
Abstract
This study aims to examine the long-term articular damage in rheumatoid arthritis (RA) patients according to rheumatoid arthritis articular damage (RAAD) score and to evaluate the parameters correlated with this score. The RAAD score was assessed in 85 RA patients who had the disease for more than 10 years. Patients were divided into three groups according to duration of the disease: group 1, 10–14 years; group 2, 15–19 years; and group 3, more than 20 years. Patients were also divided into three groups according to the time of initiation of treatment with disease-modifying antirheumatic drugs: group A, within the first 2 years, group B, between 2 and 5 years; and group C, after 5 years. We investigated the RAAD score relationship between groups 1, 2, 3; groups A, B, C; sex; drug compliance; age of onset of the disease; and Health Assessment Questionnaire (HAQ). We observed significant differences in RAAD scores according to groups 1, 2, 3 (p<0.01), but not to groups A, B, C; sex; or drug compliance (p>0.05). While the RAAD score correlated well with the HAQ (r=0.560, p<0.001), it did not correlate with the age at onset of the disease (p>0.05). As RA is not a benign disease and articular damage progresses over time, the goal of RA therapy must be to maintain a response before the onset of irreversible damage and loss of function.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Joint damage and disability in rheumatoid arthritis (RA) increase with disease duration, but the nature of their relationship is uncertain. Joint damage progresses constantly over the first 20 years of RA, and the link between damage and disability are strongest in late RA [1].
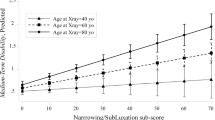
The degree of damage shows the irreversible results of disease activity over time, and joint damage is the most prominent feature of the disease outcome. Although RA is commonly evaluated by radiographs, there are some drawbacks to this technique, among them that damage in soft tissues surrounding the bones and damage in large joints cannot be seen. There have been several attempts to develop a score for irreversible articular damage, based on clinical examination of large and small joints particularly for measuring long-term damage, but until now these have not been widely used. The Rheumatoid Arthritis Articular Damage (RAAD) score was recently developed as a quick and feasible method for measuring the long-term articular damage in large RA populations, and it has been demonstrated to correlate well with the Larsen score with a good interobserver reliability [2]. The maximum total score is 70, with higher scores indicating greater articular damage.
In this study, our objective was to examine the long-term articular damage in RA patients with RAAD score. We further investigated the impact of sex, different initiation times of disease-modifying antirheumatic drug (DMARD) therapy, compliance, age at onset of disease, and Health Assessment Questionnaire (HAQ) on RAAD scores.
Materials and methods
A cross-sectional study was conducted in a hospital that serves individuals with a social security insurance (SSK), provided for blue collar workers and their relatives. The hospital is a tertiary care referral and training center and provides care for those referred from other SSK clinics spread throughout the country, but any patient with an SSK insurance can also be admitted to the hospital without any referral, and this latter group constitutes the majority of the case-mix. The study included all patients consecutively admitted to the Physical Therapy and Rehabilitation Outpatient Clinic between September 2002 and December 2004, if they were fulfilled the 1987 ACR criteria [3] and had a disease duration of more than 10 years.
Data were collected upon admission to the outpatient clinic, using a standard questionnaire and a face-to-face interview. History of disease and drug usage was sought retrospectively.
On the basis of self-report, patients were divided into groups according to: (1) duration of the disease preceding the study onset, as group 1 (10–14 years), group 2 (15–19 years), and group 3 (20 years or longer); and (2) the time of initiation of DMARDs treatment, as group A (in the first 2 years), group B (2–5 years), and group C (5 years after diagnosis).
Patients were divided into three groups according to duration of the disease: group 1, 10–14Vyears; group 2, 15–19 years; and group 3, more than 20 years. They were also divided according to time of initiation of DMARDs treatment: group A, in the first 2 years; group B, between 2 and 5 years; and group C, after 5 years. Information on drugs used was retrospectively sought.
