
Abstract
Homoeopathy is often advocated for fibromyalgia (FM) and many FM patients use it. To critically evaluate all randomised clinical trials (RCTs) of homoeopathy as a treatment for FM, six electronic databases were searched to identify all relevant studies. Data extraction and the assessment of the methodological quality of all included studies were done by two independent reviewers. Four RCTs were found, including two feasibility studies. Three studies were placebo-controlled. None of the trials was without serious flaws. Invariably, their results suggested that homoeopathy was better than the control interventions in alleviating the symptoms of FM. Independent replications are missing. Even though all RCTs suggested results that favour homoeopathy, important caveats exist. Therefore, the effectiveness of homoeopathy as a symptomatic treatment for FM remains unproven.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fibromyalgia (FM) is a chronic pain condition which can be challenging to treat with conventional medicine [1]. This could be one reason why FM patients frequently turn to complementary and alternative medicine (CAM) [2]. Homoeopathy is one form of CAM that has become a popular treatment choice [3]. Several aspects of the treatment (e.g, long, empathetic consultation and a high degree of individualising the remedies), might make it particularly attractive to patients with FM.
The homoeopathic approach involves a largely somatically focussed assessment alongside the actual treatment (the remedy) whilst emotional symptoms are also assessed and assumed to be targeted by the remedy. Thus, homoeopathy accommodates the multidimensional nature of FM symptoms. According to the concepts of classical homoeopathy, if the optimal remedy is correctly prescribed, any co-existing emotional factors will also be alleviated in conjunction with the physical symptoms [4]. However, as the mechanism for homoeopathic action, if any, is not evident, it seems necessary to ascertain the extent that homoeopathic remedy per se is the trigger for any clinical outcome.
The aim of this systematic review was to evaluate whether homoeopathic treatments can have a therapeutic effect on the symptoms of fibromyalgia.
Methods
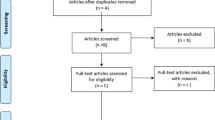
The following databases were searched from their inception to August 2009; MEDLINE, EMBASE and PSYCHINFO via the OVID interface, CINAHL and AMED via the EBSCO interface and CENTRAL via the Cochrane library. No restrictions were applied regarding language or time (Fig. 1). Reference lists of all full text articles were hand-searched for additional studies as were bibliographies of major reviews [5–7].

Search strategy MEDLINE (via OVID)
Study selection
All titles and abstracts retrieved from the searches were assessed for eligibility. All articles appearing to meet the inclusion criteria based on reading the abstract were retrieved as full documents and independently considered for inclusion by two reviewers (RP, RT). Disagreements were resolved through discussion with the third author (EE). For inclusion into the review, trials were required to meet the following pre-defined criteria: participants had to be recruited into the trial based on a diagnosis of FM with the selection criteria made transparent to the reader (e.g, self referrals/referral from specialist centre). The intervention had to be a homoeopathic medicine or homoeopathic package of care; the remedy selection could be individualised and therefore change as the treatment progressed. The remedy selection needed to be carried out by a qualified homoeopath. Placebo, no treatment, treatment as usual or waiting list control groups were permissible for the control groups. The primary outcomes had to be either: the severity of FM symptoms as measured by validated assessment tool (e.g., Fibromyalgia Impact Questionnaire; FIQ), standardised measures of pain (e.g., visual analogue scales were acceptable), tender point count and fatigue; emotional health (as rated by patient or observer); need for medication; physical functioning; sleep quality or quality of life measure. Only studies that were described as randomised clinical trials (RCT), which evaluated the effectiveness of homoeopathy versus an appropriate comparator (as outlined above) were included. Only completed studies were included (reports of ongoing trials were excluded). Data from included studies were extracted independently by two reviewers (RP, RT) using a standardised form with pre-defined criteria. Disagreements between reviewers were resolved through discussions with the third author.
Quality assessment
The methodological quality of all included RCTs was evaluated independently by two researchers (RP, RT) using the Jadad score [8]. Further methodological quality data were extracted based on recommendations from the Cochrane Handbook of Systematic Reviews of Interventions (Cochrane Collaboration 2008) [9] and the Jadad Criteria for Clinical trials on Pain Management, 2000 [10].
