
Abstract
Hypoxemia has been associated with low bone mineral density (BMD) in animal and human models. We assessed the association of haemoglobin levels with ultrasound-derived (UD) T score, Z score and the stiffness index in all 358 subjects aged 75+ living in Tuscania (Italy). Also, we searched for the haemoglobin cutoff levels that might best identify participants with osteoporosis. In the multivariable linear regression analysis, haemoglobin levels were associated among participants with the UD T score [β = 0.13; 95% confidence interval (CI) = 0.01–0.25; p = 0.030], Z score (β = 0.11; 95% CI = 0.01–0.22; p = 0.045) and stiffness index (β = 1.87; 95% CI = 0.51–3.21; p = 0.007) after adjusting for potential confounders. Haemoglobin levels <140 g/L in men and <130 g/L in women best predicted osteoporosis in linear discriminant analysis. Haemoglobin is independently associated with all UD-BMD parameters. Haemoglobin levels <140 g/L in men and 130 g/L in women might be adopted in clinical practice to identify older subjects in whom screening for osteoporosis might yield higher effectiveness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has been estimated that 1.31 million new hip fractures occurred in 1990. In the same year, the prevalence of hip fractures associated with disability was 4.48 million; 740,000 deaths have been imputed to hip fracture [1]. A threefold increase in incident hip fractures is anticipated within 2030 [2]. In addition, a threefold increase in total direct costs has been documented among patients with hip fracture in the year following the event, as compared with other age-matched subjects [3]. However, apart from hormonal factors, knowledge about the determinants of osteoporosis in older populations is still poor.
Anemia represents a common condition in older populations, which prevalence has been found in about 13% of subjects older than 70 [4]. Noticeably, hypoxemia has been proven to be a risk factor for osteoporosis [5–7]. Several studies have reported on the concurrence of osteoporosis and anemia in selected conditions, such as sickle-cell anemia [8], chronic inflammatory conditions [9] or renal failure [10]. However, available information on the association between haemoglobin levels and osteoporosis in general older populations is scanty [5].
We tested whether haemoglobin levels are associated with bone mineral density in older community-dwelling populations, independently of underlying conditions that might induce both anemia and osteoporosis. Also, we searched for haemoglobin cutoff levels, if any, that might best predict osteoporosis in older subjects.
Patients and methods
Participants
The study involved all subjects, without exclusion criteria, aged 75 or older living in Tuscania (Italy) on January 1, 2004. This town had been selected for a study of the genetic determinants of health status in older populations, along with five other Italian towns. Of the 387 participants enrolled in the site, we excluded 23 subjects with missing data for the study variables and six participants treated with biphosphonates. None of the participating women were on hormonal treatment during the survey. Data were recorded using dedicated software. All participants underwent ambulatory or home visits by the study physicians, who performed detailed physical and anamnestical examination, standard electrocardiography, Doppler echocardiography and bone densitometry, and collected blood samples for serum chemistry and genomic analyses. Also, the study researchers completed a questionnaire which included data on socioeconomic status, lifestyle habits and physical activity, among others. Smoking was considered as total lifetime pack-years for current and former smokers. Alcohol consumption was considered when it consisted of at least two drinks per week. Education was expressed as years of school attendance. Nutritional parameters were collected using a validated questionnaire already adopted for testing large Italian populations [11]. Physical activity was measured using the Physical Activity Scale for the Elderly questionnaire [12]. Participants’ diagnoses and treatments were obtained by their general practitioners before the study visits and further confirmed by the study physicians, who received specific training and whose concordance had been tested using dummy cases. Drugs were coded according to the anatomical, therapeutic and chemical codes [13]. Diagnoses were coded according to the International Classification of Diseases, ninth edition, Clinical Modification codes [14]. Blood samples were obtained in the morning after an overnight fast; after processing, the specimens were aliquoted into cryovials, frozen at −70°C and shipped to the Department of Experimental Pathology, University of Bologna. Measures for interleukin-6 (IL-6) and high-sensitivity C reactive protein (CRP) were obtained from frozen stored plasma and measured in duplicate. IL-6 and CRP plasma levels were measured by enzyme-linked immunosorbent assay kits.
Diagnosis of anemia
Anemia was defined according to the World Health Organization (WHO) criteria: haemoglobin <130 g/L in male and <120 g/L in female participants [15].