We used RAAD score, which is an easy method for defining articular damage by physical examination; a goniometer was the only required instrument. In this method, 35 joints or joint groups are scored on a three-point scale (0, no irreversible damage; 1, partly damaged; 2, severe damage, ankylosis, or prosthesis). The maximum total score is 70, with higher scores indicating greater articular damage (Table 1) [2]. The same physician who was blinded to the patient history evaluated score.
The HAQ was used to evaluate the physical functioning [4].
Rheumatoid factor (RF) positivity was examined and Ritchie articular index [5] was evaluated.
Compliance was evaluated at every visit, specifically for DMARDs, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticosteroids. The patients were asked to describe their adherence to the prescribed dose and timing according to the scale of “strictly,” “quite,” “not really,” or “not at all.” Patients were considered compliant if they reported that they respected both the dose and the timing of the prescribed medication “strictly” and/or “quite.” All other answers were considered as “noncompliant.” Compliance to drugs was defined if the patient was compliant to the DMARDs, NSAIDs, and corticosteroids.
Analyses included frequency and percent distributions. Kruskal–Wallis test was used in comparison of RAAD score and HAQ score between different disease duration groups and different initiation times of DMARD therapy groups. Multiple comparison test was used to evaluate which group was the cause of difference. Mann–Whitney U test was used in the comparative analyses of RAAD score in different groups of sex, compliance, and initiation time of DMARD therapy. Pearson’s correlation coefficients were assessed to detect the relationship between RAAD scores with HAQ and age of disease onset. Level of statistical significance was accepted as 0.05 throughout the analyses. All analyses were conducted using SPSS for Windows, version 11.0.
Results
Demographic and clinical characteristics of the patients were listed in Table 2.
The three different disease duration groups revealed significantly different results according to RAAD scores (p=0.001). There was a significant difference between group 1 (10–14 years) and group 2 (15–19 years) (p=0.035) and also between group 1 and group 3 (>20 years) (p=0.000). However, we failed to reach statistical significance between group 2 and group 3 (p=0.051).
There were no significant differences in RAAD scores between groups based on sex (p=0.307), time of initiation of DMARD therapy (p=0.814), and drug compliance (p=0.944). The means and statistical differences between RAAD scores and the different parameters are recorded in Table 3.
While RAAD scores demonstrated no correlation with age at onset of the disease (p=0.888), there was a correlation between RAAD scores and HAQ (r=0.560, p=0.000).
The three different disease duration groups also revealed significantly different HAQ scores (p=0.007). There was a significant difference between groups 1 (10–14 years) and 2 (15–19 years) (p=0.024) and between groups 1 and 3 (>20 years) (p=0.002). However, there was no difference between groups 2 and 3 (p=0.400).
Discussion
Rheumatoid arthritis is a chronic disease that causes considerable physical, mental, social, and economic burdens [6]. It affects 1 in 100 individuals in the population and leads to physical, psychosocial, and economical problems [7]. It is a debilitating and progressive disease in which structural joint damage can continue to develop even in the face of symptomatic relief. To have a better quality of life, a reduction in structural damage should also be considered as one of the goals of the therapy in addition to controlling the symptoms and improving the physical function.
Disability may be prominently influenced by large, rather than small, joint damage, as shown in the prospective research from Drossaers-Bakker et al. [8]. X-ray scoring systems need to be refined to assess large joint damage and to be able to separate erosions from markers of joint failure such as total cartilage loss. Moreover, there is a ceiling effect on scores of X-ray damage, in that the scores do not reflect the degree of the damage, highlighting the fact that in late RA disease, the interaction between joint damage and disability cannot be fully explained using the current methods. To better evaluate the joint failure, new scoring methods are needed [9]. Attempts to design a clinical damage score in RA have been published before, but until now, these have not been widely used. In this study, we used the currently designed RAAD score to define the late effects of the disease in assessing damage. It is an easy and quick evaluation method for outpatient practice [2].