Meta-analysis
A meta-analysis was considered but this plan had to be abandoned due to the clinical heterogeneity of the primary data.
Results
Four studies fulfilled the above criteria and are summarised in Tables 1 and 2.
Fisher [11] performed a randomised, double blind, placebo-controlled trial to compare the effectiveness of three commonly used homoeopathic remedies for FM; Rhus toxicodendron, Arnica montana or Bryonia. Twenty-four patients with FM were assessed in terms of sleep, pain, number of tender spots and analgesic consumption at baseline, 1, 2 and 3 months. Each patient’s symptom picture was scored for goodness-of-fit to the remedy selected. The experimental group received one of the three remedies in 6c potency twice a day for 3 months. The placebo group took indistinguishable placebos during the same period of time. Analysis of the differences between groups in terms of pain and sleep measured by visual analogue scales (VAS) showed no significant effects: p = 0.19, p = 0.078, respectively. However, when broken down to distinguish between well-indicated remedies as opposed to poorly indicated remedies there were significant differences (p < 0.05) in pain scores and in sleep scores (at 2 and 3 months) for those participants whose remedies were optimal fits. There was no significant difference in tender spot counts between groups and analgesic consumption results were not reported.
In 1989, Fisher et al. [12] carried out another RCT specifically assessing the effects of R. toxicodendron 6c in the treatment of FM. The decision to use just this remedy was based upon the results of the previous study indicating 42% of FM patients fitted the R. toxicodendron picture. This study used a cross-over design. Thirty FM patients, fitting the R. toxicodendron picture (as established by a homoeopath), received both active treatment and placebo treatment in random order for 1 month each. The dose was two tablets three times daily. After the initial consultation, there was no further contact with the homoeopath. At the end of the treatment period, the number of tender points in the placebo group was significantly higher than in the experimental group (p < 0.005). Improvements in pain and sleep, measured by a combined VAS, was also significantly greater for the rhus tox group compared to the placebo group (p = 0.0052). A re-analysis of Fisher’s data was published by Colquon in 1991 [13]. Distribution-free randomisation tests were applied separately to the scores of pain, sleep and tender points and no significant treatment effects after the first treatment period was found.
Bell et al. [14, 15] carried out an RCT testing the feasibility of using homoeopathic remedies in the treatment of FM. Sixty-two FM patients were included. Rather than assessing the efficacy of just one or a few homoeopathic remedies, remedy selection was kept completely open, resulting in 41 remedies being utilised in the trial. LM remedies (diluted to 1 in 50,000) in solution were used. Patients were interviewed and assessed by two homoeopaths at baseline, 2 and 4 months. They were able to change the remedy or the dosage at any time (which emulates how homoeopaths work). Primary outcome measures were collected at baseline, 3 months (and 6 months after cross-over option). After 4 months, all patients were given the option to change group for an additional 2 months. At 3-month follow-up, for treatment completers, the experimental group showed a significant greater improvement in tender point count (p < 0.05) and tender point pain on palpation (p < 0.01), appraisal of FM scores (p < 0.05) and global health rating (p < 0.05; data adjusted for anger and depression). Further analysis indicate that a significantly higher proportion of patients in the homeoapthy group experienced at least a 25% improvement in tender point pain on examination (13/26) versus placebo group (four/27), (Fisher’s exact test, two-tailed, p = 0.008). There was a trend for the homoeopathic group to improve on the affective dimension of the McGill Pain Questionnaire (MPQ), POMs depression and POMs anger-hostility (all p < 0.10). At 6 months [15], those who had decided to stay in the experimental group rather than switch, showed significantly greater gains in global health than the placebo-switch subgroup.