Measurement of bone mineral density
As the study enrolled the whole older population of the site, including homebound subjects, a portable instrument was used to assess bone densitometry (Achilles Express, GE Medical Systems, Madison, WI, USA). This validated instrument measures bone density and structure using ultrasound bone densitometry [16]. Ultrasound densitometry enables measurement of the physical properties of bone, specifically bone mineral density. The ultrasound measurement is based on two criteria: the velocity [speed of sound (s), SOS] and frequency attenuation [broadband ultrasound attenuation (dB/MHz), BUA] of sound wave as it travels through the bone [17]. The stiffness is an index combining SOS and BUA, which is calculated by the spread speed of supersonic waves. The formula is (BUA − 50) × 0.671 + (SOS − 1,380) × 0.28. This charts the SOS and BUA into biologically relevant ranges.
According to current WHO recommendations, the ultrasound-derived T score was automatically calculated by the built-in software as the difference between the subject bone mineral density (represented by the stiffness index) and the average density in a reference healthy 30-year-old woman of the same ethnicity, divided by the standard deviation of the reference population [18]. The reference population was derived by the NHANES III study population [19]. According to WHO guidelines, osteoporosis is defined as a T score value of −2.5 or lower, meaning a bone density that is two and a half standard deviations below the mean of a 30-year-old woman. The ultrasound-derived Z score was automatically calculated by normalising the T score for age, as recommended by WHO. The intra-observer and inter-observer correlation coefficients for ultrasound bone densitometry that were analysed during the researchers’ training were 0.73 and 0.68, respectively.
Data analyses
Data of continuous variables are presented as mean values ± SD. Statistical analyses were performed using the SPSS for Windows 13.0 software (Chicago, IL, USA); differences were considered significant at the p < 0.050 level. Analysis of variance (ANOVA) for normally distributed variables in relation to diagnosis of anemia was performed by ANOVA comparisons; otherwise, the nonparametric Kruskal–Wallis H test was adopted. Chi-square analysis was used for dichotomous variables. Haemoglobin was considered as a continuous variable. High-sensitivity CRP and IL-6 were analysed after log transformation.
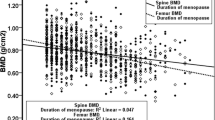
Linear regression analysis was used to estimate the association of variables of interest, including haemoglobin levels, with the ultrasound-derived T score, Z score, and the stiffness index. Linearity of variables was assessed using the ANOVA test of linearity; the linearity assumption was assumed to be satisfied at a p < 0.050 level. To assess independent correlates of bone mineral density, which might confound the association between the ultrasound-derived T score, Z score and the stiffness index with haemoglobin levels, groups of variables (demographics, co-morbid conditions, medications, and objective tests, as shown in Table 1) were first examined in separate age- and sex-adjusted regression models with the simultaneous introduction of covariates (Table 2). Those variables, significant at the p < 0.050 level in these initial models, were simultaneously entered into a summary age- and sex-adjusted regression model (Table 2). In addition, the association between bone mineral density parameters and haemoglobin levels was assessed (Table 3), adjusting for those variables which differed significantly according to diagnosis of anemia (Table 1).
Eventually, linear discriminant analysis was used in separate models to identify haemoglobin levels which best predicted ultrasound-derived T score levels diagnostic of osteoporosis (i.e., <−2.5) in men and women. The Bayesian characteristics of dichotomised haemoglobin levels for identifying osteoporosis were also calculated.
Results
Anemia was detected in 43/358 (12%) participants; osteoporosis was found in 153/358 (43%) participants. The main characteristics of participants, according to diagnosis of anemia, are shown in Table 1. In the three initial linear regression models, age, sex, protein consumption, physical activity scale for the elderly, body mass index and haemoglobin were all associated with indices of bone mineral density at a p < 0.050 level (Table 2). In the final regression models, haemoglobin levels were still associated with the ultrasound-derived T score (β = 0.13; 95% confidence intervals = 0.01–0.25; p = 0.030), Z score (β = 0.11; 95% confidence intervals = 0.01–0.22; p = 0.045) and stiffness index (β = 1.87; 95% confidence intervals = 0.51–3.21; p = 0.007) after simultaneously adjusting for all these potential confounders (Table 2). Also, in the regression model (Table 3) including those variables which were found to differ significantly according to diagnosis of anemia (Table 1), haemoglobin levels were still associated with ultrasound-derived T score (β = 0.23; 95% confidence intervals = 0.09–0.36; p = 0.001), Z score (β = 0.15; 95% confidence intervals = 0.01–0.30; p = 0.039) and stiffness index (β = 2.45; 95% confidence intervals = 0.71–4.20; p = 0.006).