Cohort studies of RA patients attending specialist clinics with varying disease durations have shown highly significant correlations between disease duration and joint damage [1, 10]. Scott et al. [1], concluded in his review that joint damage assessed by radiological scores in cohorts of RA patients treated with conventional antirheumatic drugs is less than 10% of possible maximum of highest Larsen or Sharp score in early RA, rising to 40% of possible maximum by 20 years. Furthermore, the average annual increase in damage, as determined by Scott, was 1.6–1.9% of the possible maximum. In the current study, we found results parallel to Zijlstra et al. [2] in disease duration. This result emphasizes the time effect of the disease. There is a question whether the rate of progression decreases as the disease duration increases. Larsen and Thoen [11] found that the rate of increase slowed down later in the disease and the Larsen score fell. Wolfe and Sharp [12] reported that the rate of progression was constant over a 19-year follow-up. In the current study, we showed that the patients who had RA for more than 20 years had no more structural damage or disability than the patients with RA for 15–19 years. Our view is that articular damage did not demonstrate progression after 19 years of the disease.
There have been contradictory results regarding sex prevalence during the course of RA. Some studies have suggested that males may follow a much more severe course [13], whereas others have shown that females experience a more severe course [14]. In the current study, there was no sex predilection regarding degree of articular damage.
Studies in patients with RA who were diagnosed within 2 years of the onset of symptoms showed that early use of DMARDs was preferable to delayed treatment in terms of radiographic progression [15, 16]. We evaluated the patients divided into three groups with respect to the time of onset of DMARD therapy and found no correlation between the RAAD score and time of therapy onset. We showed that neither early nor delayed initiation of DMARD therapy affected the long-term articular damage. This may be related to the fact that traditionally used DMARDs have limitations that may impinge on potential efficacy. Two factors limiting the long-term efficacy of traditional DMARDs are waning response during long-term therapy and poorly tolerated adverse events; the effects of commonly used DMARDs on radiographic progression of RA were often minimal [17]. Although in the current study the duration and dose of the therapies were not standardized, we can conclude that the current DMARD therapies may not be as effective in decreasing the articular damage as expected.
Lee and Tan [18] found no significant difference in erosions between the compliant and noncompliant group. To our knowledge, there is no report evaluating the correlation between compliance and articular damage. In this study, we showed that there was no correlation between these parameters. Despite patient compliance to their drug therapies, articular damage still developed in our cohort.
Prognostic markers for progressive joint damage and disability have been extensively reviewed. Sociodemographic markers such as older age at onset are associated with poor prognosis [13]. Gradual noticed onset of the disease after 40 years was a predictor of disease progression [19]. However, Skoumal and Wottawa [20] divided patients according to age at onset of the disease, and they found no statistically significant difference in radiological progression and clinical scores. We also were unable to determine a correlation between the RAAD scores and age at onset.
As disease duration increases, the correlation between damage and disability becomes more obvious [21]. In the early disease, the HAQ score shows that loss of functional capacity is caused mainly by disease activity, while later in the disease course, destruction may be the main determinant [8]. Bakker et al. [22] found that the Sharp score initially showed only a weak correlation with HAQ; however, by the 12th year there was a much stronger correlation. In our study, the HAQ score correlated well with the articular damage score, which was consistent with the earlier reports [2]. Disability worsens over the course of RA [23].
Both the HAQ and articular damage scores were significantly worse in patients with 15 to 19 years of disease when compared to those with 10 to 15 years of disease, but no significant difference in either score was observed between patients with 20 years of disease vs those with disease duration of 15 to 19 years. These observations support that the progression of the disease is greater in the first 19 years.
In this study, we observed that the articular damage increased with disease duration in late RA patients. Initiation time of DMARD therapy, sex, compliance to drugs, and age at onset of disease had no effect on articular damage. RA is not a benign disease and may progress over time even in the presence of DMARDs. The ultimate goal of RA therapy is to maintain a response and a state of remission as early in the disease process as possible, before the onset of irreversible damage and loss of function. To achieve such goals, drugs that effectively and rapidly block inflammation and joint destruction, but are not limited by waning long-term responses, serious toxicities, or adverse events that detract from quality of life, are required.