Rather than assessing the specific effects of the homoeopathic remedy in isolation, Relton [16] compared a homoeopathic package of care as an adjunct to usual care with usual care alone in a pilot, feasibility study. Forty-seven FM patients were recruited and assessed at baseline and 22 weeks on a number of outcome measures. The primary outcome measure was the FIQ total score. Intent to treat between groups analysis found a significantly greater reduction in the FIQ total scores (p < 0.01) for the homoeopathic package of care being observed, but no significant difference in FIQ pain scores was found. In the completers’ sample between-groups change score analysis, there were significantly greater reductions in the McGill pain scores, McGill Affective Scores, McGill Affective and Sensory Scores, the FIQ fatigue and the tiredness upon waking scores in the homoeopathic care group than the usual care group (all p < 0.05). In addition, the number of days felt good (p < 0.05) was significantly greater in the homoeopathy group. There were no significant differences in tender point count, EuroQol, MYMOPS or HADS between the groups.
Discussion
All four RCTs included in this systematic review reported evidence supporting the effectiveness of homoeopathy compared to placebo or to usual care. However, none of them is free from flaws.
The first study by Fisher suggested no effect of the homoeopathic treatments for the total group of patients but a significant result in favour of homoeopathy when broken down into well-indicated remedies. The fact that the authors individualised the remedies to some degree indicates a more realistic approach to homoeopathic practice, although total individualisation of remedy selection would have been more in keeping with concepts of classical homoeopathy. The main points of critique are the very small sample size and the short duration of treatment. The paucity of details given on the randomisation process means that it is impossible to assess its appropriateness. The lack of demographic information on the patients limits interpretation of the study findings.
In 1989, Fisher et al suggested that a homoeopathic remedy can lead to improvements greater than those of a placebo. A repeated measures design was used with no washout period between active and placebo. As homoeopathic remedies are claimed to continue having an effect long after the remedy has been administered, the possibility that the data were confounded by carryover treatment effects cannot be discounted. Further problems with the study were the small sample size, insufficient information relating to the randomisation procedure and no demographic data of the patients. The re-analysis by Colquhoun [13] suggested that there was no evidence for the efficacy of homoeopathic treatment when distribution-free randomisation tests were employed. He criticised Fisher for combining pain and sleep scores thus invalidating the results.
The feasibility study by Bell et al. [14] was a well-constructed RCT (albeit slightly underpowered) which scored highly on methodological quality (Jadad score 4), only failing to obtain the highest Jadad score of 5 because reasons for drop out were reported for all of the participants rather than by group. The randomisation process was transparent and appropriate (computer generated with treatment allocation concealed), and an indistinguishable placebo was used. A detailed description of participants was disclosed to enable assessment of generalisability. Bell et al. individualised the remedy selection and allowed for changes to remedy and dosage (as in real homoeopathic prescribing). There was no restriction on remedy chosen except that it had to be given as an LM potency. They included a large number of outcome measures which generated large amounts of data. In terms of the crossover part of the trial [15], it has been argued that a longer washout period is needed between receiving the active and placebo solution; estimating a 1 month per year of the suffering [17]. Interpretation of the results obtained during the crossover period is more problematic as it is difficult to establish whether the lack of washout period had confounded the data obtained from active-switch group. Nonetheless, interesting differences between groups were observed which suggests that homoeopathic remedies were affecting FM symptoms over and above the non-specific placebo effects.
One proposed mechanism for homoeopathy is time-dependant sensitisation (“the progressive, persistent amplification of responses within a susceptible individual from repeated, intermittent exposures to an environmental factor, pharmacological or non-pharmacological in nature” [18]). In addition to the primary paper, Bell et al published further articles [18] on this study examining possible sensitisation-related changes in electroencephalography (EEG) relative alpha magnitude in order to test the hypothesis that repeated administration of individualised homoeopathic remedies will produce measurable increases in EEG alpha responses over time. In line with their hypothesis, the authors reported significant patterns of progressive increases in alpha (1 and 2) magnitudes during the sniff tests in the active group, whereas the placebo group’s declined between the initial and 3-month sessions. Baseline measures of alpha did not differ which indicates it is the homoeopathic remedy that brings about the effect. Over the whole sample at the end of the 6-month study, increased alpha magnitudes correlated significantly with total amount of time on active remedy treatment either due to randomised assignment or optional crossover decision which is consistent with the time dependant sensitisation (TDS) hypothesis that it is amount of time on the remedy rather than dosage. Although not a clinical outcome, the investigation of the physiological differences in neurological responses between conditions is an important development in homoeopathic research.