Eventually, the linear discriminant analysis indicated in separate models that haemoglobin levels below 140 g/L in men and 130 g/L in women best predicted (p < 0.0001) participants having ultrasound-derived T score levels <−2.5. Using such cutoff levels, low haemoglobin had 35% sensitivity, 77% specificity, 53% positive predictive value and 61% negative predictive value.
Discussion
The results of the present study indicate that haemoglobin levels are independently associated with all the ultrasonographic bone mineral parameters in unselected, community-dwelling older populations. Also, haemoglobin levels <140 g/L in men and 130 g/L in women might best identify older subjects having ultrasound-derived T score levels <−2.5.
The association of haemoglobin levels with bone mineral density does not represent a mere academic oddity. In fact, several studies have reported that the prevalence and incidence rates of osteoporotic fractures are constantly increasing in Western countries, paralleling the aging of populations [2, 20, 21]. Accordingly, several reports have documented that the mortality rates and the financial burden associated with fractures are currently boosting [3, 22, 23]. In this setting, a threefold increase in total direct costs has been documented among patients with hip fracture in the year following the event, as compared with age-matched subjects without fractures [3].
On the other hand, epidemiological data indicate that anemia is a prevalent condition in older populations, affecting about 13% of subjects aged 70+ [21]. In addition, available data demonstrate that anemia is a powerful risk factor for increased mortality and disability in the elderly [24–26]. This might be partially due to the increased risk of falls [27] because reduced haemoglobin levels have been associated both with decreased muscular strength and poorer physical performance [19, 24–26, 28]. According to these findings, anemia might further increase the risk of fractures in the elderly.
Several conditions characterised by low haemoglobin levels or anemia might also be associated with increased prevalence of bone loss or osteoporosis without any clear cause–effect relationship [9, 10, 29]. However, a study has suggested that anemia might be associated with osteoporosis independently of underlying conditions [30]. Our results support the hypothesis of independent association between low haemoglobin levels and bone mineral density. The role of confounding in this setting is crucial. In fact, several variables, including demographics, lifestyle habits, co-morbid conditions, drug treatment and objective parameters have been associated with bone mineral density in older subjects [31]. To minimise the effect of potential confounders, we built regression models adjusting both for those factors associated with bone mineral density (Table 2) and for variables associated with anemia in the study population (Table 3).
The present study does not allow us to explain the pathophysiology of reduced bone mineral density in participants with low haemoglobin levels. It might be hypothesised that inflammation, frequently found in older subjects, might affect both bone density parameters and haemoglobin levels. In fact, several studies have focused on the role of proinflammatory cytokines in the development of anemia and osteoporosis in older populations [29, 32, 33]. Specifically, healthy elderly present higher circulating levels of IL-6 as compared with younger subjects [34]; this proinflammatory cytokine yields an inhibitory control on haematopoiesis [35].
Indeed, the study previously carried out in an elderly population has suggested that the association between low haemoglobin levels and osteoporosis might be independent of circulating proinflammatory cytokines [30]. In our study, the association between haemoglobin levels and bone mineral density parameters persisted even after adjusting for circulating levels of IL-6 and CRP.
Experimental and clinical studies have rather suggested that hypoxemia might cause osteoporosis [5, 28]. Accordingly, in patients with chronic obstructive pulmonary disease, an independent association between severity of the illness and bone mineral density parameters has been demonstrated [6]. More recently, a study has found an association between left ventricular function and bone mineral density parameters in older women [7]. Thus, hypoxemia might have contributed to the association between low haemoglobin levels and bone mineral density parameters in the present study.
In our study, the association of haemoglobin levels with bone mineral density parameters persisted (Table 3) after adjusting for those variables that differed according to diagnosis of anemia (Table 1). This might be relevant to clinical practice, as it might indicate a potential therapeutic approach to osteoporosis through the correction of low haemoglobin levels. Even independently of such a possible therapeutic approach, the finding of low haemoglobin levels might add to currently acknowledged risk factors for the identification of higher-risk subpopulations for screening purposes. In fact, currently adopted clinical tools for the assessment of increased probability of osteoporosis yield low specificity and positive predictive values, as compared with those associated with low haemoglobin levels in this study [36].
A possible limitation of the study is represented by its cross-sectional design that did not allow us to ascertain any cause–effect relationships. Another limitation is the lack of measurement of serum parathormone and vitamin D levels. Information on sunlight exposure is included in the physical activity scale for the elderly, which mainly explores outdoor activities. The T score cutoff of −2.5 refers to dual-emission X-ray densitometric assay. Indeed, several threshold levels have been proposed for ultrasound measurements. The adoption of the −2.5 cutoff in this study allows lower sensitivity, but higher specificity (> 90%) as compared with other proposed thresholds [37]; this represents a conservative bias that further supports the validity of our results. Noticeably, ultrasound-derived indices of bone mineral density have been found to predict the risk of nonspinal fractures [38].
