacute bacterial endocarditis with positive cytoplasmic antineutrophil cytoplasmic antibodies and anti-proteinase 3 antibodies. Arthritis Rheum 43:226–231
Schmitt WH, van der Woude FJ (2004) Clinical applications of antineutrophil cytoplasmic antibody testing. Curr Opin Rheumatol 16:9–17
Chirinos JA, Corrales-Medina VF, Garcia S et al (2007) Endocarditis associated with antineutrophil cytoplasmic antibodies: a case report and review of the literature. Clin Rheumatol 26:590–595
Chou TN, Hsu TC, Chen RM et al (2000) Parvovirus B19 infection associated with the production of anti-neutrophil cytoplasmic antibody (ANCA) and anticardiolipin antibody (aCL). Lupus 9:551–554
Wu YY, Hsu TC, Chen TY et al (2002) Proteinase 3 and dihydrolipoamide dehydrogenase (E3) are major autoantigens in hepatitis C virus (HCV) infection. Clin Exp Immunol 128:347–352
Zeledon JI, McKelvey RL, Servilla KS et al (2008) Glomerulonephritis causing acute renal failure during the course of bacterial infections. Histological varieties, potential pathogenetic pathways and treatment. Int Urol Nephrol 40:461–470
Li JS, Sexton DJ, Mick N et al (2000) Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 30:633–638
Radice A, Vecchi M, Bianchi MB, Sinico RA (2000) Contribution of immunoflorescence to the identification and characterization of anti-neutrophil cytoplasmic autoantibodies. The role of different fixatives. Clin Exp Rheum 18:707–712
Lamprecht P, Gause A, Gross WL (1999) Cryoglobulinemic vasculitis. Arthritis Rheum 42:2507–2516
Davies DJ, Moran JE, Niall JF, Ryan GB (1982) Segmental necrotizing glomerulonephritis with antineutrophil antibody: possible arbo virus aetiology? Br Med J 285:606
Tidman M, Olander R, Svalander C, Danielsson D (1998) Patients hospitalized because of small vessel vasculitides with renal involvement in the period 1975–95: organ involvement, anti-neutrophil cytoplasmic antibodies patterns, seasonal attack rates and fluctuation of annual frequencies. J Intern Med 244:133–141
Chan B, d'Intini V, Savige J (2006) Anti-neutrophil cytoplasmic antibody (ANCA)-associated microscopic polyangiitis following a suppurative wound infection. Nephrol Dial Transplant 21:2993–2994
Popa ER, Stegeman CA, Abdulahad WH et al (2007) Staphylococcal toxic-shock-syndrome-toxin-1 as a risk factor for disease relapse in Wegener's granulomatosis. Rheumatology 46:1029–1033
Simpson IJ, Skinner MA, Geursen A et al (1995) Peripheral blood T lymphocytes in systemic vasculitis: increased T cell receptor V beta 2 gene usage in microscopic polyarteritis. Clin Exp Immunol 101:220–226
Flores-Suárez LF, Cabiedes J, Villa AR et al (2003) Prevalence of antineutrophil cytoplasmic autoantibodies in patients with tuberculosis. Rheumatology 42:223–229
Leff RD, Hellman RN, Mullany CJ (1999) Acute aortic insufficiency associated with Wegener granulomatosis. Mayo Clin Proc 74:897–899
de Corla-Souza A, Cunha BA (2003) Streptococcal viridans subacute bacterial endocarditis associated with antineutrophil cytoplasmic autoantibodies (ANCA). Heart Lung 32:140–143
Chaw HY, Buxton N, Wong PS (2004) Staphylococcal endocarditis with a ventriculo-atrial shunt. J R Soc Med 97:182–183
Haseyama T, Imai H, Komatsuda A et al (1998) Proteinase-3-antineutrophil cytoplasmic antibody (PR3-ANCA) positive crescentic glomerulonephritis in a patient with Down's syndrome and infectious endocarditis. Nephrol Dial Transplant 13:2142–2146
Pendergraft WF 3 rd, Preston GA, Shah RR et al (2004) Autoimmunity is triggered by cPR-3(105–201), a protein complementary to human autoantigen proteinase-3. Nat Med 10:72–79
Hellmich B, Ehren M, Lindstaedt M et al (2001) Anti-MPO-ANCA-positive microscopic polyangiitis following subacute bacterial endocarditis. Clin Rheumatol 20:441–443