Bell et al. [19] also looked at EEG cordance in relation to responses to homoeopathic treatment. This is a measure derived from absolute and relative scalp EEG power which has been found to correlate with patterns of brain blood flow and metabolic functional neuro-imaging studies. Based on evidence from prior depression studies [20, 21] they hypothesised that there would be differences in EEG cordance between exceptional and non-exceptional responders to homoeopathic treatment. When EEG cordance was analysed, the six “exceptional responders” had more negative initial EEG cordance difference scores in the prefrontal cortex (FP1 and FP2). Right prefrontal cordance correlated significantly with reduced local pain and trait absorption (ability to focus attention selectively and fully). The authors also reported a significant finding at the 10% level in improvement in global health.
Although the findings of the study were interesting, they need replication before any firm conclusions can be drawn, both the EEG and cordance studies provide some indication that homoeopathic remedies might lead to physiological responses which differ from non-specific or placebo responses to homoeopathic intervention. Both studies highlight the need to consider differences in individual characteristics which may correlate with or predict trial outcomes.
Relton et al. [16] also reported favourable results. The design of this study did not control for placebo effects, although the authors make it clear that they did not set out to test whether homoeopathic remedies work better than placebo. They aimed at testing the feasibility of using a homoeopathic package of care in addition to usual care. Arguably, the results would have been more meaningful if Relton had compared the homoeopathic package of care with the same package of care where patients saw a homoeopath for an equal length of time but did not receive an active treatment, instead a placebo sugar pill. This would have controlled for the non-specific effects of the therapeutic setting that may have brought about the positive effects found in this study. A systematic review of trials adopting this design has shown that such studies will always generate a positive result, even if the experimental treatment has no specific therapeutic effects [22]. In addition, a high drop-out rate in the usual care group was observed in Relton et al’s study (eight/24) which reduced the power of the study. The between-group analyses from the trial completers look favourable for homoeopathy but with such a large drop-out in the usual care group, it is difficult to relate to the homoeopathic treatment alone. The only significant result from the intent-to-treat sample was a greater reduction in the FIQ total score in the homoeopathic care group −6.53 (15.03) p < 0.01 than usual care. This study, however, does not tell us much about homoeopathy per se.
When evaluating the evidence for or against homoeopathy one should briefly comment on the plausibility of this treatment. Homoeopathy is based on two main principles [4]. The Law of Similars claims that, if a substance causes symptoms in healthy volunteers, it can be used to treat these symptoms effectively when they occur in patients. The law of the infinitesimal dose holds that, if a substance is serially diluted in the homoeopathic way, it becomes not weaker but stronger, even if the dilution is beyond Avogadro’s number. Currently, there is little scientific evidence to support these theoretical principles. It is therefore difficult to accept that homoeopathy is biologically plausible [23]. Bell et al’s [18] research into TDS, however, does provide an alternative methodology for investigation physiological changes in response to homoeopathic remedies.
Our review has a number of limitations. Even though our searches were thorough, we cannot be sure that all relevant RCTs were located. Negative studies tend to remain unpublished [24]. This bias could therefore have distorted the overall picture. All the four RCTs tested different homoeopathic treatments or approaches; this means that no independent replication of any of the tested approaches exists. The paucity and, at times, disappointing quality of the available RCTs render firm conclusions problematic.
In summary, the findings of the four existing RCTs all favour homoeopathy over controls. Yet none of the studies is sufficiently rigorous to provide a definitive answer. Future studies should minimise bias more effectively than did the trials available so far.