Independently of its pathophysiological determinants, the finding of increased probability of osteoporosis in older participants, whose haemoglobin levels were below 140 g/L in men and 130 g/L in women, allows us to select subjects with higher pretest probability of osteoporosis in whom screening might yield higher effectiveness.
References
Johnell O, Kanis JA (2004) An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int 15:897–902
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Jarvinen M (1999) Hip fractures in Finland between 1970 and 1997 and predictions for the future. Lancet 353:802–805
Braithwaite RS, Col NF, Wong JB (2003) Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51:364–70
Penninx BW, Pahor M, Woodman RC, Guralnik JM (2006) Anemia in old age is associated with increased mortality and hospitalization. J Gerontol A Biol Sci Med Sci 61:474–479
Fujimoto H, Fujimoto K, Ueda A, Ohata M (1999) Hypoxemia is a risk factor for bone mass loss. J Bone Miner Metab 17:211–216
Karul AB, Karadag F, Yensel N, Altinisik M, Altun C, Cildag O (2003) Should COPD patients be routinely evaluated for bone mineral density? J Bone Miner Metab 21:242–246
Laudisio A, Marzetti E, Antonica L, Cocchi A, Bernabei R, Zuccalà G (2008) Association of left ventricular function with bone mineral density in older women: a population-based study. Calcif Tissue Int 82:27–33
Sarrai M, Duroseau H, D’Augustine J, Moktan S, Bellevue R (2007) Bone mass density in adults with sickle cell disease. Br J Haematol 136:666–672
Gasche C (2000) Complications of inflammatory bowel disease. Hepatogastroenterology 47:49–56
Taal MW, Masud T, Green D, Cassidy MJ (1999) Risk factors for reduced bone density in haemodialysis patients. Nephrol Dial Transplant 14:1922–1928
Gaddi A, Cicero AF, Wani FO, Dormi A, Pasquarelli V, D’Addato S (2001) The realization of a project aimed at reducing the plasmatic lipid level in a large Italian population improves the mean calcium daily intake: the Brisighella Study. Eur J Clin Nutr 55:97–106
Washburn RA, Smith KW, Jette AM, Janney CA (1993) The Physical Activity Scale for the Elderly (PASE): development and evaluation. J Clin Epidemiol 46:153–162
Pahor M, Chrischilles EA, Guralnik JM, Brown SL, Wallace RB, Carbonin P (1994) Drug data coding and analysis in epidemiologic studies. Eur J Clin Epidemiol 10:405–411
PHS–HCFA (1980) International classification of diseases, 9th rev. Public Health Service–Health Care Financing Administration, Washington, DC
World Health Organization. Nutritional Anaemias (1968) Report of a WHO Scientific Group. Technical Report Series No. 405. World Health Organization, Geneva
Krieg MA, Cornuz J, Ruffieux C, Sandini L, Büche D, Dambacher MA, Hartl F, Häuselmann HJ, Kraenzlin M, Lippuner K, Neff M, Pancaldi P, Rizzoli R, Tanzi F, Theiler R, Tyndall A, Wimpfheimer K, Burckhardt P (2003) Comparison of three bone ultrasounds for the discrimination of subjects with and without osteoporotic fractures among 7562 elderly women. J Bone Miner Res 18:1261–1266
Langton CM, Palmer SB, Porter RW (1984) The measurement of broadband ultrasonic attenuation in cancellous bone. Eng Med 13:89–91
WHO scientific group on the prevention and management of osteoporosis (2000) Prevention and management of osteoporosis: report of a WHO scientific group. WHO technical report series, 921 Geneva, WHO Library
Kanis JA, Gluer CC (2000) An update on the diagnosis and assessment of osteoporosis with densitometry. Committee of Scientific Advisors, International Osteoporosis Foundation. Osteoporos Int 11:192–202
Cooper C, Campion G, Melton LJ 3rd (1992) Hip fractures in the elderly: a world-wide projection. Osteoporosis Int 2:285–289
National Center for health statistics (1986) 1985 summary, national hospital discharge survey; advance data from vital and health statistics, n 127. DHHS (PHS) 86–1250. Hyattsville, MD, Sept. 25
Autier P, Haentjens P, Bentin J, Baillon JM, Grivegnée AR, Closon MC, Boonen S (2000) Costs induced by hip fractures: a prospective controlled study in Belgium. Osteoporosis Int 11:373–380