References
Scott DL, Pugner K, Kaarela K et al (2000) The links between joint damage and disability in rheumatoid arthritis. Rheumatology 39:122–132
Zijlstra TR, Moens HJ, Bukhari MAS (2002) The rheumatoid arthritis articular damage score: first steps in developing a clinical index of long term damage in RA. Ann Rheum Dis 61:20–23
Arnett FC, Edworthy SM, Bloch DA et al (1998) The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31:315–324
Pincus T, Summey JA, Soraci SAJ et al (1983) Assessment of patient satisfaction in activities of daily living using a modified Stanford Health Assessment Questionnaire. Arthritis Rheum 26:1346–1353
Ritchie DM, Boyle JA, McInnes JM et al (1968) Clinical studies with an articular index for the assessment of joint tenderness in patients with rheumatoid arthritis. Q J Med 37:393–406
Lubeck DP (2004) Patient reported outcomes and their role in the assessment of rheumatoid arthritis. Pharmacoeconomics 22(suppl 1):13–26
Harris ED Jr (1989) The clinical features of rheumatoid arthritis. In: Kelley WN, Harris ED Jr, Ruddy S, Sledge CB (eds) Textbook of rheumatology. Saunders, Philadelphia, PA, pp 943–981
Drossaers-Bakker KW, Kroon HM, Zwinderman AH et al (2000) Radiographic damage of large joints in long-term rheumatoid arthritis and its relation to function. Rheumatology 39:998–1003
Scott DL, Smith C, Kingsley G (2003) Joint damage and disability in rheumatoid arthritis: an updated systematic review. Clin Exp Rheumatol 21:20–27
Li C, Scott DL, Deodhar A et al (1999) Radiological gradients and predicting the progression of rheumatoid arthritis. Ann Rheum Dis 58(suppl):97
Larsen A, Thoen J (1987) Hand radiography of 200 patients with rheumatoid arthritis repeated after an interval of one year. Scand J Rheumatol 16:395–401
Wolfe F, Sharp JT (1998) Radiologic outcome of recent onset rheumatoid arthritis. Arthritis Rheum 41:1571–1582
van Riel PLCM, Wijnands MJH, van de Putte LBA (1998) Evaluation and management of active inflammatory disease. In: Klippel JH, Dieppe PA (eds) Rheumatology, 2nd edn. Mosby, London, pp 14.1–14.12
Thompson PW, Pegley FS (1991) A comparison of disability measured by the Standford Health Assessment Questionnaire disability scales (HAQ) in male and female rheumatoid outpatients. Br J Rheumatol 30:298–300
Egsmose C, Lund B, Borg G et al (1995) Patients with rheumatoid arthritis benefit from early 2nd line therapy: 5 year follow up of a prospective double blind placebo controlled study. J Rheumatol 22:2208–2213
Van der Heide A, Jacobs JW, Bijlsma JW et al (1996) The effectiveness of early treatment with “second line” antirheumatic drugs. A randomised, controlled trial. Ann Intern Med 124:699–707
Scott DL (2004) Pursuit of optimal outcomes in rheumatoid arthritis. Pharmacoeconomics 22:13–26
Lee P, Tan WP (1979) Drug compliance in outpatients with rheumatoid arthritis. Aust N Z J Med 9:274–277
Gradual N (2004) The natural history and prognosis of rheumatoid arthritis: association of radiographic outcome with process variables, joint motion and immune proteins. Scand J Rheumatol 33:1–37
Skoumal M, Wottawa A (2002) Long term observation study of Austrian patients with rheumatoid arthritis. Acta Med Austriaca 29:52–56
Welsing PM, Van Gestel AM, Swýnkels HL et al (2001) The relationship between disease activity, joint destruction and functional capacity over the course of rheumatoid arthritis. Arthritis Rheum 44:2009–2017
Bakker KW, Amesz E, van Zeben D et al (1998) Long term outcome in rheumatoid arthritis: destruction versus disability. Br J Rheumatol 37:85
Pollard Z, Choy EH, Scott DL (2005) The consequences of rheumatoid arthritis: Quality of life measures in the individual patient. Clin Exp Rheumatol 23(suppl 9):S43–S52
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Eksioglu, E., Tuncay, R., Gurcay, E. et al. Articular damage in late rheumatoid arthritis. Clin Rheumatol 26, 314–318 (2007). https://doi.org/10.1007/s10067-006-0293-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-006-0293-3