References
http://www.privatehealth.co.uk/diseases/arthritic-bone-muscle/fibromyalgia
Pioro-Boisset M, Esdaile JM, Fitzcharles MA (1996) Alternative medicine use in fibromylagia syndrome. Arthritis Care Res 9:13–17
Breuer GS, Orbach H, Elkayam O, Berkun Y, Paran D, Mates M, Nesher G (2005) Perceived efficacy among patients of various methods of complementary alternative medicine for rheumatologic diseases. Clin Exp Rheumatol 23(5):693–696
Hahnemann S. The Organon. 1842 Homeopathic Publications. New Dehli
Kleijnen J, Knipschild P, ter Riet G (1991) Clinical trials in homeopathy. Br Med J 302:316–323
Linde K, Clausius N, Ramirez G, Melchart D, Eitel F, Hedges LV, Jonas WB (1997) Are the clinical effects of hompeathy placebo effects? A meta-anaylsis of placebo-controlled trials. Lancet 350:834–843
Shang A, Huwiler-Müntener K, Nartay L, Jüni P, Dörig S, Sterne J et al (2005) Are the clinical effects of homeopathy placebo effects? Comparative study of placebo-controlled trials of homeopathy and allopathy. Lancet 366:726–732
Jadad AR, Moore RA, Carroll D et al (1996) Assessing the quality of reports of randomized controlled trials: is blinding necessary? Control Clin Trials 17(1):1–2
Cochrane Collaboration. Cochrane Handbook: assessing risk of bias in included studies. Chapter 8 (2008) Accessed at http://www.cochrane-handbook.org/
Ezzo J et al (2000) Is acupuncture effective for the treatment of chronic pain? A systematic review. Pain 86:217–225
Fisher P (1986) An experimental double-blind clinical trial method in homeopathy. Use of a limited range of remedies to treat fibrositis. Br Homeopath J 75(3):142
Fisher P, Greenwood G, Huskisson EC, Turner P, Belon P (1989) Effects of homeopathic treatment on fibrositis (primary fibromyalgia). Br Med J 299:365–366
Colquhoun D (1990) Re-anaylsis of clinical trial of homeopathic treatment in fibrositis. Lancet 336:441–442
Bell IR, Lewis DA II, Brooks AJ (2004) Improved clinical status in Fibromyalgia patients treated with individualised homeopathic medicines versus placebo. Rhuematology 43(5):577–582
Bell IR, Lewis DA II, Brooks AJ, Schwartz GE, Lewis SE, Caspi O, Scott A et al (2004) Individual differences in response to randomly assigned active individualized homeopathic and placebo treatment in fibromyalgia: implications of a double-blinded optional crossover design. J Altern Complement Med 10(2):269–283
Relton C, Smith C, Raw J, Walters C, Adelbajo AO, Thomas KJ, Young TA (2009) Healthcare provided by a homeopath as an adjunct to usual care for Fibromyalgia (FMS): results of a pilot randomised controlled trial. Homeopathy 98:77–82
Vithoulkas G (1980) The science of homeopathy. B J Publishers Ltd
Bell IR, Lewis DA II, Lewis SE, Schwartz GE, Caspi O, Brooks AJ et al (2003) EEG alpha sensitization in individualized homeopathic treatment of fibromyalgia. Int J Neurosci 114(9):1195–1220
Bell IR, Lewis DA II, Schwartz GE, Lewis SE, Caspi O, Scott A et al (2004) Electroencephalographic cordance patterns distinguish exceptional clinical responders with fibromyalgia to individualized homeopathic medicines. J Altern Complement Med 10(2):285–299
Cook IA, Leutcher A, Morgan M, Witte E, Stubbeman WF, Abrams M et al (2002) Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 27:120–131
Leuchter AF, Cook IA, Mena I, Dunkin JJ, Cummings JL, Newton TF et al (1994) Assessment of cerebral perfusion using quantitative EEG cordance. Psychiatry Res 55:141–152
Ernst E, Lee MS (2008) A trial design that generates only "positive" results. J Postgrad Med 54(3):214–216
Ernst E, Ted J, Kaptchuk MD (1996) Homeopathy revisited. Arch Intern Med 156(19):2162–2164
Ernst E, Pittler MH (1997) Alternative therapy bias. Nature 385:480
Acknowledgements
There are no conflicts of interest to declare. We would like to thank Helen Coelho with help in designing the study and Leala Watson for administrative assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by grants from The Laing Foundation, Schwabe, Pilkington and GSK
Rights and permissions
About this article
Cite this article
Perry, R., Terry, R. & Ernst, E. A systematic review of homoeopathy for the treatment of fibromyalgia. Clin Rheumatol 29, 457–464 (2010). https://doi.org/10.1007/s10067-009-1361-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-009-1361-2