Schousboe JT, Taylor BC, Fink HA, Kane RL, Cummings SR, Orwoll ES, Melton LJ 3rd, Bauer DC, Ensrud KE (2007) Cost-effectiveness of bone densitometry followed by treatment of osteoporosis in older men. JAMA 298:629–637
Penninx BW, Guralnik JM, Onder G, Ferrucci L, Wallace RB, Pahor M (2003) Anemia and decline in physical performance among older persons. Am J Med 115:104–110
Penninx BW, Pahor M, Cesari M, Corsi AM, Woodman RC, Bandinelli S, Guralnik JM, Ferrucci L (2004) Anemia is associated with disability and decreased physical performance and muscle strength in the elderly. J Am Geriatr Soc 52:719–724
Woodman R, Ferrucci L, Guralnik J (2005) Anemia in older adults. Curr Opin Hematol 12:123–128
Penninx BW, Pluijm SM, Lips P, Woodman R, Miedema K, Guralnik JM, Deeg DJ (2005) Late-life anemia is associated with increased risk of recurrent falls. J Am Geriatr Soc 53:2106–2111
Mineo TC, Ambrogi V, Mineo D, Fabbri A, Fabbrini E, Massoud R (2005) Bone mineral density improvement after lung volume reduction surgery for severe emphysema. Chest 127:1960–1966
Leng S, Chaves P, Koenig K, Walston J (2002) Serum interleukin-6 and hemoglobin as physiological correlates in the geriatric syndrome of frailty: a pilot study. J Am Geriatr Soc 50:1268–1271
Cesari M, Pahor M, Lauretani F, Penninx BW, Bartali B, Russo R, Cherubini A, Woodman R, Bandinelli S, Guralnik JM, Ferrucci L (2005) Bone density and hemoglobin levels in older persons: results from the InCHIANTI study. Osteoporos Int 16:691–699
Laudisio A, Marzetti E, Antonica L, Settanni S, Georgakakis I, Bernabei R, Franceschi C, Zuccalà G (2007) Masticatory dysfunction is associated with osteoporosis in older men. J Clin Periodontol 34:964–968
Cauley JA, Danielson ME, Boudreau RM, Forrest KY, Zmuda JM, Pahor M, Tylavsky FA, Cummings SR, Harris TB, Newman AB, Health ABC Study (2007) Inflammatory markers and incident fracture risk in older men and women: the health aging and body composition study. J Bone Miner Res 22:1088–1095
Jilka RL, Hangoc G, Girasole G, Passeri G, Williams DC, Abrams JS, Boyce B, Broxmeyer H, Manolagas SC (1992) Increased osteoclast development after estrogen loss: mediation by interleukin-6. Science 257:88–91
Wieczorowska-Tobis K, Niemir ZI, Podkówka R, Korybalska K, Mossakowska M, Breborowicz A (2006) Can an increased level of circulating IL-8 be a predictor of human longevity. Med Sci Monit 12:CR118–CR121
Baraldi-Junkins CA, Beck AC, Rothstein G (2000) Hematopoieis and cytokines. Relevance to cancer and aging. Hematol Oncol Clin North Am 14:45–61
Skedros JG, Sybrowsky CL, Stoddard GJ (2007) The osteoporosis self-assessment screening tool: a useful tool for the orthopaedic surgeon. J Bone Joint Surg Am 89:765–772
Nayak S, Olkin I, Liu H, Grabe M, Gould MK, Allen IE, Owens DK, Bravata DM (2006) Meta-analysis: accuracy of quantitative ultrasound for identifying patients with osteoporosis. Ann Intern Med 144:832–841
Marín F, González-Macías J, Díez-Pérez A, Palma S, Delgado-Rodríguez M (2006) Relationship between bone quantitative ultrasound and fractures: a meta-analysis. J Bone Miner Res 21:1126–1135
Acknowledgement
This research was partially supported as a “targeted project” (SS9.4.2) by the Italian Ministry of Health.
Ethical standards
The present study was carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. All subjects included in the present study have given written informed consent.
Conflict of interest statement
None of the authors reported any conflicts of interest. All the authors have full control of all primary data and they agree to allow the journal to review their data if requested.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Laudisio, A., Marzetti, E., Pagano, F. et al. Haemoglobin levels are associated with bone mineral density in the elderly: a population-based study. Clin Rheumatol 28, 145–151 (2009). https://doi.org/10.1007/s10067-008-0998-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-008-0998-6