Miranda-Filloy JA, Veiga JA, Juarez Y et al (2006) Microscopic polyangiitis following recurrent Staphylococcus aureus bacteremia and infectious endocarditis. Clin Exp Rheumatol 24:705–706
Savige JA, Nassis L, Cooper T et al (2002) Antineutrophil cytoplasmic antibody (ANCA)-associated systemic vasculitis after immunisation with bacterial proteins. Clin Exp Rheumatol 20:783–790
Hurtado PR, Jeffs L, Nitschke J et al (2008) CpG oligodeoxynucleotide stimulates production of anti-neutrophil cytoplasmic antibodies in ANCA associated vasculitis. BMC Immunol 9:34. doi:10.1186/1471-2172-9-34
Papayannopoulos V, Zychlinsky A (2009) NETs: a new strategy for using old weapons. Trends Immunol 30:513–521
Lamprecht P, Schmitt WH, Gross WL (1998) Mixed cryoglobulinaemia, glomerulonephritis, and ANCA: essential cryoglobulinaemic vasculitis or ANCA-associated vasculitis? Nephrol Dial Transplant 13:213–221
Igaki N, Nakaji M, Moriguchi R et al (2000) A case of hepatitis C virus-associated glomerulonephropathy presenting with MPO-ANCA-positive rapidly progressive glomerulonephritis. Nippon Jinzo Gakkai Shi 42:353–358
Zuckerman E, Slobodin G, Kessel A et al (2002) Peripheral B-cell CD5 expansion and CD81 overexpression and their association with disease severity and autoimmune markers in chronic hepatitis C virus infection. Clin Exp Immunol 128:353–358
Neumann I, Regele H, Kain R et al (2003) Glomerular immune deposits are associated with increased proteinuria in patients with ANCA-associated crescentic nephritis. Nephrol Dial Transplant 18:524–531
Tiliakos AM, Tiliakos NA (2008) Dual ANCA positivity in subacute bacterial endocarditis. J Clin Rheumatol 14:38–40
Chen YX, Yu HJ, Ni LY et al (2007) Propylthiouracil-associated antineutrophil cytoplasmic autoantibody-positive vasculitis: retrospective study of 19 cases. J Rheumatol 34:2451–2456
Fukuda M, Motokawa M, Usami T et al (2006) PR3-ANCA-positive crescentic necrotizing glomerulonephritis accompanied by isolated pulmonic valve infective endocarditis, with reference to previous reports of renal pathology. Clin Nephrol 66:202–209
Yang JJ, Tuttle RH, Hogan SL et al (2000) Target antigens for anti-neutrophil cytoplasmic autoantibodies (ANCA) are on the surface of primed and apoptotic but not unstimulated neutrophils. Clin Exp Immunol 121:165–172
Muller Kobold AC, van der Geld YM, Limburg PC et al (1999) Pathophysiology of ANCA-associated glomerulonephritis. Nephrol Dial Transplant 14:1366–1375
Kessenbrock K, Krumbholz M, Schönermarck U et al (2009) Netting neutrophils in autoimmune small-vessel vasculitis. Nat Med 15:623–625
Lande R, Gregorio J, Facchinetti V et al (2007) Plasmacytoid dendritic cells sense self-DNA coupled with antimicrobial peptide. Nature 449:564–569
Neeli I, Khan SN, Radic M (2008) Histone deimination as a response to inflammatory stimuli in neutrophils. J Immunol 180:1895–1902
Csernok E, Lamprecht P, Gross WL (2010) Clinical and immunological features of drug-induced and infection-induced proteinase 3-antineutrophil cytoplasmic antibodies and myeloperoxidase-antineutrophil cytoplasmic antibodies and vasculitis. Curr Opin Rheumatol 22:43–48
Acknowledgment
Supported by the Ministry of Science of the Republic of Serbia, grant no. 145032.
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bonaci-Nikolic, B., Andrejevic, S., Pavlovic, M. et al. Prolonged infections associated with antineutrophil cytoplasmic antibodies specific to proteinase 3 and myeloperoxidase: diagnostic and therapeutic challenge. Clin Rheumatol 29, 893–904 (2010). https://doi.org/10.1007/s10067-010-1424-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-010-1424-4